
Abstract
Purpose:
To determine the value of the polymerase chain reaction analysis of aqueous humor specimens as a tool to diagnose cytomegalovirus retinitis in AIDS patients.
Methods:
In all, 63 AIDS patients were evaluated in this study. They were sorted into two diagnostic categories: eyes with active cytomegalovirus retinitis and eyes without active cytomegalovirus retinitis. The aqueous humor and blood samples were collected and analyzed by polymerase chain reaction.
Results:
A total of 49 patients had active cytomegalovirus retinitis (77.8%) and 14 patients had inactive cytomegalovirus retinitis or normal fundus (22.2%). The mean average of patients was 39 years (range: 22–59). The majority of patients were male (90.5%). Cytomegalovirus DNA was detected in 46 and 7 of 49 aqueous and blood samples, respectively, from AIDS patients with active cytomegalovirus retinitis. We did not detect cytomegalovirus DNA in any of the eyes without active cytomegalovirus retinitis. The sensitivity of polymerase chain reaction in the detection of cytomegalovirus in aqueous humor and blood samples was 93.5% and 14.3%, respectively.
Conclusions:
The polymerase chain reaction analysis is a safe, highly specific, and sensitive method to diagnose cytomegalovirus retinitis.
Introduction
Cytomegalovirus retinitis (CMVR) is the most common sight-threatening complication of acquired immunodeficiency syndrome (AIDS), occurring in up to 25%–40% of patients.1–3 In most cases, the diagnosis of CMVR is based on the appearance of the fundus by ophthalmoscopy which are typical but not always specific. 4 However, atypical manifestations occur in some patients. It may be difficult to distinguish from retinopathies caused by varicella-zoster virus or herpes simplex virus and other rare pathogens, such as Treponema pallidum and Toxoplasma gondii, which may have similar clinical signs. Therefore, it is imperative that patients should be accurately diagnosed as early as possible. A polymerase chain reaction (PCR) diagnosis has proven to be very useful because only a very small sample is required. The purpose of this study was to determine the value of the PCR analysis of aqueous humor specimens as a tool to diagnose CMVR.
Methods
Patients
The study population consisted of 63 AIDS patients at the Beijing DiTan Hospital, Capital Medical University between March 2014 and September 2017. They were sorted into two diagnostic categories based on ophthalmoscopic fundus examination. (1) Eyes with active CMVR: The typical lesion consisted of an area of retinal necrosis or edema surrounded by granular infiltrates and a silvery white border marking the edge of the active borders, with variable amounts of retinal hemorrhage and inflammatory vascular sheathing. Those cases with atypical manifestation were excluded. (2) Eyes without active CMVR (eyes with inactive CMVR or without lesion): The retina remains thin and atrophic associated with clumping of the retinal pigment epithelium and attenuated vessels. 5 (Figure 1) Samples of aqueous humor and plasma were obtained from these patients. T-cell subsets were obtained. Each patient had an ophthalmic evaluation that included slit-lamp examination and dilated fundus examination performed by the staff ophthalmologist. The diagnosis of CMVR was based on the typical fundus appearance of the disease and made by two ophthalmologists. All of these patients with CMVR were newly diagnosed. None of them had been treated previously with intravenous or intravitreal foscarnet or ganciclovir.
