
Abstract
Purpose:
To present our experience treating hypotony maculopathy with a simple, minimally invasive, and removable ab interno tube Ahmed glaucoma valve occlusion.
Methods:
Under topical anesthesia a 5–0 polypropylene suture (Prolene; Ethicon) was inserted into the Ahmed glaucoma valve tube. The length of the tube was measured, and an external suture cauterization was performed to allow an easier and safer fixation in the tube. The suture was introduced into the tube itself with the viscoelastic 27-gauge cannula.
Results:
This technique was performed in three cases of hypotony maculopathy with a complex history of medical treatments: a 4-year-old boy with Donnai-Barrow syndrome and previous pars plana vitrectomy that developed hypotony maculopathy the day after Ahmed glaucoma valve insertion and two male patients (69 and 49 years old) that underwent hypotony maculopathy after cyclophotocoagulation as a last option to reduce intraocular pressure. One of the men had three filtering surgeries, two 5-fluorouracil needlings and Ahmed glaucoma valve insertion. The other male patient had keratoplasty and posterior Ahmed glaucoma valve insertion. In the three cases, both hypotony and maculopathy were reversed within a week and a month, respectively, after Ahmed glaucoma valve occlusion with no complications. When hypotony maculopathy develops it seems suitable to occlude completely the Ahmed glaucoma valve tube to swiftly reverse clinical and anatomic changes.
Conclusion:
Intraluminal Ahmed glaucoma valve occlusion with cauterized suture is a simple, quick, reversible, and effective technique that may offer a minimally invasive way to resolve hypotony maculopathy in complex cases and avoid severe loss of vision.
Introduction
Historically, hypotony maculopathy (HM) is an uncommon condition typically characterized by low intraocular pressure (IOP), associated with reduced central vision, triggering optic nerve swelling, and folding of the retina and/or choroid1,2 or other structural changes. 3 HM incidence increased to 20% after the introduction of glaucoma-filtering surgery,4,5 and it is known that (1) male sex, (2) myopia, (3) primary filtering surgery with an antifibrotic agent, and (4) young age (less than 60 years) are all risk factors associated with this condition. 6 Early detection and resolution of HM is essential since permanent chorioretinal changes and poor visual outcome can occur without treatment.
The use of glaucoma drainage devices (GDD) is becoming more frequent in the treatment of both refractory glaucoma and in first filtration procedures and leads to some common, but benign conjunctival complications. 7 Nevertheless, HM is a serious clinical problem that may present after GDD implantation. Ahmed glaucoma valve (AGV) (New World Medical, Inc., Rancho Cucamonga, LA, USA) has been shown to lower the incidence of postoperative hypotony than non-valved GDD8–10 However, HM occurs despite valve design or fluid flow optimization11,12 and its management is difficult because it does not completely resolve (IOP increase is enough to reverse the structural alterations) with medical treatments.8,13,14 In addition, it has been reported that cyclophotocoagulation could lead to ciliary body inhibition, generating an additional hypotony added to the AGV overfiltration itself. 1
This article presents our experience treating HM with a simple, minimally invasive, and removable ab interno tube AGV occlusion.
Methods
The surgery can be performed under topical anesthesia. A paracentesis was created at limbus 90 degrees away from the tube followed by viscoelastic (Hyaluronic acid; 10 mg/mL; Biolon®, Tedec-Meiji Farma) injection into the anterior chamber. A 5–0 polypropylene suture (Prolene; Ethicon) was inserted into the AGV tube via a second paracentesis site created in the same meridian of the GDD. The length of the tube was measured, and an external suture cauterization was performed after trimming it to allow an easier and safer fixation in the tube, thus totally occluding the lumen. The suture was introduced into the tube itself with the viscoelastic 27-gauge cannula until the occlusion of the tube was concluded. VisionBlue (0.006% version of Trypan blue, DORC, Zuidland, The Netherlands) was used to visualize flow through the tube, thus being sure that it was totally occluded (see video as supplementary online material). In case of necessity, the suture could be removed with a 23G Grieshaber Revolution® DSP (Alcon) vitreoretinal instrument.
The procedures adhered to the tenets of the Declaration of Helsinki, and patients signed a consent form for scientific purposes.
Results
This technique was performed in three cases of HM with a complex history of medical treatments.
Case 1
A 4-year-old boy presented with Donnai-Barrow syndrome and previous pars plana vitrectomy with 5000 cST silicone for giant retinal tear in his left eye. After 2 years of silicone extraction, IOP measured with Goldman applanation tonometer was 30 mmHg with maximum IOP lowering medications and visual acuity of hand movement. An AGV was implanted without complications. The day after IOP decreased to 2–4 mmHg with a choroidal detachment. This condition remained for a month after suture reinforcements and anti-inflammatory treatment with dexamethasone phosphate (1 mg/mL; Dexafree®, Laboratoires Unither, France). A valve tube occlusion, as described above, using general anesthesia, was performed without intra- or postoperative complications and IOP increased to 7–8 mmHg after 1 week. Complete resolution of structural changes was achieved 1 month after the surgery. Follow-up 1 year later found it remained stable.
