
Abstract
Purpose:
To analyze the correlation between age, gender, refractive error, keratometry, and corneal thickness in a large group of subjects.
Methods:
This study is a retrospective analysis of patients who underwent refractive surgery between January 2000 and February 2015 at Care Vision Refractive Clinic, Tel Aviv, Israel. Patient demographics, subjective refraction, pachymetry, and average keratometry were collected.
Results:
Overall, 51,113 eyes of patients averaging 28.8 ± 9.3 years of which 53.9% were males were included. Average keratometry, spherical equivalent and cylindrical error differed significantly between male and female subjects (p < 0.001), while pachymetry did not (p = 0.332). In myopic eyes, correlations between age, pachymetry, average keratometry, spherical equivalent, and cylindrical error were all statistically significant except for the correlation between age and either pachymetry (p = 0.462) or spherical equivalent (p = 0.016). All correlations found were negligible or small (|r|= 0.003 to 0.141). In hyperopic eyes, correlations between age, pachymetry, average keratometry, spherical equivalent, and cylindrical error were all statistically significant except for the correlation between average keratometry and either pachymetry or cylindrical error (p = 0.344 or p = 0.274, respectively). All correlations found were negligible or small, except for a moderate correlation found between age and cylindrical error (r = 0.365).
Conclusion:
Refractive state, pachymetry, and keratometry of refractive surgery candidates are mostly weakly correlated.
Introduction
The refractive status, corneal thickness, and keratometry are important parameters used in the evaluation and management of corneal pathologies. Specifically, they are indispensable when planning refractive surgery. These parameters affect the type of refractive procedure chosen and are the basis for laser ablation programming. The refractive status, corneal thickness, and keratometry are also important in risk assessment prior to surgery. Each of them is an independent factor associated with postoperative complications such as corneal ectasia.1,2 They are also important in risk assessment of intraoperative complications, such as those related to flap creation and adherence. In addition, they influence visual outcome following surgery. 3
Therefore, it is important to better understand these components and evaluate possible relationship between them. Several studies previously evaluated this relationship, but had conflicting results.4–11 In this study, we analyzed refractive error, keratometry, corneal thickness, and their correlation with each other and with patient age and sex, in a large group of subjects.
Materials and methods
This study is a retrospective analysis of the electronic medical records of all patients who underwent refractive surgery between January 2000 and February 2015 at Care Vision Refractive Clinic, Tel Aviv, Israel. Exclusion criteria were age <18 years, previous laser refractive surgery, history of corneal pathology, emmetropia, or incomplete data that preclude analysis. Included in the study were 51,113 eyes of 26,869 patients. The study was approved by the Institutional Review Board of the Tel Aviv Medical Center, Tel Aviv, Israel.
The following data were recorded and assessed: patient demographics, subjective refraction (including spherical and cylindrical corrections), pachymetry, and average keratometry (AK). Subjective refraction was performed by an optometrist. Spherical equivalent (SE) was calculated as the sum of the sphere and half the cylinder in diopters (D). Pachymetry (minimal corneal thickness) was obtained using contact ultrasound between 2000 and 2005, using Orbscan (Bausch & Lomb, Rochester, NY, USA) between 2006 and 2010, or using Sirius (C.S.O., Florence, Italy) between 2011 and 2015. Keratometry was obtained using TMS-4 (Tomey, Erlangen, Germany) between 2000 and 2005, Orbscan between 2006 and 2010, or using Sirius between 2011 and 2015.
Statistical analysis
Data were recorded in Microsoft Excel and analyzed using SPSS version 21 (SPSS Inc., Chicago, IL, USA). Analysis was initially of the entire cohort, followed by analysis of the myopic (SE < 0) and hyperopic (SE > 0) groups separately, with a comparison between them. Comparison was also made between male and female groups. One-way analysis of variance was used to compare multiple group averages with adjustment for multiple comparisons using Bonferroni correction. The Pearson correlation was used to analyze the relationship between continuous variables. Chi-square was used for comparison of categorical variables such as types of astigmatism. A p value less than 0.001 was considered statistically significant.