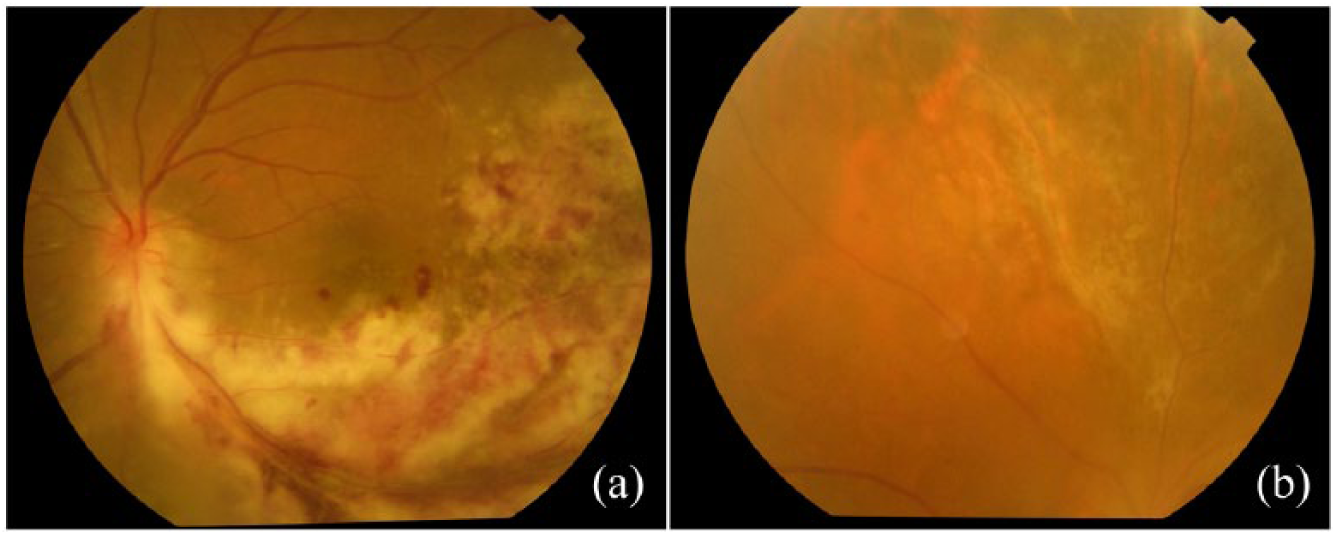
Fundus photographs of (a) active CMVR and (b) inactive CMVR.
Specimen collection and processing
Blood samples were collected in ethylenediaminetetraacetic acid (EDTA) tubes and stored at −20°C until the PCR was run. The aqueous humor specimen was taken from the worse eye of each patient. If both eyes were normal, one eye would be selected at random to undergo anterior chamber tap.
Standard preparation for obtaining an aqueous humor specimen included topical anesthesia and the use of a sterile lid speculum. An anterior chamber paracentesis was performed using a 30-gauge needle. A 0.1-mL aqueous humor was aspirated and acquired for real-time PCR (diagnostic kit for the quantification of human CMV DNA, PCR-Fluorescence; Da An Gene Co., Ltd, Sun Yat-Sen University, China).
Statistical analysis
SPSS software for Windows version 22.0 was used. Descriptive statistics were computed. All data were expressed as the mean ± standard deviation (SD). Comparisons of PCR results between different groups were made by Fisher’s exact test. Statistical significance was considered achieved if the probability was less than 5% (p < 0.05).
Results
In all, 63 patients were evaluated in this study: 49 patients had active CMVR (77.8%) and 14 patients had inactive CMVR or normal fundus (22.2%). Six patients of each group have systemic CMV infection. Systemic CMV infection did not correlate with CD4 counts (p = 0.137). The mean average of patients was 39 years (range: 22–59). The majority of patients were male (90.5%). The mean and median CD4+ T-lymphocyte cell counts were 90 cells/µL (SD: 129.4) and 34 cells/µL, respectively. In all cases, aqueous humor specimens were screened for CMV by the real-time PCR.
Table 1 lists the comparison of patients with active CMVR and without active CMVR in gender, age, and CD4+ T-lymphocyte cell count.
Comparison of patients with active CMVR and without active CMVR (n = 63).
