
Abstract
Introduction:
Optic nerve sheath meningiomas and intracavernous arachnoid cysts are both fairly rare conditions, and to the best of our knowledge, have not been previously reported to co-occur in the same patient. Both can cause diplopia, but only ONSMs have been documented to demonstrate progressive worsening of ocular motility.
Case Report:
A 67-year-old woman with blur and diplopia demonstrated a right optic neuropathy and limited ductions bilaterally. Neuroimaging revealed a right optic nerve sheath meningioma and left intracavernous arachnoid cyst. She was conservatively managed with neurosurgical surveillance for 1.5 years, until her diplopia worsened. Ocular motility re-evaluation demonstrated a worsening left abduction deficit, suggesting interval change of the intracavernous cyst, rather than the meningioma.
Conclusion:
There are only a few reported cases of cranial nerve VI palsy secondary to a cavernous sinus arachnoid cyst. However, this is the first reported case in a patient with a concurrent optic nerve sheath meningioma, and the first case demonstrating progressive worsening of a sixth cranial nerve palsy from an intracavernous arachnoid cyst. Determining which comorbidity caused worsening of symptoms played a critical role in the management of this patient.
Keywords
Introduction
Optic nerve sheath meningiomas (ONSM) are fairly rare, accounting for 1%–2% of all orbital tumors. 1 They occur most often in adult women and have a natural history of slowly progressive optic neuropathy and vision loss, which can be highly variable. 1 ONSM can also cause diplopia and ductional limitations due to mass effect in the orbit. Arachnoid cysts are quite rare as well, with a frequency of 1% of all intracranial space-occupying lesions. 2 Intracavernous arachnoid cysts are even more rare and can cause ductional limitations and diplopia due to cranial nerve (CN) palsies.3–6 To the best of our knowledge, there have been no previously reported cases of progressive worsening of a sixth CN palsy from an intracavernous arachnoid cyst or of co-occurrence of an ONSM with an intracavernous arachnoid cyst.
The purpose of this manuscript is to present a case of progressive CN VI palsy secondary to intracavernous arachnoid cyst, as well as to report the rare co-occurrence of intracavernous arachnoid cyst and ONSM.
Case description
A 67-year-old woman presented with complaints of blur in the right eye and occasional diplopia for the past 6 months. There was no associated pain. Ocular history was unremarkable. Systemic history was remarkable for hypertension and hypercholesterolemia.
Best-corrected visual acuity was OD 20/30 and OS 20/20. All Ishihara color plates were correctly identified in each eye. There was a 1.5 log relative afferent pupillary defect in the right eye. Humphrey visual fields demonstrated a dense inferior arcuate defect and superior temporal defect OD and were full OS. Exophthalmometry measurements were OD 22 mm and OS 21 mm. Ductions were remarkable for a right supraduction deficit (60% normal ductional ability) and possible mild limitation of right abduction (95%) and adduction (95%), as well as a mild left abduction deficit (90%). Prism cover testing in primary gaze found 2 prism diopters (PD) of esodeviation. In upgaze, there was 8 PD exodeviation and 8 PD left hyper (LH) deviation. In downgaze, there was 3 PD exodeviation. In right gaze, there was 4 PD esodeviation, and in left gaze, there was 8 PD esodeviation and 2 LH deviation (Figure 1). Ocular health assessment was remarkable for asymmetric optic disk cupping at 0.8/0.9 OD and 0.6/0.6 OS, with no edema, optociliary shunt vessels, or definite pallor. Intraocular pressures were normal in each eye. Optical coherence tomography (OCT) demonstrated thinning of the neuroretinal rim and retinal nerve fiber layer, as well as ganglion cell thinning OD, suggestive of a right optic neuropathy.
