
Abstract
Purpose:
To describe a clinical case of corneoscleral xanthogranuloma, a rare manifestation of juvenile xanthogranuloma, and xanthoma disseminatum, which responded well to chemotherapy.
Methods:
Interventional case report and literature search.
Results:
A 9-year-old female patient with a disseminated disease showed complete regression of her corneoscleral xanthogranuloma with methotrexate and azathioprine therapy.
Conclusion:
Since they are potentially blinding, corneoscleral xanthogranulomas are commonly surgically excised. While surgical resection has been widely advocated in the literature, immunosuppressive therapy alone may be a pertinent management line of corneoscleral xanthogranuloma, especially with systemic involvement.
Introduction
Xanthoma disseminatum (XD) is a rare, non-inherited, benign disorder that belongs to the spectrum of non-Langerhans cell histiocytoses (non-LCH). It is characterized by aberrant collections of histiocytes with subsequent intracellular deposition of lipids in otherwise non-dyslipidemic patients, leading to widespread formation of xanthomas. 1 While XD is known primarily as a mucocutaneous disorder, additional organs may be affected. For example, up to 40% of XD patients develop diabetes insipidus secondary to the central nervous system (CNS) involvement. 1 The disease has a benign course, and thus, can be managed conservatively. However, since ocular involvement may lead to sight-threatening complications, active treatment may become necessary. 2 Attempts to treat corneoscleral xanthogranulomas included topical steroids, angiogenesis inhibitors, immunosuppressive therapy, radiation, and surgical excision with or without lamellar keratoplasty.2–4 Although several reports advocated the surgical approach,2,5 no clear evidence exists to support any particular treatment modality. We report herein a XD patient with limbal xanthogranuloma showing complete remission after treatment with methotrexate and azathioprine.
Case description
A 9-year-old female presented to our service with a 1-month history of yellow-to-brown lesion on the left eye. She had no other ocular complaints. During the year prior to presentation, she had had numerous periorbital skin eruptions that progressively spread to the chin, neck, torso, and upper extremities. She also experienced polydipsia and polyuria and was diagnosed with central diabetes insipidus, for which she was treated with desmopressin. External examination revealed miliary xanthomatous skin papules, measuring 1–4 mm in maximum dimensions, of high density in the periorbital area (Figure 1). The skin lesions were also widely distributed over the scalp, face, neck, chest, axillae, abdomen, back, and flexural aspects of the upper and lower extremities. No mucosal lesions or lymphadenopathy were noted. Biomicroscopic examination showed a 1.8 × 1.9 mm2 elevated, smooth nodule with yellow-tinged center and salmon-colored vascular periphery involving the corneoscleral limbus at 1 o’clock position (Figure 2). The uncorrected visual acuity was 20/20-1 in both eyes. The visual field, pupils, extraocular muscles, and intraocular pressure were within normal limits bilaterally. A skin biopsy showed granulomatous infiltrates consisting of epithelioid histiocytes with bland nuclei and abundant amphophilic cytoplasm. Scattered Touton giant cells, lymphocytes, and eosinophils were also present. These histological findings were suggestive of xanthoma. Given the progressive, diffuse distribution of the lesions, the slit-lamp appearance of the limboscleral lesion, and the presence of diabetes insipidus, the presumptive diagnosis of XD with ocular and CNS involvement was made.