Interpretation of correlation coefficient
The conventional guidelines for correlation coefficients interpretation as described by Cohen were used. 12 Briefly, correlation coefficients (absolute) of <0.10, 0.10–0.29, 0.30–0.49, and ⩾0.50 were considered negligible, small, medium, and large, respectively. 12
Results
Of the 51,113 eyes included, 50.1% were right eyes and 53.9% were males. Average age was 28.8 ± 9.3 years. Pachymetry was 533 ± 34 µm, AK was 44.0 ± 1.5 D, cylindrical error was 0.83 ± 0.86 D, and SE was –3.69 ± 2.51 D. Astigmatism types were distributed as follows: with-the-rule astigmatism in 46.5%, against-the-rule astigmatism in 21.1%, oblique astigmatism in 9.2%, and no astigmatism in 23.3%. The distribution of age, pachymetry, AK, and SE is shown in Figure 1.
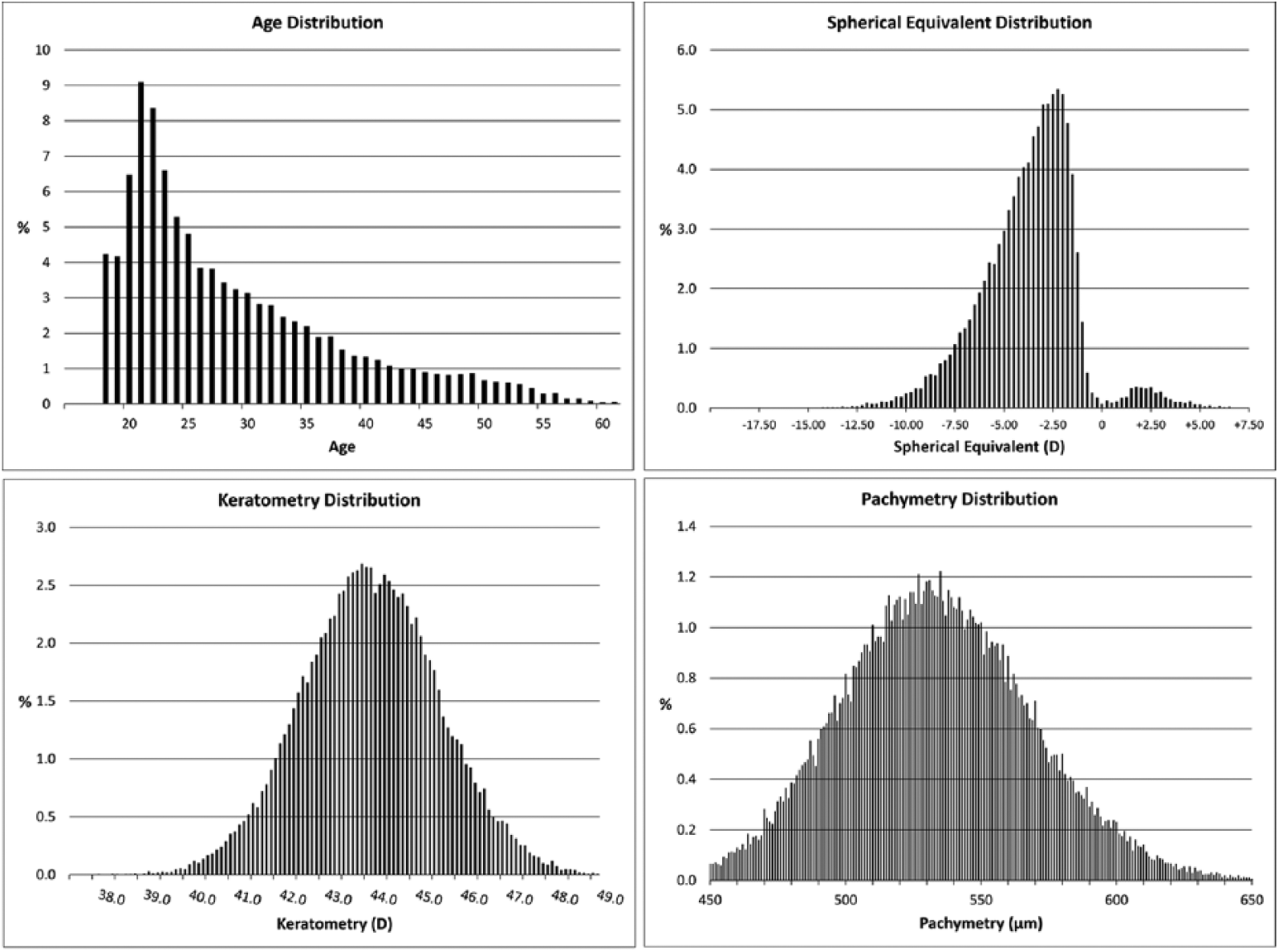
Distribution of age, spherical equivalent, keratometry and pachymetry.