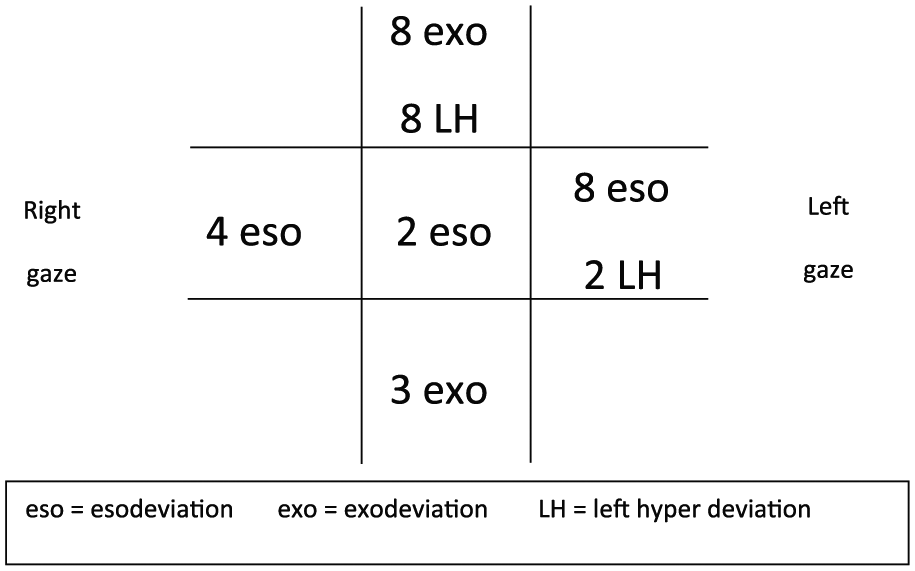
Cover test results in initial presentation. Note that right hyperdeviation in upgaze secondary to the right ONSM, and an increased esodeviation in left gaze, thought to be related to the left intracavernous arachnoid cyst.
A magnetic resonance imaging (MRI) of the brain and orbits with and without contrast was remarkable for a right ONSM accounting for the right optic neuropathy and supraduction deficit, as well as a small left cavernous sinus cystic lesion accounting for the mild left abduction limitation (Figure 2). The cyst followed cerebrospinal fluid (CSF) signal on T1, T2, and FLAIR sequencing and did not exhibit restricted diffusion, suggestive of an arachnoid cyst.
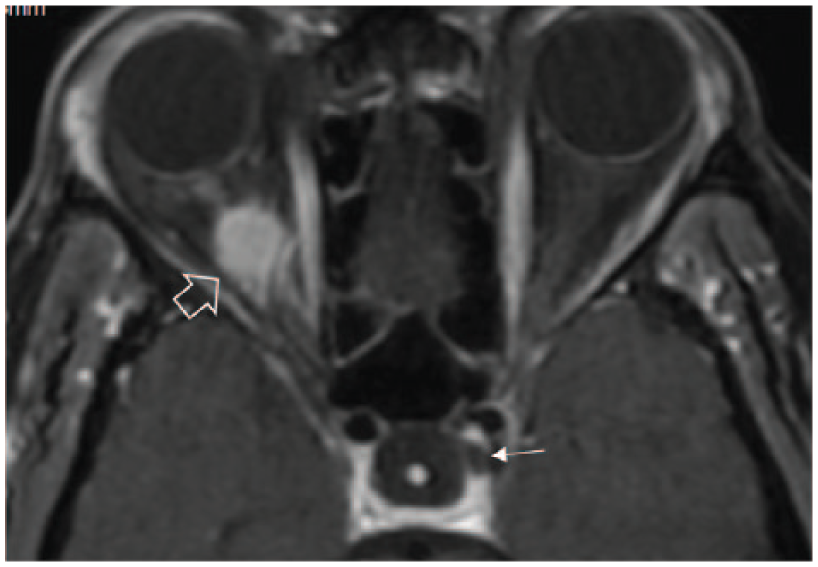
T1-weighted MRI with contrast. Note the enhancing right ONSM (large open arrow) and hypointense left intracavernous arachnoid cyst (small thin arrow).
