
Abstract
Introduction:
Amblyopia is speculated to be an untreatable disease in the patient, who is beyond the critical period of vision; however, currently, it is treatable in adults.
Purpose:
This study aimed to elucidate whether the treatment is useful in both anisometropic amblyopia and strabismic amblyopia. In addition, the differences were detected between anisometropic amblyopia and strabismic amblyopia after the same perceptual treatment and whether the suppression in anisometropic amblyopia or strabismic amblyopia could be decreased before and after the treatment.
Methods:
A binocular perceptual learning was applied for the treatment, the suppression was measured, and the patients were followed up for 2 months after training. Anisometropic amblyopia and strabismic amblyopia groups were subjected to the assessment of stereo, visual acuity, contrast sensitivity, and suppression before and after the training.
Results:
After 6 weeks of “Diploma Gabor Orientation Coherence” training, in the anisometropic amblyopia group, the outcomes of visual acuity (t = 3.114, p = 0.026) and contrast sensitivity (t = 7.786, p = 0.001) were increased significantly. While in the strabismic amblyopia group, the outcomes of stereo (t = 2.987, p = 0.040) and contrast sensitivity (t = 3.638, p = 0.022) were increased significantly.
Conclusion:
After Diploma Gabor Orientation Coherence training in the same frequency and in the same duration, the anisometropic amblyopia group got an improvement in visual acuity, but the strabismic amblyopia group got an improvement in stereo. As there are evidences to show that anisometropic amblyopia and strabismic amblyopia were injured in different pathways, we think the diverse results might come from the different pathway injury in anisometropic amblyopia and strabismic amblyopia.
Keywords
Introduction
Amblyopia is the primary cause of monocular low vision in preschool and school children, which can be an unusual experience in the visual sensitive period (due to anisometropia, deprivation, or strabismus). Although the conventional therapy might be effective in childhood, 15%–50% is yet untreatable. 1 Adult amblyopia is difficult to treat and a clinical issue. Nevertheless, recent studies on amblyopia mechanism and therapy have shown some improvements with considerable progress in adult amblyopia treatment.2–4
Visual plasticity is the ability of the visual system to alter its responses according to the changes in the visual input. Previously, amblyopia was untreatable in children or adults, who were beyond the critical period of visual cortex development. 5 However, recent evidence on plasticity in children or adults’ visual system has demonstrated that training in specific visual tasks might improve the performance or sensitivity.6–8 As the reserve of plasticity was observed in amblyopic eyes (AEs) in adults, the improvements in the training were varied and difficult to explicate. Finally, a theory proposed an imbalance during the AE and the fellow eye (FE) that might be ascribed to the inhibition to the binocular emulation.9–11
The basic process of binocular inhibition occurs not only in patients with amblyopia but also in normal individuals; however, it is maintained at a specific equilibrium only in normal individuals. Consequently, the disrupted balance leads to a disadvantage in one eye (suppression), causing amblyopia. 12 Thus, the disinhibition treatment was established that utilized the common method of binocular perceptual learning treatment. Simmers and Gray 13 successfully used the perceptual learning treatment as an approach to therapy in adult amblyopia and obtained an effective result. Nonetheless, several investigators employed a variety of visual tasks; the adult visual system can change according to the behavioral demands.14,15 A majority of the results of these studies neither distinguished strabismic amblyopia (SA) and anisometropic amblyopia (AA) nor measured the suppression before or after training.
Previous studies have shown several differences between SA and AA: different scotoma, different content of GABA (γ-aminobutyric acid), and different injury in the cellular pathway with respect to color, shape, and motion.16–18 Thus, first, we should distinguish between amblyopia, and then, suppression from FE to AE should be measured before and after treatment as it is a critical initiation factor. Until 2013, Hess and colleagues19,20 used a “Gabors” model to quantify suppression, which showed satisfactory repeatability and stability. Some studies indicated that different types of amblyopia might be injured in different cellular pathways. For example, Kawabata and Adachi-Usami et al. 21 reported that the amblyopic visual cortex has a normal complement of cells but reduced spatial resolution and a disordered topographical map. Changes occurring in the late sensitive period selectively impact the parvocellular pathway (PP). So in this study, we measured the suppression between AE and FE and distinguished the parvocellular pathway (PP) and magnocellular pathway (MP).
In this study, we applied binocular perceptual learning treatment as our treatment strategy, measured the suppression stringently, and the participants were followed up for 2 months after training. In addition, whether our treatment was useful in both SA and AA was also evaluated. Furthermore, the potential differences after the same perceptual treatment in SA and AA and whether the suppression in SA and AA could be decreased before and after treatment were also analyzed.
Methods
Participants
This study was approved by the Institutional Review Board of Eye and ENT Hospital of Fudan University, and all participants provided written informed consent in accordance with the Declaration of Helsinki (2008).
A total of 24 adults (21.324 ± 4.113,
Two of our patients got monocular deprivation treatment, but both of these patients had abandoned monocular deprivation treatment 2 years or more before joining in our study. These participants were divided into two groups (12 in each group): AA and SA groups. Both groups received the binocular approach of the orientation perception. During training, one of the participants in the SA group quit, while none in the AA group withdrew (the total loss in the follow-up rate was 4.17%).