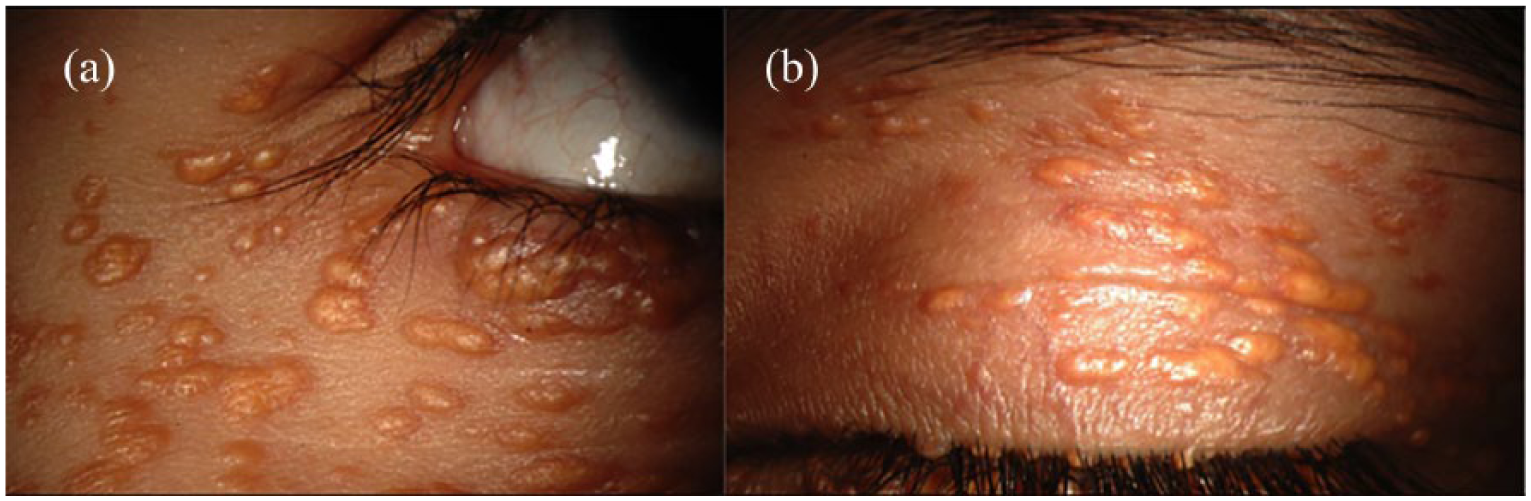
Multiple tan-orange papulonodular skin eruptions several millimeters in size distributed over the periorbital area. Coalescence of the lesions (a) and involvement of the lid margin (b) can be also seen.
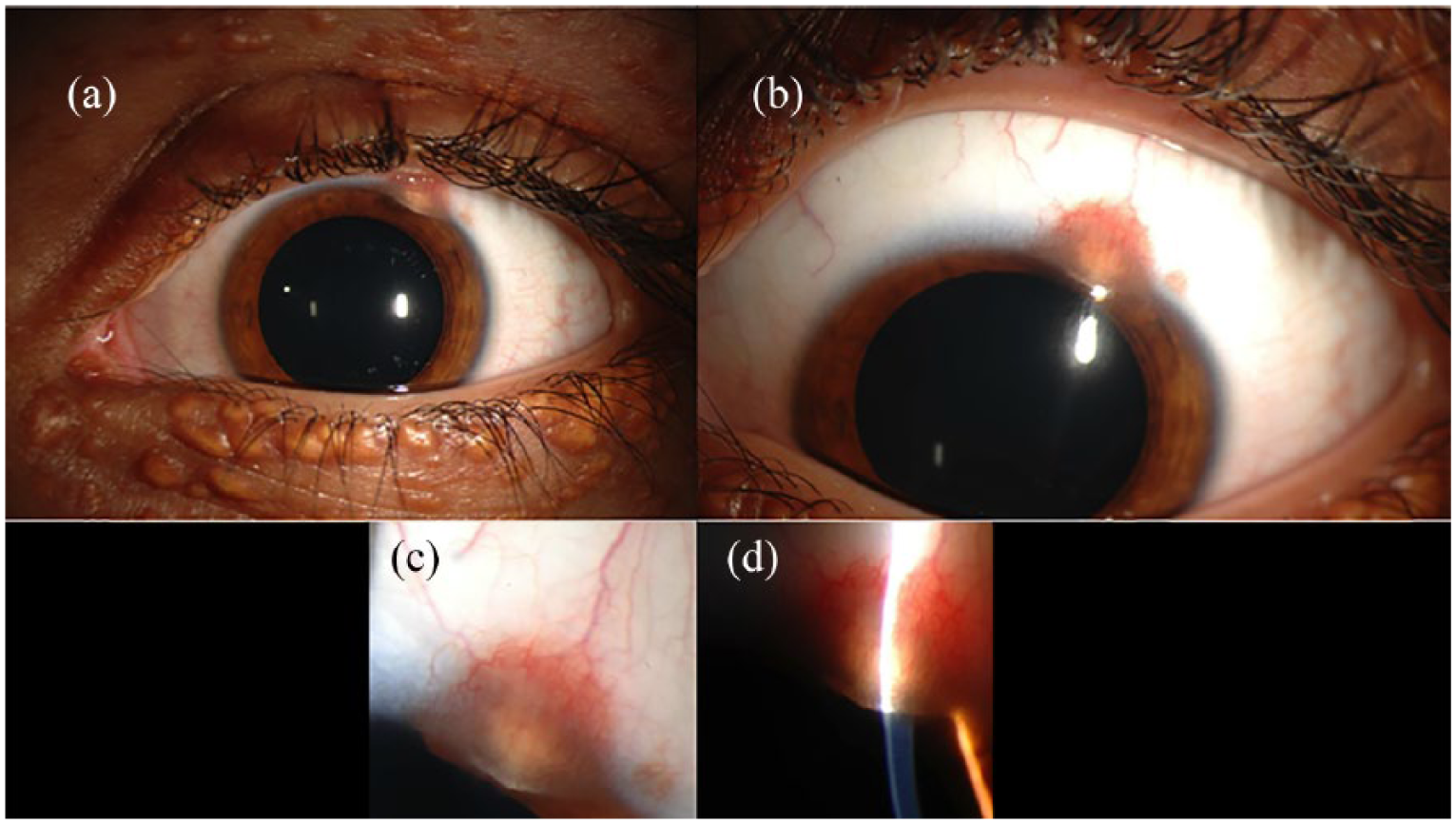
Wide-beam (a, b, and c) and slit-beam (d) biomicroscopy showing an elevated, smooth nodule with yellow-tinged center and salmon-colored vascular periphery involving the supero-temporal limbal area.