The patient was under neurosurgical surveillance; symptoms and exam findings remained stable. However, after 1.5 years, she complained of worsening vision. When she reported these progressive visual symptoms at neurosurgery follow-up, it was thought that the most likely etiology was progressive worsening of the ONSM. Therefore, radiation therapy was considered pending repeat neuro-ophthalmic evaluation.
At the neuro-ophthalmic re-evaluation, all measures of afferent visual function were stable, including no worsening of her visual acuity to suggest growth of the right ONSM. Efferent testing was remarkable for a significantly worsened left abduction deficit, with abducting ability now at only 50%, decreasing from 90% on initial presentation. There was an associated increased esodeviation in left gaze, now at 20 PD esodeviation. Ductional ability of the right eye was fairly stable (Figure 3). These findings were suggestive of interval enlargement of the left intracavernous cyst rather than interval change of the right ONSM. To alleviate diplopia, 15 PD of base-out prism to achieve single vision in primary gaze was prescribed and dispensed in the form of a Fresnel prism over the right eye.
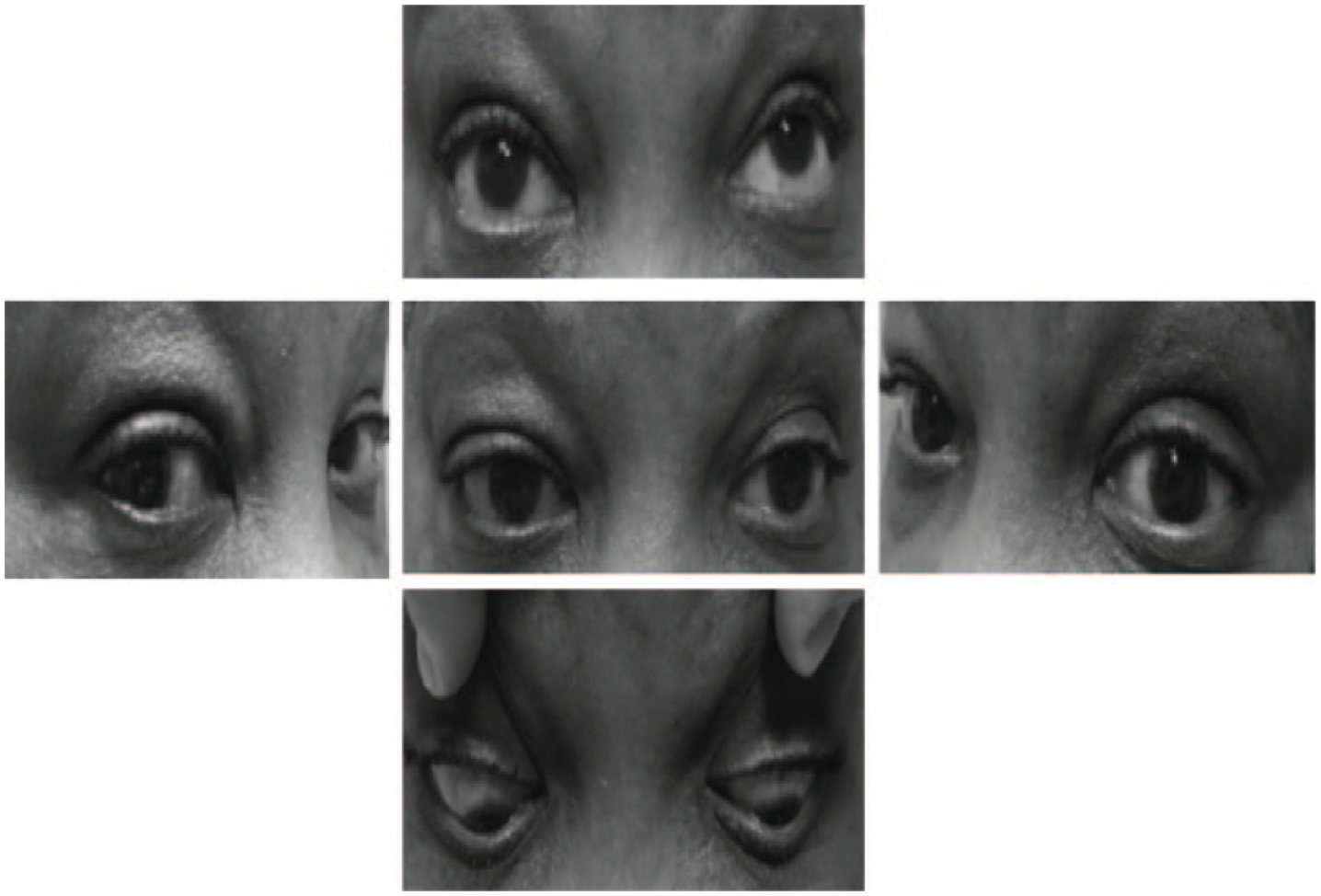
Ocular motilities at the time of worsening symptoms. Note the right supraduction and left abduction deficits.