Diploma Gabor Orientation Coherence training paradigm
Stimuli
In this test, we employed a linearized 1700 cathode ray tube displayer screen (Philips 107S61, Amsterdam, Netherlands; refresh rate = 60 Hz, mean luminance 200 cd/m2) at a viewing distance of 100 cm with the uniform field luminance of 5 cd/m2 in a semi-dark room as a monitor. Stimuli were generated and controlled by MATLAB (MathWorks Inc., USA) using Psychtoolbox on an ACER computer and displayed on the monitor. The dichoptic presentation used a Wheatstone stereoscope. The luminance contrast (including the following tests) was specified as Michelson contrasts [C = (Imax – Imin)/(Imax + Imin)]. The global orientation stimuli consisted of 100 Gabor patches presented in the binocular black rectangular frame (15° × 15°). Two short fixation lines were presented in each eye surrounding the frames that helped the participants to obtain binocular fusion easily. The individual Gabor patch was 1° with a spatial frequency of 2 cycles/°. These Gabor patches were presented in two types: regular orientation dots (“signals”) that were shown on the screen with the same orientation (“±5°” jitter around horizontal/vertical) and non-directional dots (“noise”) that were shown on the screen with random orientations. The spatial distributions and orientations of Gabor patches were random across trials (Picture 1).
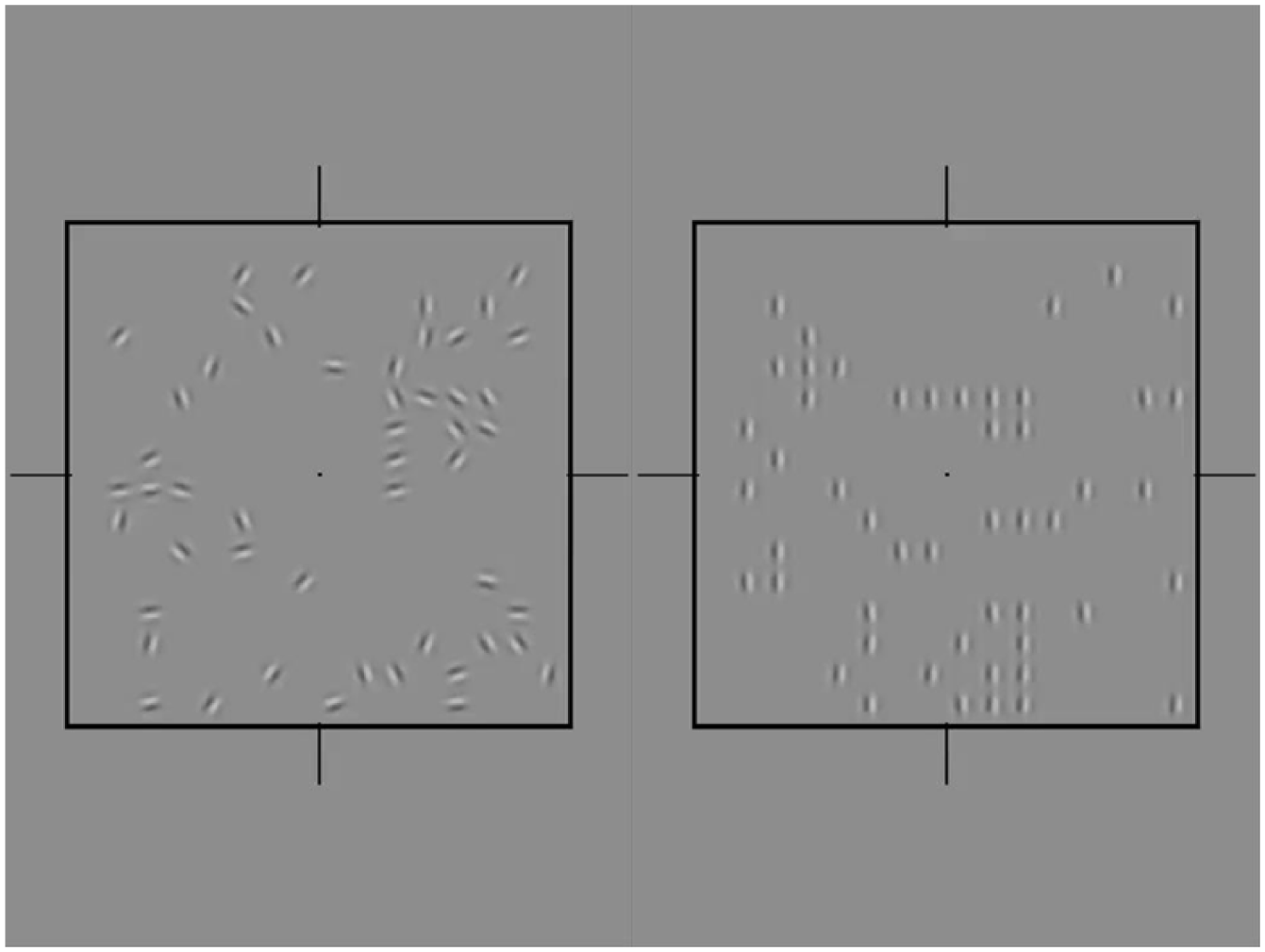
The left picture shows 50% signal dots, and the right picture shows 50% noise dots in DGOC training. The participant has to decide the dots’ correct orientation (horizontal or vertical) in the fused image.