AK, SE, and cylindrical error differed significantly between male and female subjects (p < 0.001 for all), while pachymetry did not (p = 0.332). Females had a slightly higher rate of with-the-rule astigmatism compared with males (49.3% vs 44.1%, p < 0.001), while males had a slightly higher rate of against-the-rule astigmatism compared with females (24.5% vs 17.0%, p < 0.001). Female AK was 0.60 ± 0.03 D steeper, and female SE was 0.31 ± 0.04 D more myopic than male AK and SE. Gender comparison is shown in Table 1.
Comparison between males and females.
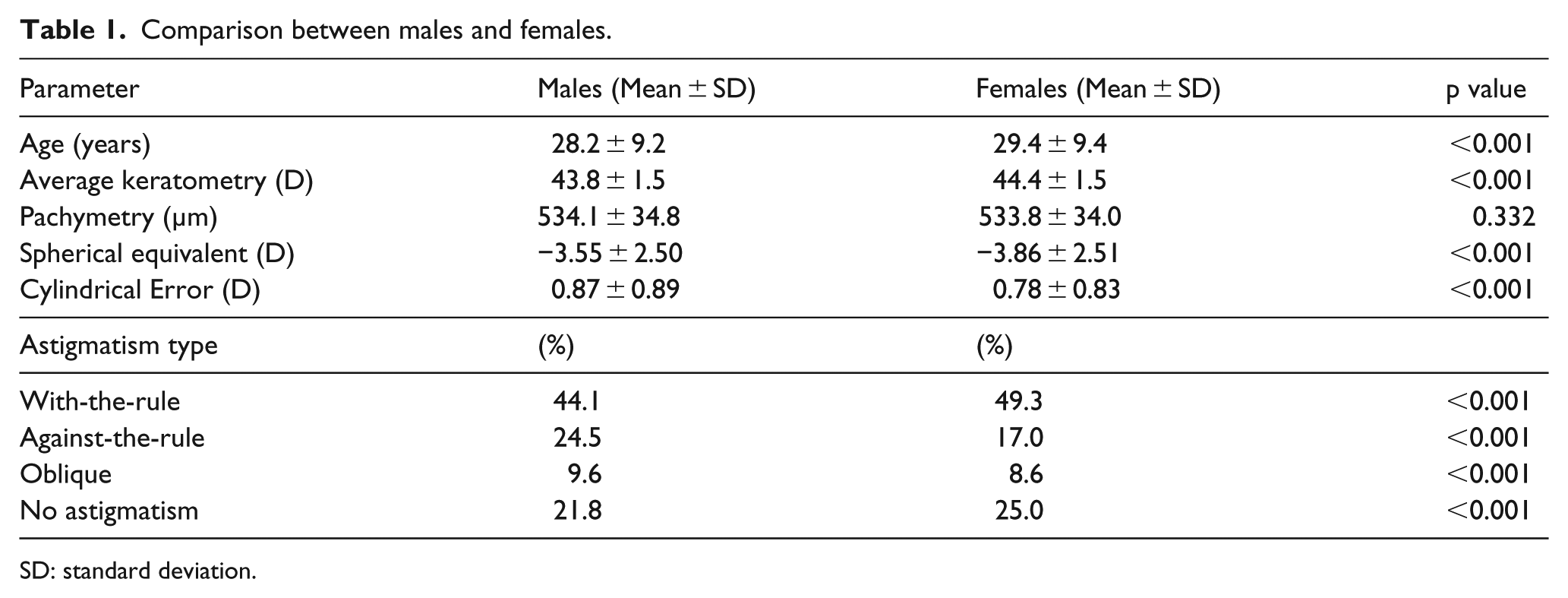
SD: standard deviation.
Correlation analysis
Correlations between age, pachymetry, AK, SE, and cylindrical error were all statistically significant except for the correlation between pachymetry and SE (p = 0.944). All correlations found were negligible to small, with absolute values ranging from r = 0.0003 to r = 0.206 (Table 2). The strongest correlation found was between age and SE (r = 0.206, p < 0.001).