Case 2
A 69-year-old man consulted due to high IOP with maximum number of glaucoma medications. His ocular history revealed three filtering surgeries and two 5-fluorouracil needlings. An AGV was inserted, and after 8 months a cyclophotocoagulation was performed due to maintained high IOP. At 2 weeks, IOP decreased to 3 mmHg, and a choroidal detachment was detected with visual acuity of counting fingers. Two drainages were performed, but hypotony remained with folding of the retina. Following the drainages, the patient underwent the described surgery, under topical anesthesia, without intra- or postoperative complications. We observed that the IOP regressed to 6–7 mmHg in a week and his best-corrected visual acuity (BCVA) improved to 0.2 Snellen 1 year later with an IOP of 10 mmHg.
Case 3
A 49-year-old man consulted due to progressive visual loss after a cyclophotocoagulation 2 weeks before. BCVA was 0.04 Snellen. His ocular history revealed a keratoplasty and posterior AGV insertion. Fundus examination and optical coherence tomography (OCT) showed retinal folds (Figure 1, left). Increased choroidal thickness was detected by echography. Tube occlusion with suture insertion was done, under topical anesthesia, without complications intra- or postoperatively. Maculopathy was resolved in a month and corroborated with OCT images (Figure 1, right). No reliable IOP measurements were taken pre- and post-suture insertion due to cornea condition.
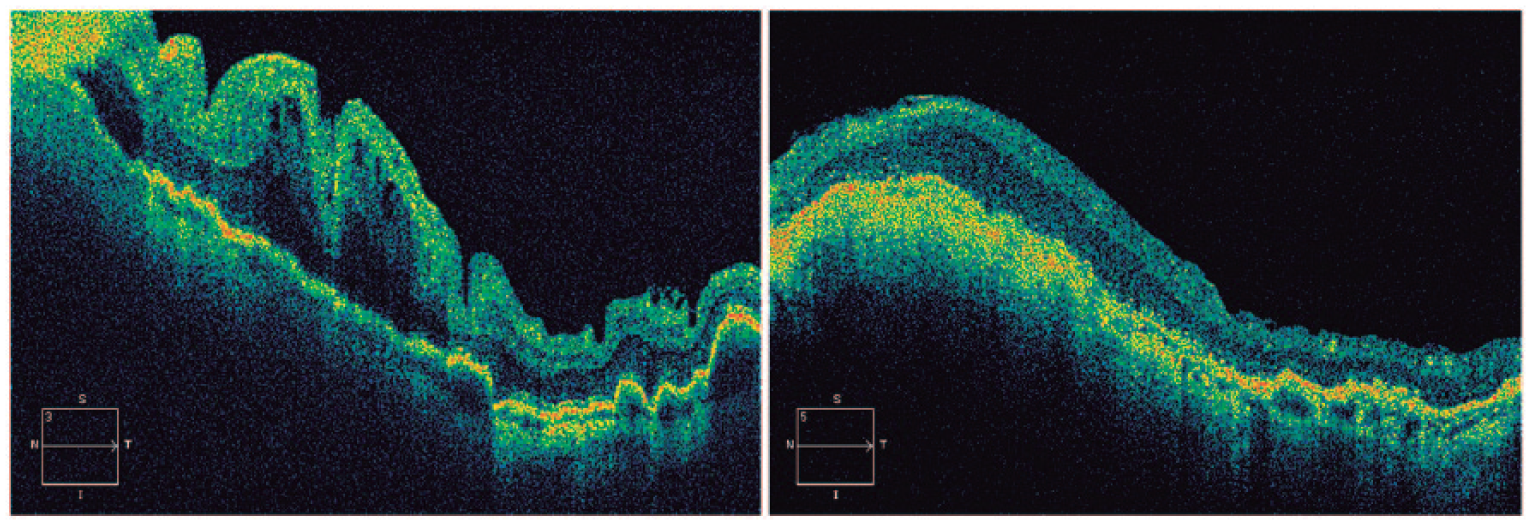
Retinal folds of case three (49-year-old male): (left) preoperative OCT image and (right) postoperative OCT image at 1 month after Ahmed glaucoma valve tube occlusion.
Conclusion
Tube occlusion with polypropylene had been first proposed in Baerveldt GDD to maintain anterior chamber during phacoemulsification 13 and was systematically applied during Baerveldt GDD implantation with variable results after removing the occlusion. 15
Other alternatives like tube or complete GDD removal to reverse hypotony may cause conjunctival and scleral damage due to the invasive nature of the intervention, 16 and the patient may again need additional medication and surgery to control IOP. Tube ligation is another alternative to reverse hypotony, but it has shown to have a relatively high rate of failure. Stein et al. 8 found a rate of failure in the procedure that varied according to the suture material used from 20% to 50% including primary and secondary revisions. These failures required additional surgery.
Comparing with the other alternatives discussed earlier, the surgical technique presented here is more easily removable under topical anesthesia; it does not require special materials, results in no damage to the conjunctiva, and thus allows future glaucoma surgery alternatives if needed. In addition, a resorbable suture could be used as an alternative to prevent removal maneuvers, albeit noted that this is not exempt from certain complications.
Nevertheless, the set of three complex cases described in this study is not large enough to comprehensively assess the beneficial effects of this procedure, warranting a larger clinical study with more patients.
In conclusion, intraluminal AGV occlusion with cauterized suture is a simple, relatively quick, reversible, and effective technique that may offer a minimally invasive way to resolve HM in complex cases and avoid severe loss of vision.
Footnotes
Acknowledgements
We sincerely thank Justin C d’Antin and Michael J Edel for their assistance with the English edition of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.