Procedure
Before training, the participants were asked to complete a frame alignment task to acquire two eyes fusion. The signal Gabor stimuli were presented in AE with 100% luminance contrast, while the luminance contrast of noise Gabor stimuli in FE was modified (10%, 30%, 50%, 70%, 90%, and 100%) in different runs in a random sequence. In each trial, the global orientation stimuli were presented for 200 ms, and the subjects instructed to respond to the signal patches’ orientation (vertical or horizontal) using a keyboard. The signal patch number in AE was adjusted by a 3-down-1-up staircase (79% correct performance) with a step size of 10%. The staircase was terminated at the eighth reversal and the coherent threshold, and the proportion of signal Gabor patches was calculated as the mean of the last four reversals. Our participants insisted 6 weeks’ training with 3 times/week.
Stereopsis and visual acuity measurements
Titmus stereopsis at 40 cm viewing distance was used to assess stereopsis, while all participants were forbidden to undergo pupil dilation before the completion of this test. Visual acuity was tested using a logMAR chart with 0.1 logMAR steps, viewed from a distance of 4 m with refraction best corrected and without the drug for pupil dilation.
Contrast sensitivity at high spatial frequency
Contrast sensitivity was assessed at a high spatial frequency of 1 c/d, using a two-alternative, forced-choice method. A double brief sound in double “Doo” was coupled with the display of Gabor patches; the participants had to judge the display of Gabor patches as first or second, and the interval was 1 s. Under the guidance of someone familiar with the procedure, the participants completed a threshold measurement. 50% accurate thresholds were estimated for each measurement using a Bayesian adaptive staircase run over a maximum of 50 trials, which generated data that were fit by a Weibull function. The program was executed by MATLAB (2013); the condition of this test was the same as above (section “Stimuli”).
Measurement of suppression
Motion coherence threshold