Correlation analysis—entire cohort.
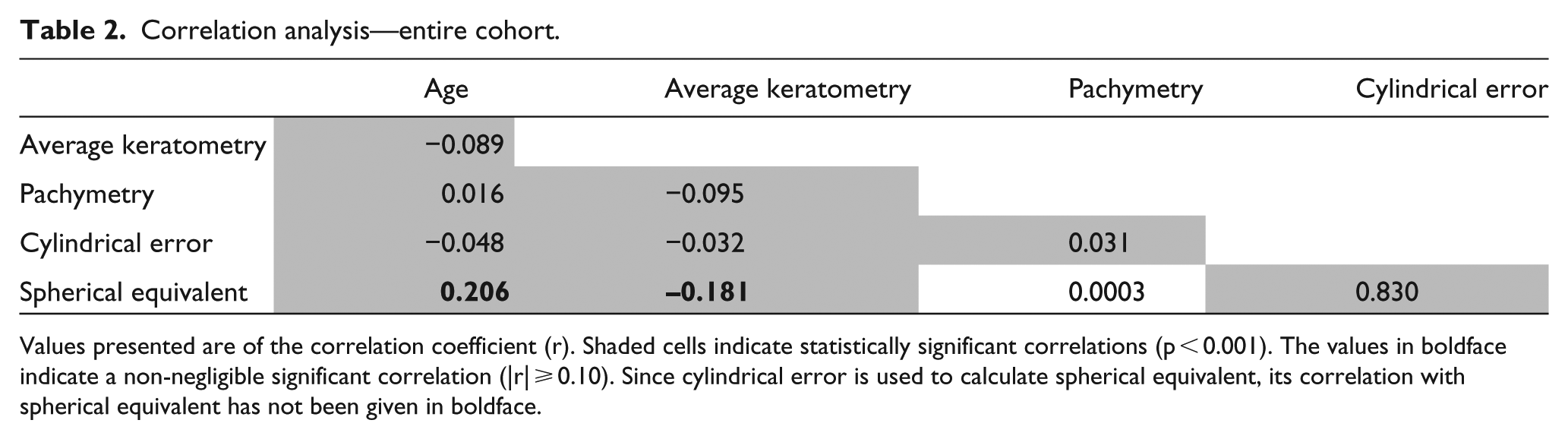
Values presented are of the correlation coefficient (r). Shaded cells indicate statistically significant correlations (p < 0.001). The values in boldface indicate a non-negligible significant correlation (|r| ⩾ 0.10). Since cylindrical error is used to calculate spherical equivalent, its correlation with spherical equivalent has not been given in boldface.
Analysis of myopic and hyperopic eyes
There were 48,889 myopic eyes and 2224 hyperopic eyes. Pachymetry, AK, SE, and cylindrical error differed significantly between myopic and hyperopic subjects (p < 0.001 for all). Myopic AK was 0.90 ± 0.06 D steeper, and myopic pachymetry was 6.8 ± 1.5 µm thinner than hyperopic AK and pachymetry. Myopic eyes had a significantly higher rate of with-the rule astigmatism compared with hyperopic eyes (47.4% vs 26.0%, p < 0.001) while hyperopic eyes had a significantly higher rate of against-the rule astigmatism compared with myopic eyes (37.8% vs 20.3%, p < 0.001). Comparison between myopic and hyperopic eyes is shown in Table 3.
Comparison between hyperopic and myopic eyes.