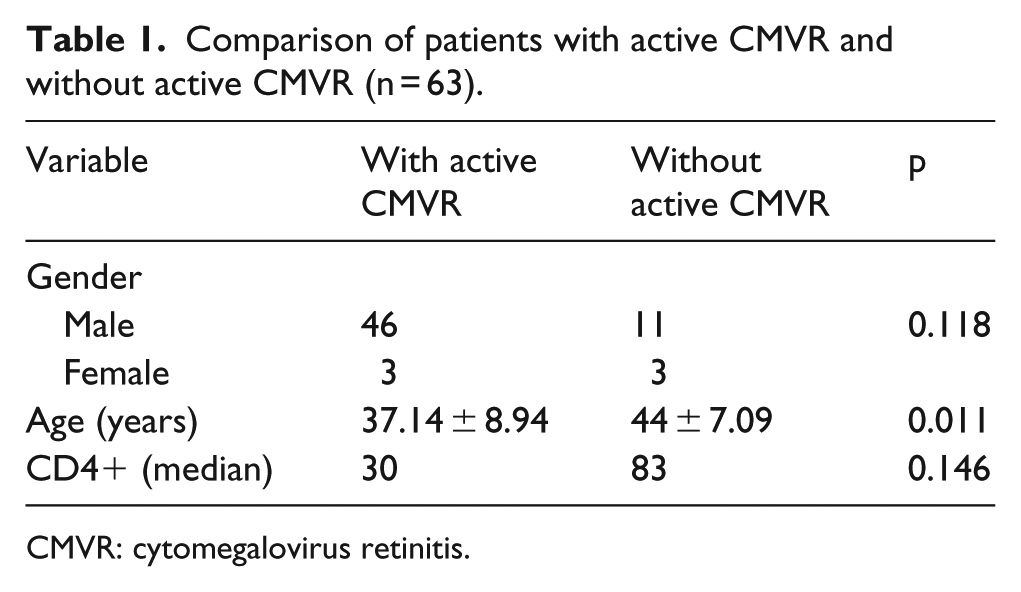
CMVR: cytomegalovirus retinitis.
To determine the sensitivity of PCR assay for CMV DNA in aqueous humor of the patients, we studied aqueous specimens from 49 patients with active CMVR. Of 49 aqueous specimens from 49 eyes with active retinitis, 46 (93.5%) were CMV PCR positive. To determine the specificity of PCR assay for CMV DNA in aqueous humor of the patients, we studied aqueous specimens from 14 patients without active CMVR. We did not detect CMV DNA in any of the eyes without active CMVR. Therefore, the sensitivity was calculated to be 93.5% and the specificity was calculated to be 100%.
We analyzed blood specimens collected from the patients at the same time as the aqueous specimens in order to compare the sensitivity and specificity of aqueous specimens with blood specimens for diagnosing active CMVR. Of 49 plasma specimens from 49 patients with active retinitis, 7 (14.3%) were CMV PCR positive. The sensitivity of plasma specimen was calculated to be 14.3%. There was no correlation between Plasma CMV PCR results and CMVR activity (p = 0.333 > 0.05; Table 2).
PCR assay of CMV DNA from aqueous humor and plasma correlates with CMVR activity.
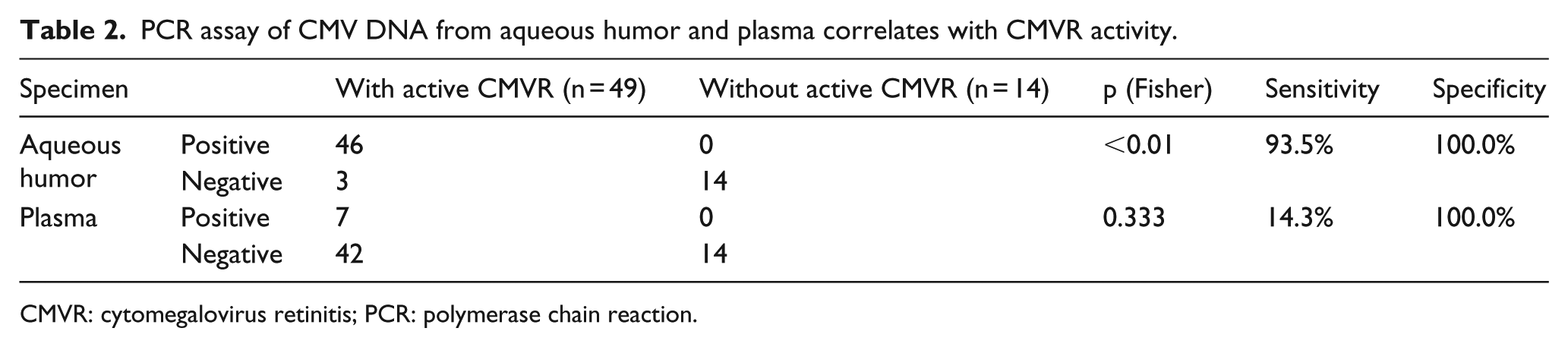
CMVR: cytomegalovirus retinitis; PCR: polymerase chain reaction.