Two classical approaches have been reported to quantify the binocular suppression: Diploma Gabor Orientation Coherence (DGOC) and dichoptic global motion coherence (DGMC). 7 The DGMC paradigm is similar to dichoptic global orientation coherent paradigm in our training part (section “Diploma Gabor Orientation Coherence training paradigm”), except moving dots instead of orientation Gabor patches. “Signal” dots moved in the same direction (vertically or horizontally), while “noise” dots moved in random directions. Both the signal and noise dots moved at the speed of 3.36°/s. At the beginning of each motion sequence, the position of each dot was assigned randomly. Each dot had a limited lifetime to prevent the subjects from tracking individual dots, and a new dot emerged at a random location when a specific dot reached its limited lifetime. When a dot reached the edge of the rectangular frame, it was immediately re-plotted in a random position within the frame. The number of signal dots in AE was adjusted by a 3-down-1-up staircase (79% correct performance) with a step size of 10%. 14 The staircase was terminated at the eighth reversal and the coherent threshold, and the proportion of signal moving dots was calculated as the mean of the last four reversals (Picture 2). In addition, we selected this DGMC paradigm as an indicator of binocular suppression status before and after training.
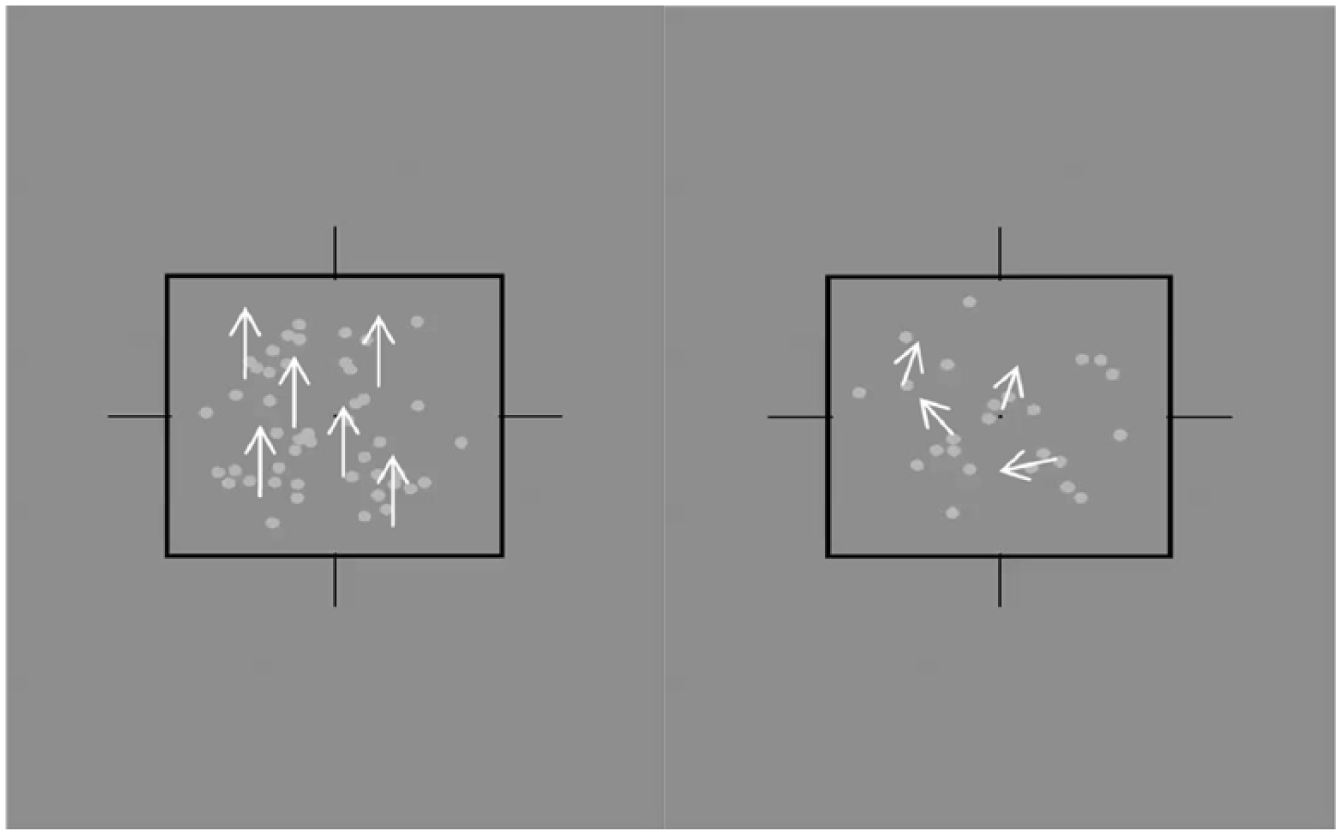
The left picture shows 50% signal dots, and the right picture shows 50% noise dots in the estimation of suppression of motion coherence threshold. The participant has to decide whether the dot is moving up or down in the fused image.
Dichoptic global coherence
First, the signals were shown to AE in contrast to FE from 10% to 100%, following which the signal shifted to FE. Moreover, the dots presented to AE were maintained at 100%, and we only modified the contrast of the dots shown to FE. The coherence thresholds versus interocular contrast ratio curves (TvRs) were fitted using “non-linear curve fit” by Gaussian Fitting in Origin 9.0 software using the fitting formula (1), wherein the x-coordinate of the intersection point (balance point) served as the dichoptic global coherence (the quantification of suppression)

Results
A total of 24 participants were recruited in this study (Table 1) and baseline data
The participants were divided into anisometropia amblyopia group (AA) and strabismus amblyopia group (SA).
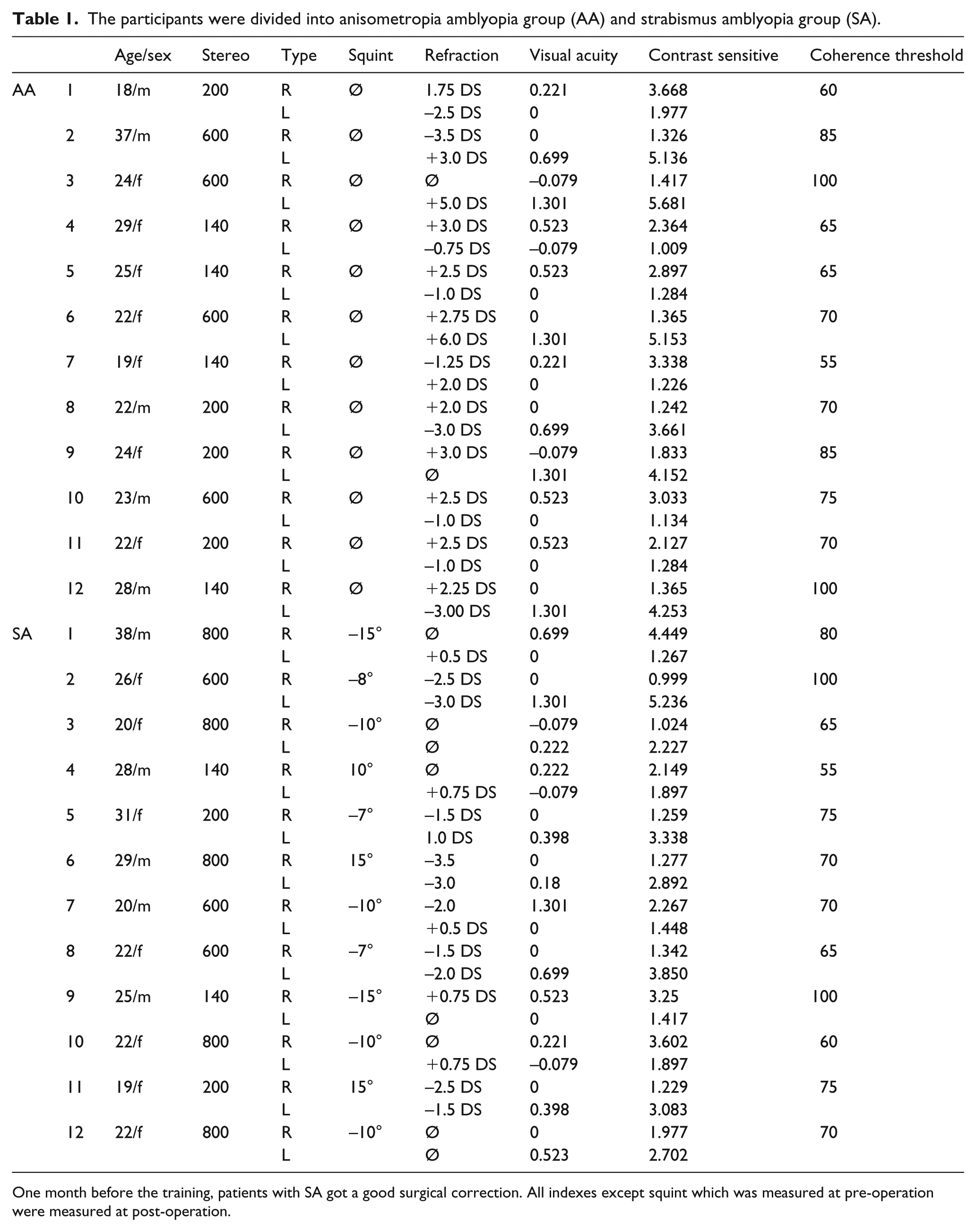
One month before the training, patients with SA got a good surgical correction. All indexes except squint which was measured at pre-operation were measured at post-operation.