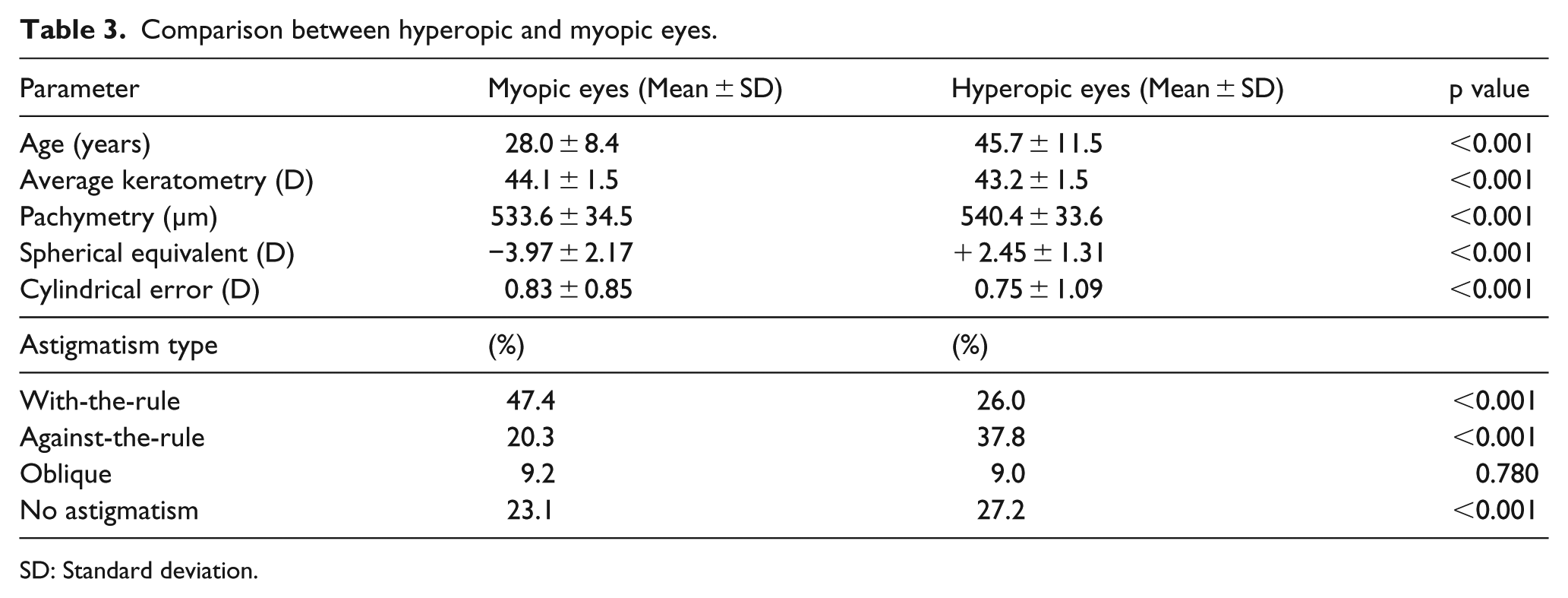
SD: Standard deviation.
In myopic eyes, correlations between age, pachymetry, AK, SE, and cylindrical error were all statistically significant except for the correlation between age and either pachymetry (p = 0.462) or SE (p = 0.016). All correlations found were negligible to small, with absolute values ranging from r = 0.003 to r = 0.141 (Table 4). In hyperopic eyes, correlations between age, pachymetry, AK, SE, and cylindrical error were all statistically significant except for the correlation between AK and either pachymetry or cylindrical error (p = 0.344 or p = 0.274, respectively). All correlations found were negligible to small (Table 5), except for a moderate correlation found between age and cylindrical error (r = 0.365).
Correlation analysis—myopic eyes.
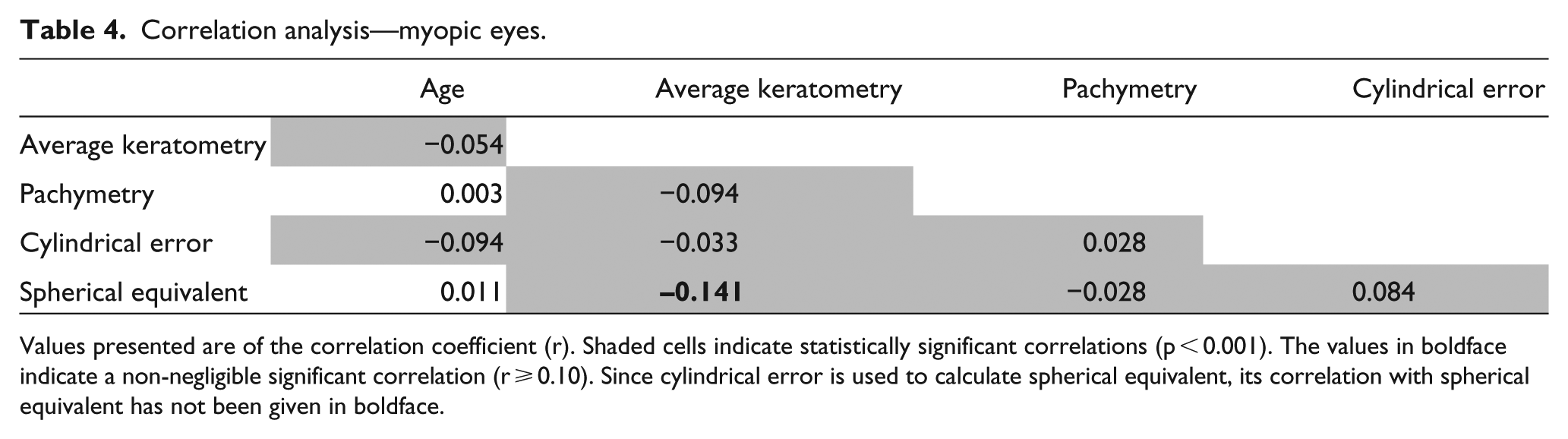
Values presented are of the correlation coefficient (r). Shaded cells indicate statistically significant correlations (p < 0.001). The values in boldface indicate a non-negligible significant correlation (r ⩾ 0.10). Since cylindrical error is used to calculate spherical equivalent, its correlation with spherical equivalent has not been given in boldface.