Aqueous humor samples from three patients were negative, which was not inconsistent with the clinical status of CMVR. All of them had no symptoms and were found to have positive lesions by routine examination. All of their fundus examination showed that the surface area of CMVR was tiny (less than 2 disk diameter (DD); Figure 2). Case 1 refused treatment at first. He came to ophthalmic clinic with the complaint of blurred vision 2 months later. Anterior chamber paracentesis was performed again. High copies of CMV DNA in the aqueous humor sample (4.08 × 104 copies/mL) were detected. Case 2 and Case 3 were diagnosed with CMVR and received intravenous foscarnet. The retinitis regressed after 2–3 weeks of treatment.
Of the 63 eyes, 2 eyes in this study experienced complications of subconjunctival hemorrhage. No one had retinal detachments or endophthalmitis.
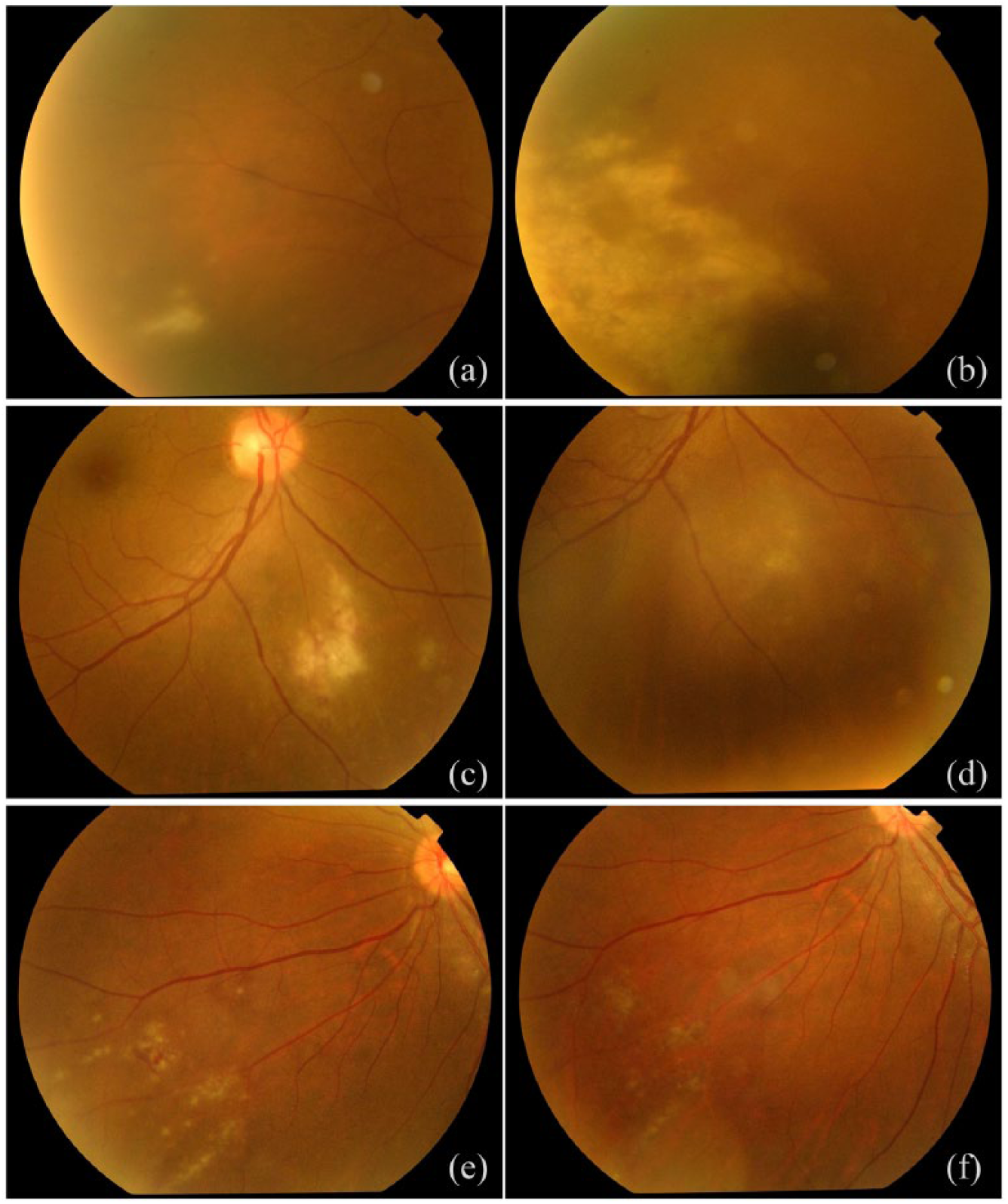
Fundus photographs of (a and b) Case 1, Case 2 (c) before and (d) after (2 weeks) treatment with foscarnet, and Case 3 (e) before and (f) after (3 weeks) treatment with foscarnet.