After 6 weeks of DGOC training in the AA group (Figure 1), the outcomes of visual acuity (t = 3.114, p = 0.026) and contrast sensitivity (t = 7.786, p = 0.001) were increased significantly, and the outcome of motion coherent threshold was also decreased (t = 8.510, p < 0.001). The outcome of visual acuity (t = 3.097, p = 0.027), contrast sensitivity (t = 8.909, p < 0.001), and coherence threshold (t = 7.006, p < 0.001) showed significant differences between pre-training and 2 months after the end of training, while no significant difference was observed in the outcomes of visual acuity, contrast sensitivity, and motion coherence threshold between 2 months after the end of training and the end of training (6 weeks). In the SA group (Figure 2), the outcomes of stereo (t = 2.987, p = 0.040) and contrast sensitivity (t = 3.638, p = 0.022) were increased significantly in 6 weeks after training as compared to that before training. Moreover, the outcome of motion coherent threshold was decreased (t = 3.882, p = 0.018). The outcome of stereo (t = 2.987, p = 0.040), contrast sensitivity (t = 4.587, p = 0.010), and coherence threshold (t = 3.354, p = 0.028) showed statistically significant differences between pre-training and 2 months after the end of training, while any significant difference was not detected in the outcome of stereo, visual acuity, contrast sensitivity, and motion coherence threshold between 2 months after the end of training and the end of training (6 weeks).
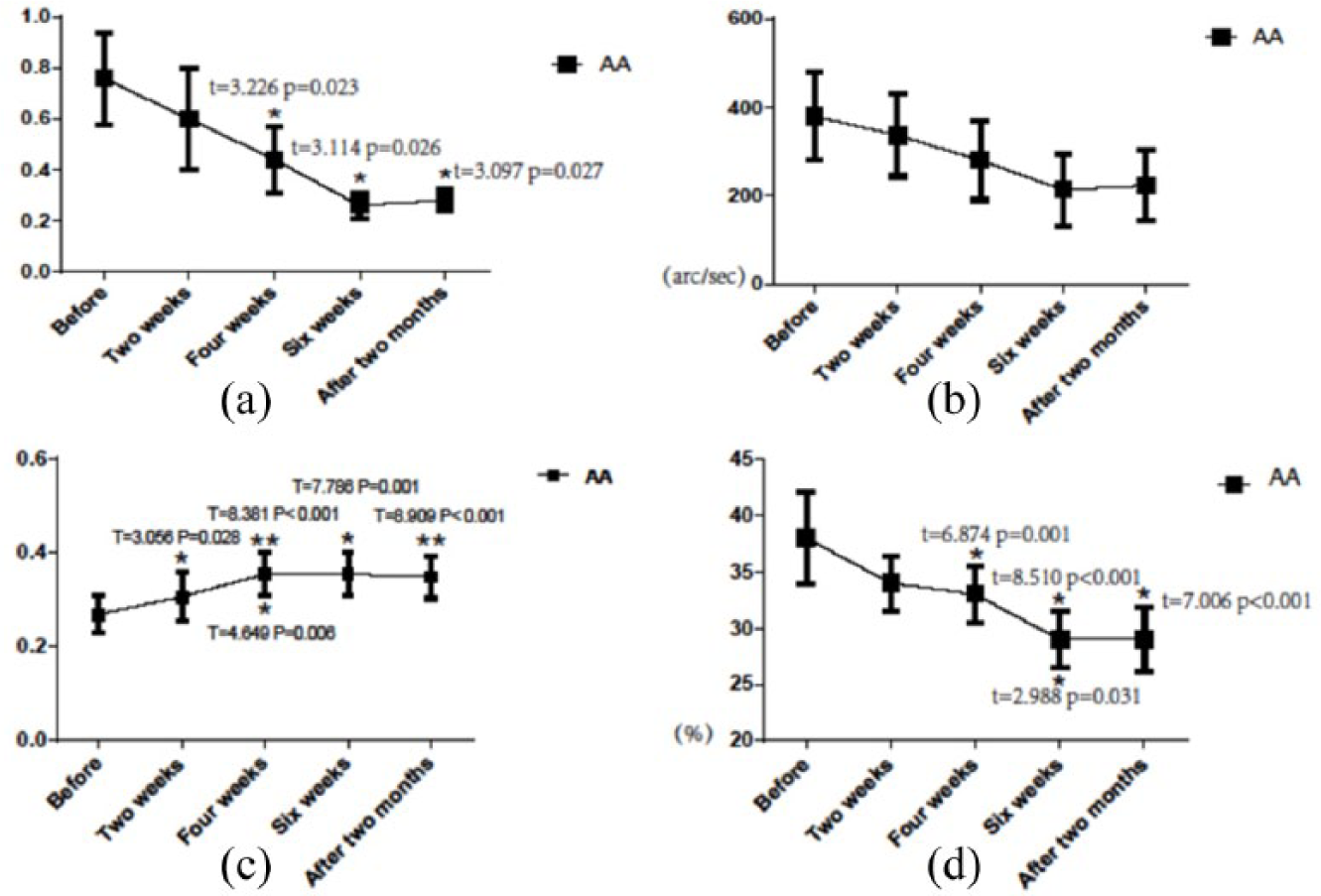
The vertical axis represents the outcome of visual acuity, stereo, contrast sensitivity, and coherence threshold before training, 6 weeks after training, and 2 months after the end of training in the AA group. The horizontal axis represents the time of training. The error bars indicate SEM. “*” above the bar indicates a significant difference (p < 0.05) between the week after training and before training. “*” under the bar indicates significant differences between the week and previous time points. Significant t- and p-values are shown in these figures. (a) Visual acuity; (b) stereo; (c) contrast sensitivity; and (d) motion coherent threshold before training, 6 weeks after training, and 2 months after the end of training. The outcomes of visual acuity and contrast sensitivity of AA patients were significantly increased in 6 weeks after training as compared to that before training. The outcome of motion coherent threshold is decreased. The outcome of visual acuity, contrast sensitivity, and coherence threshold showed significant differences between pre-training and 2 months after the end of training. No significant difference was observed in the outcomes of visual acuity, contrast sensitivity, and motion coherence threshold between 2 months after the end of training and the end of training (6 weeks).