Correlation analysis—hyperopic eyes.
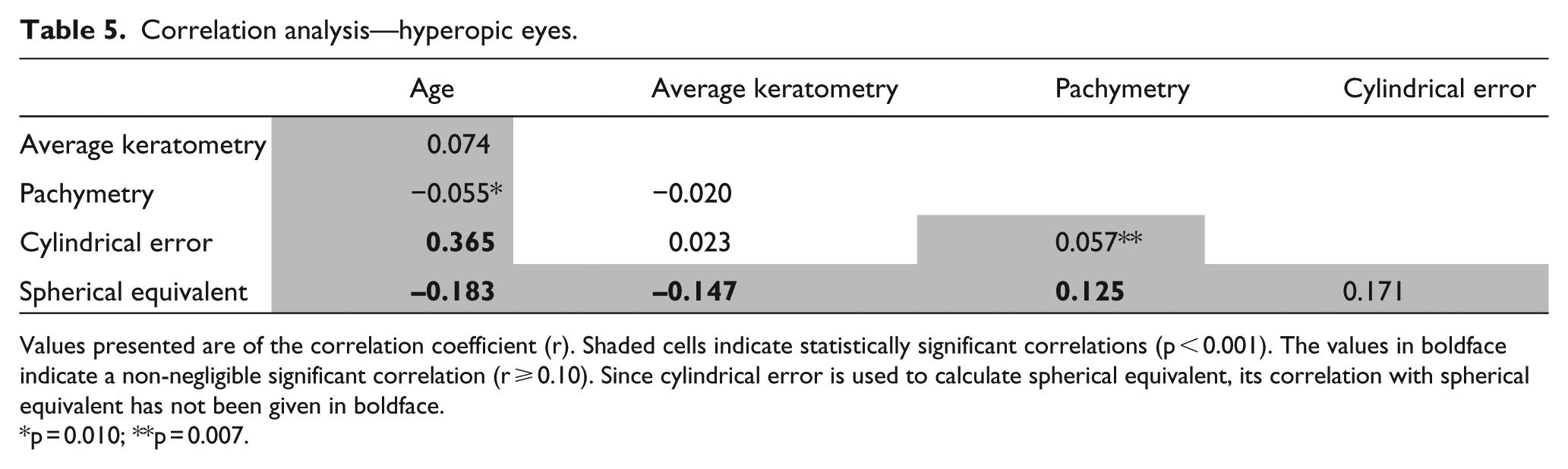
Values presented are of the correlation coefficient (r). Shaded cells indicate statistically significant correlations (p < 0.001). The values in boldface indicate a non-negligible significant correlation (r ⩾ 0.10). Since cylindrical error is used to calculate spherical equivalent, its correlation with spherical equivalent has not been given in boldface.
p = 0.010; **p = 0.007.
Discussion
In this large data analysis, the possible relationship between the refractive state, pachymetry and keratometry has been examined in a very large cohort. When examining the correlation between these parameters in the entire cohort, myopic eyes and hyperopic eyes, the examined parameters either had a small, negligible, or no correlation with each other with the only exception being a medium correlation between age and cylindrical error in the hyperopic group only.