Over the next 2 month, the corneoscleral xanthogranuloma increased in size to 2.5 × 2.5 mm2 but remained stable thereafter. Given the extensive cutaneous and systemic disease, chemotherapy was initiated with LCH-based regimen, which included 6 week vinblastine 6 mg/m2/dose on the first day of each of the 6 weeks and prednisolone at 40 mg/m2/day given in 3 days for 4 weeks and then tapered over 2 weeks. Unfortunately, the xanthomatous lesions increased in size and number. Therefore, she was started on 6-mercaptopurine 50 mg/m2/day and methotrexate 10 mg/m2/week. The lesions showed relative improvement during the following 2 weeks, and the dose of 6-mercaptopurine was increased to 75 mg/m2/day but reduced later to 50 mg/m2/day due to the intolerable gastrointestinal side effects. One year after the initiation of the treatment, the limbal xanthogranuloma appeared to have flattened. The skin lesions continued to improve during the following 2 years, until complete resolution was achieved. Chemotherapy was stopped. On her last follow-up, the eyelid xanthomas and the corneoscleral lesion completely regressed with residual scarring (Figure 3). However, she remained to have symptomatic diabetes insipidus with medical management.
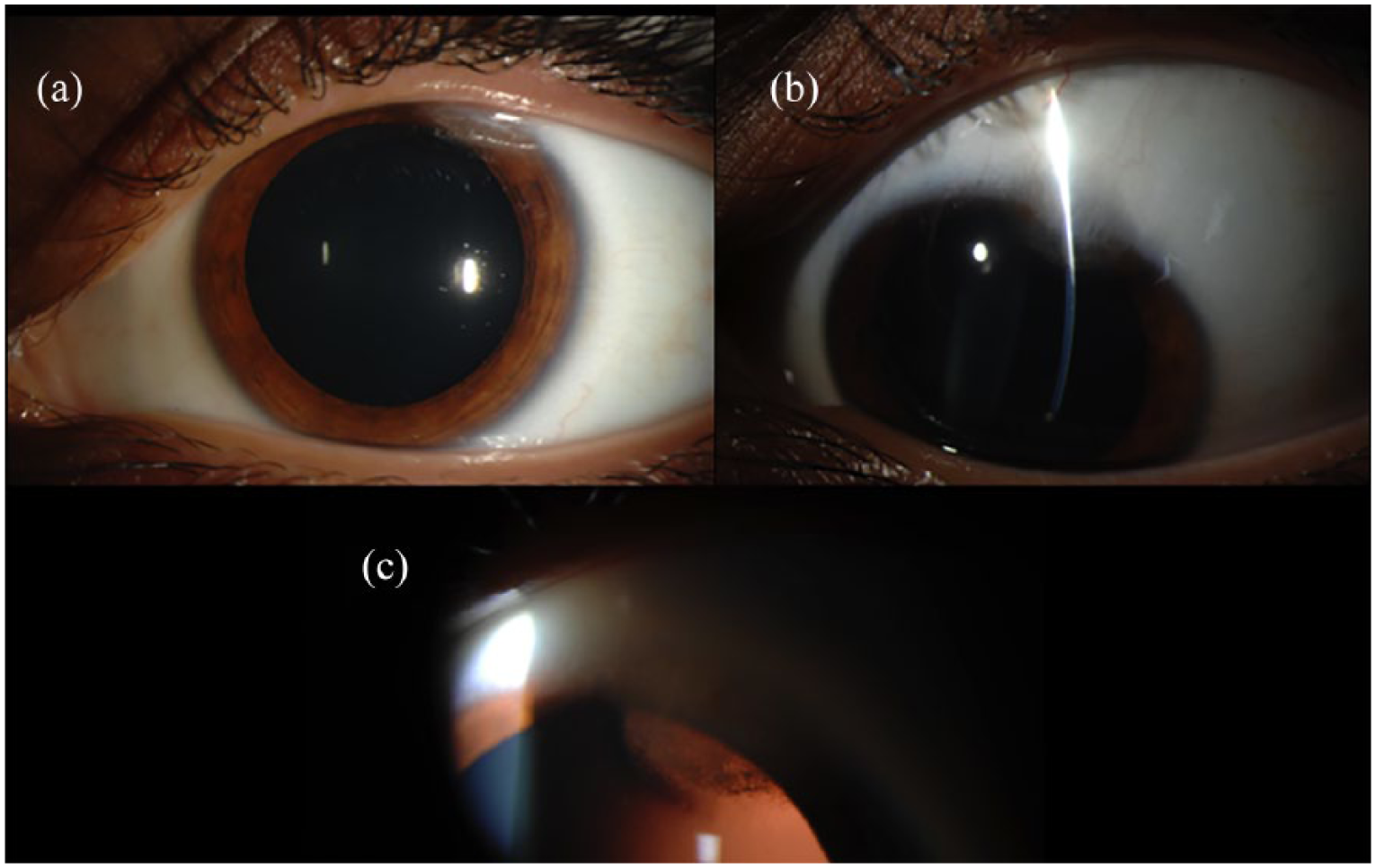
Slit-lamp biomicroscopy showing the resolution of the limbal lesion after systemic chemotherapy (a and b). Healing scar tissue can be seen using the direct (b) and retro-illumination (c).
Discussion
XD is a systemic disease with a seemingly sporadic occurrence. 1 While the proliferation of histiocytes is well documented as part of its pathogenesis, whether this process is neoplastic or reactive remains largely unknown. The disease course is typically benign but may cause significant morbidity and possibly mortality when involving critical structures. Ocular xanthogranuloma can cause a wide variety of problems, from lid disfiguration to corneal and trabecular meshwork infiltration, hyphema, and secondary glaucoma. 6 Indeed, blindness is a possible outcome. 7 In addition, while cutaneous xanthogranuloma may resolve, ocular xanthogranulomas are less likely to show spontaneous remission.2,5 This may have accounted for the common inclination to favor surgical treatment over other less invasive approaches.2,5