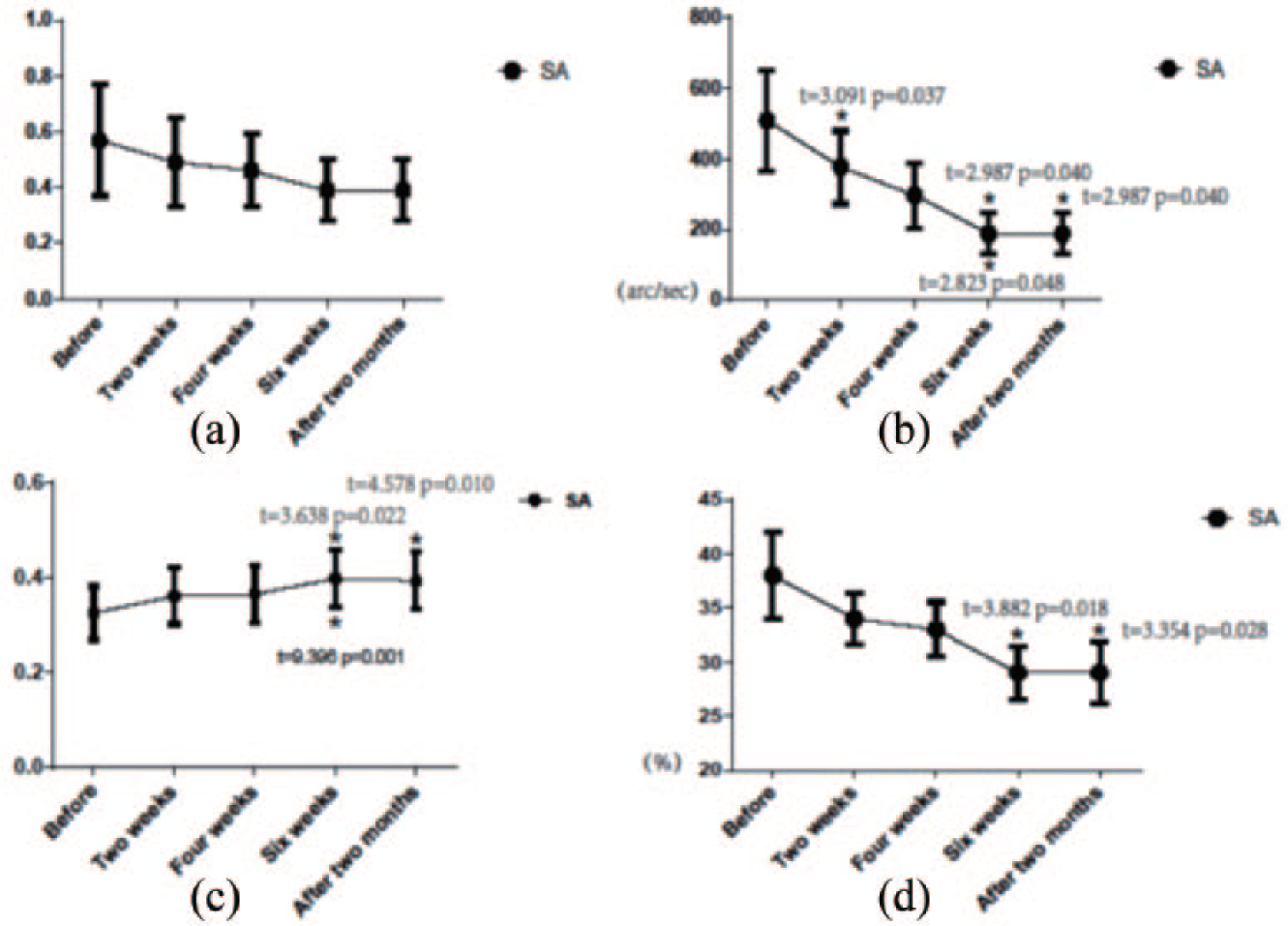
The vertical axis represents the outcome of visual acuity, stereo, contrast sensitivity, and coherence threshold before training, 6 weeks after training, and 2 months after the end of training in the SA group. The horizontal axis represents the time of training. The value of bar indicates SEM. “*” over the bar indicates a significant difference between the current week and before training. “*” under the bar indicates significant differences between the current and previous weeks. Significant t- and p-values are shown in these figures. (a) Visual acuity ; (b)stereo; (c) contrast sensitivity; and (d) motion coherent threshold before training at 6 weeks after training and 2 months after the end of training. The outcomes of stereo and contrast sensitivity of AA patients were significantly increased in 6 weeks after training as compared to that before training. Moreover, the outcome of motion coherent threshold is decreased. The outcome of stereo, contrast sensitivity, and coherence threshold showed significant differences between pre-training and 2 months after the end of training. No significant differences were noted in the outcomes of stereo, visual acuity, contrast sensitivity, and motion coherence threshold between 2 months after the end of training and the end of training (6 weeks).
A subset of the estimation of participants’ suppression is shown in Figure 3(a) and (b), and data represent before and 6 weeks after training.

(a) Estimation of suppression in AA group: interocular contrast ratio curves of the dichoptic global coherence paradigm of the AA group. Data before training and after 6 weeks training from one observer are shown in separate panels. In each panel, the vertical axis represents the motion coherence threshold, and the horizontal axis represents interocular contrast ratio (fellow eye/amblyopic eye). The coherence thresholds of AE that were measured when the amblyopic eye saw signal “Gabor” dots, which are shown as ‘’ points and the coherence thresholds of FE were measured when the fellow eye saw signal “Gabor” dots shown as ‘ ’ points. The intersection between the two solid lines in a panel was the balance