Repeat MRI of the brain and orbits with and without contrast confirmed stability of the ONSM. The left intracavernous arachnoid cyst was again observed and demonstrated potential mild expansion. Due to differing radiology facilities and slice positioning, the images could not be definitively compared for interval change (Figure 4). Enlargement of the cyst and subsequent increased compression of the left sixth CN was presumed based on the clinical presentation. Radiation treatment was obviated, and the patient has remained under neurosurgical surveillance. There was no improvement of the left sixth nerve palsy over the next year, excluding a vasculopathic sixth CN palsy. There remains no noted abnormality of the third, fourth, or first and second divisions of the fifth CNs on the left side. The patient’s symptoms remain adequately controlled, now with ground-in prism glasses. She continues to be managed conservatively with neurosurgical surveillance.
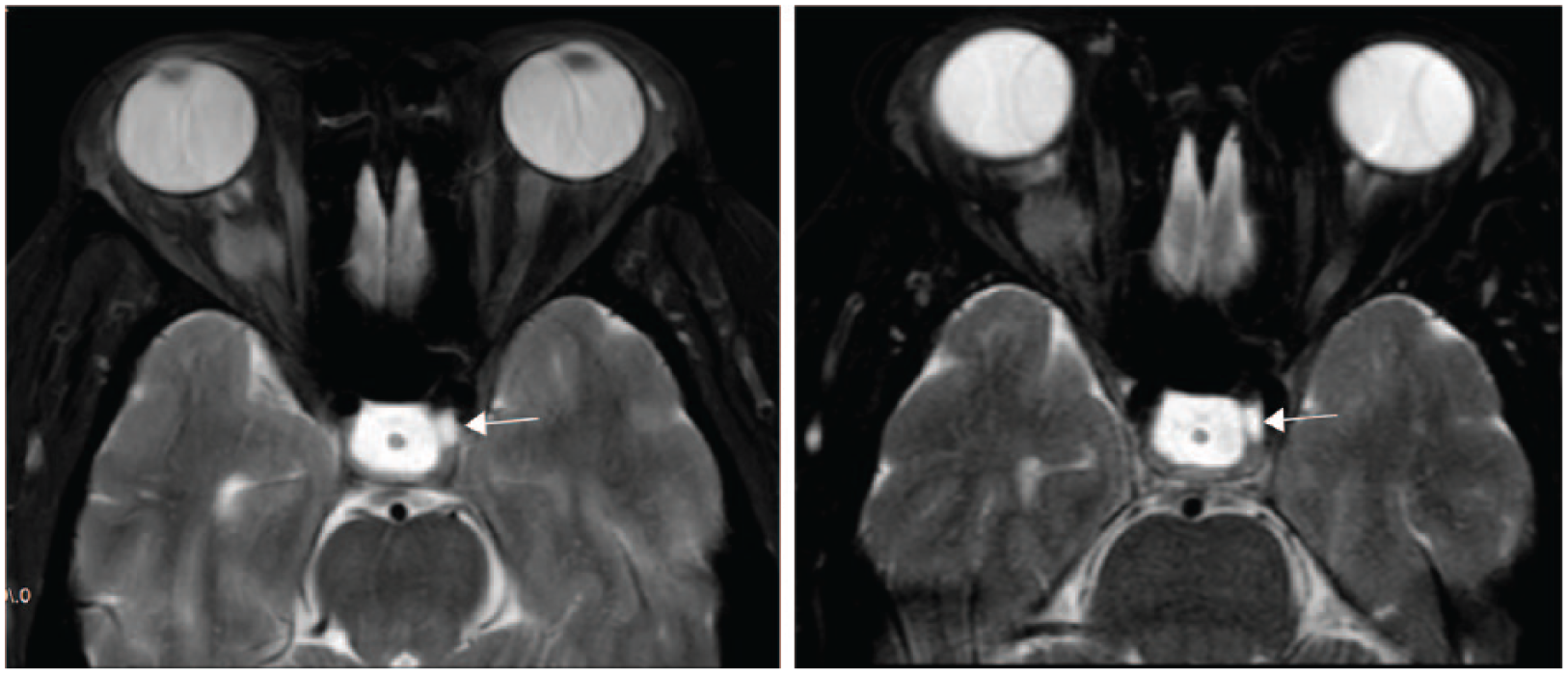
T2-weighted MRI on initial evaluation (left) and 1.5 years later after worsening diplopia (right). Note the hyperintense left intracavernous arachnoid cyst (arrow). It is difficult to assess for interval change due to differing slice position.
Discussion/conclusion
ONSMs can cause abnormal function of both the afferent and the efferent visual system. Treatment can be controversial and patients are often managed conservatively if they remain stable. Due to possible adverse effects, radiation therapy often becomes a treatment recommendation only when there is documented interval change. 1
Arachnoid cysts can be congenital or acquired, with radiologic features including homogeneous low density on CT imaging, T1 hypointensity, T2 hyperintensity, FLAIR hypointensity, and no restricted diffusion on MRI imaging. 7 They may remain stable, but can also demonstrate progressive enlargement. 