Discussion
The PCR is a highly sensitive, specific, and rapid technique for the detection of small quantities of viral DNA in intraocular fluids. 6 PCR testing is recognized as an important assay in the diagnosis of CMV-related disease. The use of the PCR in the detection of virus has many advantages. Most important is the great sensitivity that a PCR assay can provide. 7 Another important factor is that PCR needs small-volume sample, which is essential for eyes.
Pathanapitoon and associates used PCR-based assay to detect CMV DNA in conjunctival samples from patients with untreated CMVR and detected that the use of PCR in the detection of cytomegalovirus in conjunctival samples had sensitivity of only 12%. 8 This sensitivity of PCR assay is too low to have clinical utility for the diagnosis of CMVR. The sensitivity of PCR in detection of CMVR in vitreous and aqueous were 67% and 37%, respectively, in that study, which is lower than the 93% sensitivity of aqueous PCR in this study. The possible reasons that made the difference were due to different PCR-based assay and different specimen handing. Meanwhile, it was reported that PCR amplification of CMV DNA from both vitreous and aqueous specimens can provide highly sensitive and specific markers to diagnose CMVR.9,10 Compared with pars plana vitreous biopsy for vitreous specimen, anterior chamber paracentesis for aqueous specimen is associated with fewer complications. It is easier to get samples of aqueous humor, and serious side effects are rare. For this reason, we chose aqueous specimen as detecting objects. Of the 63 eyes, 2 in this study experienced complications of subconjunctival hemorrhage. No one had retinal detachments or endophthalmitis.
CMV is responsible for asymptomatic, life-long infections in 50%–90% of the healthy population. 11 It is proved that leukocytes are the major source that spread CMV in the blood, 12 and vascular endothelial cells and retinal pigment epithelial (RPE) cells are major objectives of CMV in the eye. 13 However, the pathway that CMVR caused by CMV after initial infection was controversial. It was speculated that CMV establishes its latent infection and reactivation in situ in the retina, which was supported by the detection of CMV antigen in the retina of AIDS patients without CMVR. 14 Our study indicates that PCR assay of CMV DNA from plasma has low positive predictive values for the diagnosis of CMVR. Out of 49 blood samples of active CMVR, 42 were CMV DNA negative which indicated that CMV DNA in the ocular fluid may originate from retina.
This study reported that sensitivity and specificity of the PCR assay of CMV DNA from aqueous specimen for the diagnosis of CMVR were 93.5% and 100%, respectively. The positive result is suggestive that CMV is the cause of end-organ disease. Out of 49 aqueous humor samples of active CMVR, 3 were CMV DNA negative. All of their fundus examination showed that the surface area of CMVR was tiny (less than 2DD). It has been proved that the concentration of CMV DNA in aqueous was directly related to the area of active CMVR. 9 Therefore, we speculated that CMVR with small area may not release sufficient CMV DNA into ocular fluids for detection by PCR.
In conclusion, strengths of this study include its large sample size (including 49 cases of active CMVR). There is a direct correlation between the clinical diagnosis of CMVR and the PCR analysis of aqueous humor specimens. CMV PCR can be useful in assessing aqueous humor specimens to diagnose CMVR and differentiate from other intraocular infections caused by herpes simplex virus, herpes zoster virus, syphilis, and toxoplasmosis, which mimic the manifestation. The PCR assay is a relatively safe, highly specific, and sensitive method for the diagnosis of CMVR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by “Beijing Talents Fund” (grant number: 2015000021469G202) and “Beijing Municipal Administration of Hospitals Incubating Program” (grant number: PX2018061).