point (the measurement of suppression). Solid lines represent the predictions of the Gaussian curve fitting. (b) Estimation of suppression in SA group: interocular contrast ratio curves of the dichoptic global coherence paradigm of the SA group. Data before training and after 6 weeks training from one observer are shown in separate panels. In each panel, the vertical axis represents motion coherence threshold, and the horizontal axis represents the interocular contrast ratio (fellow eye/amblyopic eye).
’ points. The intersection between the two solid lines in a panel was the balance point (the measurement of suppression). Solid lines represent the predictions of the Gaussian curve fitting. (b) Estimation of suppression in SA group: interocular contrast ratio curves of the dichoptic global coherence paradigm of the SA group. Data before training and after 6 weeks training from one observer are shown in separate panels. In each panel, the vertical axis represents motion coherence threshold, and the horizontal axis represents the interocular contrast ratio (fellow eye/amblyopic eye).
Discussion
Previously, amblyopia was alleged to be a deficit in the AE. 22 In childhood, this deficit could be improved; however, in adults, the maturity of the nervous system does not allow the deficit to return to normal. Recent studies showed that intact binocular function and the visual ability of AE were suppressed rather than faded under binocular viewing conditions.10,12 Current evidence indicates that suppression plays a primary role in both binocular and monocular deficits experienced by patients with amblyopia. These findings have led the scientists to focus on a new approach to the treatment of amblyopia that targets suppressive interactions within the visual cortex. Thus, the most valuable and reliable approaches, based on this theory, are high-frequency transcranial electrical stimulation23,24 (hf-tRNS) and perceptual learning treatment.25–27 Polat 26 and Campana et al. 28 combined hf-tRNS and perceptual learning treatment to exhibit a significant improvement in visual acuity. The studies also indicated that single perceptual learning treatment might show some improvement in amblyopic adults; however, no significant difference was noted that indicated whether hf-tRNS was better than perceptual learning treatment. Moreover, perceptual learning treatment was rather amusing than boring hf-tRNS; also, hf-tRNS can potentially induce epilepsy. Thus, this study focused on perceptual learning treatment.