8 They may be treated neurosurgically with fenestration to decompress the cyst and relieve the effects of pressure. Intracavernous arachnoid cysts are rare, but have been documented to cause cranial neuropathies.3–6 To the best of our knowledge, there have been only two previously reported cases of intracavernous arachnoid cysts causing a CN VI palsy, as in this case.3,4 Neither of these demonstrated progressive worsening. There has not been a previously reported case of expansion of an intracavernous arachnoid cyst.
Although progressive enlargement of the intracavernous arachnoid cyst could not be definitively identified on neuroimaging due to differing facilities and slice positioning, the MRI did rule out any other causative structural etiology for the progressive left abduction deficit. The lack of improvement with time ruled out an overlying vasculopathic sixth CN palsy. There were no clinical features, symptoms, or interval fluctuation to suggest myasthenia gravis. Therefore, this suggests a worsening left sixth CN palsy secondary to expansion of the left intracavernous arachnoid cyst. The fact that no other intracavernous CN involvement has been noted confirms that any enlargement of the cyst would not be great enough to compress the nerves running in the lateral wall of the sinus. Thus, enlargement of the cyst may be subtle, with slight increased mass effect on the sixth CN, and difficult to identify with certainty radiologically. Ultimately, the burden of proof lies in the clinical examination, which does not explain any alternate etiology for the progressive left abduction limitation other than enlargement of the left intracavernous arachnoid cyst.
The fact that both a fairly rare ONSM and a rare intracavernous arachnoid cyst were found in the same patient makes this a unique case. More importantly, the documentation of progressive worsening of a sixth CN palsy secondary to expansion of an intracavernous arachnoid cyst is an essential addition to the literature. To our knowledge, this is the first reported case of worsening ocular motility due to increased compression of any CN in the cavernous sinus by an expanding arachnoid cyst.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Consent was obtained from the patient to take and use images in this manuscript.