Keratometry differed slightly between genders, with female subjects having slightly steeper corneas (AK) than males (44.4 ± 1.5 and 43.8 ± 1.5 D, respectively, p < 0.001). Similar differences were found by AlMahmoud et al. 4 (44.2 ± 1.4 and 43.5 ± 1.5 D, respectively) in a study on 3395 eyes of refractive surgery candidates. Other smaller studies showed similar results in Asian 13 and African eyes as well. 14 These differences in ocular parameters between genders may be partially explained by potential differences in height and weight which were unfortunately not available for this study. Indeed, Wong et al. 15 described the relationship between ocular dimensions and refraction with adult stature and showed that taller persons had a tendency toward flatter corneas. Against-the-rule astigmatism was more common in males than in females, and the opposite was true for with-the-rule astigmatism. These findings correlate with those of Hayashi et al. 16 in a prospective study on 1000 eyes. The cause for this difference remains unclear.
In the current study, myopes demonstrated steeper corneas when compared with hyperopes. In addition, there was a small inverse correlation between SE and mean keratometry in both groups. In the myopic group, an increase in magnitude of refractive error was associated with greater keratometry values (r = –0.141, p < 0.001) while in the hyperopic group an increase in magnitude of refractive error was associated with lower keratometry values (r = –0.147, p < 0.001). These findings are in agreement with those of AlMahmoud et al. 4 They reported that across the entire range of refractive error, keratometry increased by 0.11 D for every diopter of decrease in refractive error.
The exact relationship between the studied parameters (corneal indices and refractive error) and age is unclear. In the current study, in the myopic group, such associations were either non-significant or demonstrated negligible correlations (|r|< 0.10). In the hyperopic group only, there was a medium correlation between age and cylinder (r = 0.365) and a small correlation with SE (r = –0.183). It is unclear whether these changes represent the entire population or simply reflect the natural process of presbyopia whereby older patients with less accommodative reserve are more likely to seek keratorefractive treatment for lower refractive errors. Hyperopic patients were also found to have a significantly higher rate of against-the-rule astigmatism compared with myopic patients (37.8% vs 20.3%, p < 0.001). This may be partly explained by the fact that the hyperopic group was significantly older than the myopic group and, therefore, may have underwent natural change of the astigmatism vector toward against-the-rule as corneas and associated refraction tend to shift from with-the-rule to against-the rule while aging. 17 In the current study, an association between age and corneal thickness was non-existent for myopes and negligible for hyperopes. Conflicting reports have been published regarding the association between age and corneal thickness with thinning of the cornea at a rate of up to 7 μm per decade being been reported by some groups,18–21 and others reporting no such association.22,23 In any event, it is unclear what clinical significance a 3–5 μm decrease in corneal thickness (~20 μm over five decades) truly has, if indeed this is a real trend. It should be noted that since our cohort is made of refractive surgery patients, it is largely younger than the general population, with a relatively small numbers of patients older than 50. This could affect correlation analysis related to age.
There was a negligible correlation between SE and corneal thickness in myopes and a small correlation in hyperopes. There have been conflicting reports regarding a possible association between refractive error and corneal thickness. Srivannaboon 24 reported a positive correlation between myopia and central corneal thickness (CCT) and high myopes (>6 D) have been reported to have a greater CCT than moderate and mild myopes. 25 Others, however, found a negative correlation 26 or no correlation.27–29 It seems as though the studies with very large cohorts (as opposed to those with smaller cohorts) identified small magnitudes of correlation between refractive error and corneal thickness which, again, are of unclear clinical significance.
This study has several limitations, first of which is its retrospective nature. Second, as the participants are candidates for refractive surgery, the findings may not apply to the general population. Third, the findings of this study apply to the population of Israel and may not apply to others, however, it is worth mentioning that due to substantial worldwide immigration to Israel since the country was first founded, the population is ethnically diverse. In addition, since the studied time period spanned over 15 years, different devices were used at different time periods to measure keratometry and pachymetry and this may have introduced additional variability into the data. Finally, additional parameters that were not studied may have contributed to the correlations of these parameters.
Nevertheless, this large data analysis described the correlations between the refractive state, pachymetry, and keratometry of refractive surgery candidates and found them to be weakly correlated for the most part.
Footnotes
Authors’ note
Nir Sorking is now affiliated with Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, Canada.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.