In this study, we chose a static Gabor task for training our patients, based on the approach first reported by Mansouri et al. 29 The study aspired to find a reliable method to measure the suppression of binocular interactions; however, some of the participants exhibited an improved visual function after the completion of the study. Nevertheless, all the participants in the study were repeatedly treated by more than one perceptual mission, and the one that effectuated finally cannot be deduced. Zhou et al. 30 proposed a new model find a reliable method to measure the suppression of binocular in DGOC and “Sinusoidal Waveform Coherence (SWC)” in measuring the suppression in binocular interactions. Recently, some studies indicated that amblyopia might injure the PP, which is in charge of color and shape more than the MP that is responsible for motion.31,32 As the DGOC seemed to be inclined to the PP and DGMC toward the MP, we selected DGOC as our training paradigm and DGMC as the measurement of suppression. In addition, we also reduced the duration of DGMC measurement to exclude its influence on the perceptual learning treatment.
In this study, after 6nweeks of DGOC training, visual acuity and contrast sensitivity improved and coherence threshold declined in the AA group. On the other hand, stereo and contrast sensitivity improved and coherence threshold declined in the SA group; the changes in both groups were retained for at least 2 months after the end of the training (Figures 1 and 2). Thus, first, DGOC can be applied in the treatment of adult AA or SA. Second, the stereo did not improve significantly in AA, and the visual acuity did not improve significantly in SA. After 6fweeks of DGOC training in the same frequency, the AA group got an improvement in visual acuity, but the SA group got an improvement in stereo. There are evidences to show that AA and SA were injured in different pathways, and in our study DGOC training is apt to PP, so we think the diverse results might come from the different pathway injury in AA and SA.
In the SA group, stereo was significantly improved, while in the AA group, the stereo did not improve significantly (p > 0.05). A dioptric difference between the eyes is one of the most common causes of unilateral amblyopia. If a retinal image is blurry in one eye, then the visual acuity of this eye cannot develop properly; thus, the visual stimulus is insufficient for the appropriate development of visual acuity, resulting in unclear retinal image of the fixed object in the eye with severe refractive error, which might be the mechanism in AA. 33 In SA, both eyes can get a clear vision; however, these two visions differ in that the main center cannot fuse. During the process of maturity of visual center, the power to suppress the other eye is gained, followed by the occurrence of amblyopia.34,35 The MP is in charge of motion and depth vision, and hence, the visual pathway in SA which might be injured should be the MP. Zele et al. 31 reported that both AA and SA showed contrast sensitivity deficits on the MP and PP; the SA deficit is inclined to the MP, while the AA deficit is inclined to the PP. Furthermore, we measured the suppression between AE and FE and observed that in both AA and SA groups, suppression is declined significantly after perceptual learning treatment accompanied by the improvement of visual acuity, stereo, or contrast sensitivity. Thus, Zhou et al. 30 reported that suppression plays a critical role in amblyopia, irrespective of AA or SA. DGOC was selected as an approach of perceptual learning treatment, which can potentially stimulate the PP, while in the SA group, the stereo of the MP was improved. Thus, we hypothesized that as compared to AA, the stereo vision in SA was suppressed as long as plasticity existed; when the suppression was removed it improved significantly, and similar to a spring, the more it was compressed, the more it jumped. In a similar theory, compared to SA, the visual acuity in AA was suppressed more as long as plasticity existed and diopter was corrected, and when the suppression was removed, it also improved remarkably.
Another concern is the marked improvement of contrast sensitivity in both AA and SA groups. In previous studies, by the use of abnormal contrast sensitivity as golden standard in diagnosing amblyopia36,37, several reports indicated that patients with amblyopia might have been injured in both PP and MP.38,39 With declining suppression, the visual cortex can obtain further information from the AE, and AE obtain neural rewards and training, such that the contrast sensitivity improves step by step. Some of our participants might acquire diplopia in a short process of learning treatment, but as the training continues, they can overcome the diplopia. This phenomenon might indicate both a quick recovery of visual acuity and contrast sensitivity, and a relatively slow recovery of fusion function. 40 As the training continues, the fusion function improves and the diplopia disappears.
Nevertheless, several differences were observed between adult amblyopia and child amblyopia. First, the adults are matured individuals, and hence, the therapy of low visual function is rather difficult as compared to that in children. Second, owing to the need of driving, playing, working, and self-respect, the adults emphasize the treatment. Third, most of the adults cannot accept the treatment with monocular goggle occlusion, which demonstrated only little function in adult amblyopia, and thus, a novel method is required to cure adult amblyopia. Although the cellular or molecular changes before and after training in the brain were not enlightened, the observations indicated that DGOC perceptual learning treatment could be suitable in adult amblyopia, and Li et al. 41 verified this technology can be used in an iPod. These results not only supported such perceptual learning treatment in the treatment of the adult but also showed that AA and SA might be injured in different visual pathways. The result after treatment is different, and the suppression might play a major role in the mechanism underlying AA and SA.
Footnotes
Authors’ note
Liu Shuai is also affiliated with Department of Ophthalmology, Hefei First People’s Hospital, Anhui, China.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.