Overall, xanthogranulomatous lesions rarely affect the corneoscleral limbus. Chaudhry et al. 8 and later Kontos et al. 2 have identified a total of 27 pediatric cases of limbal xanthogranuloma in the literature since it was first reported by Cogan et al. in 1958. To our knowledge, no additional cases have been reported after Kontos et al.’s review. Of the reported cases, 25 (92.6%) were treated surgically with excisional biopsy or total excision. Ashmore et al. 3 reported resolution of corneal xanthogranuloma with topical steroid regimen of loteprednol etabonate every 2 h and fluorometholone ointment nightly in a 4-month-old infant. Longmuir et al. 9 reported a 14-month-old case treated with methotrexate, whose attempt to taper the medication dose resulted in a relapse. In our case, the patient was weaned off both methotrexate and azathioprine without any recurrence or complication. Whether such response is dependent on the patient’s age group remains to be identified.
A potential advantage of surgical excision is that it allows for histological examination of the lesion. This may be important in cases of solitary corneoscleral lesions with no systemic disease or with atypical presentations.5,10 If a confirmatory diagnosis is needed but surgical excision is to be deferred, fine needle aspiration can be used as an alternative. 11 Indeed, since topical treatment can be effective in some cases, it may be a reasonable starting point if no sight-threatening or severe symptoms are present. 3 In the presented case, systemic disease was evident at presentation with CNS, ocular and extensive cutaneous involvement. As such, systemic therapy was necessary. Meanwhile, the patient’s vision was not affected, and the lesion seemed to have stabilized on subsequent follow-up visits. Since such findings are re-assuring, the deferral of surgical excision and the initiation of systemic therapy are clinically justified and may be deemed sufficient for the management of corneoscleral xanthogranulomas in the presence of systemic disease.
In short, chemotherapy is a pertinent management line of corneoscleral xanthogranuloma, especially with systemic involvement. Absence of visual disturbances at presentation, as well as stability of the lesion’s size and position over the disease course, may be reasonable indications for non-surgical ocular management. Although surgical excision may be preferred for solitary lesions, cosmesis or symptomatic deterioration, immunosuppressive agents, such as azathioprine and methotrexate, may be indicated and prove effective for patients with disseminated disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.