
Abstract
Introduction:
Phaco-antigenic glaucoma occurs in less than 1% of cataract surgeries. Managing this rare complication is challenging, especially when there are few documented cases reported. We describe the challenges of managing a case of bilateral phaco-antigenic glaucoma following uncomplicated cataract surgery requiring viscocanalostomy.
Case description:
An 82-year-old atopic lady presented with a 2-day history of painful injected right eye. She was 4 days post left and 8 days post right uncomplicated cataract surgery. On examination, the anterior chambers were deep with no hypopyon. Intraocular pressure was raised at 38 mmHg in the right eye and 24 mmHg in the left eye initially. However, intraocular pressure remained uncontrolled despite maximum medical treatment; she attended A + E six times within 11 days with intraocular pressures of up to 48 mmHg in the right eye and 46 mmHg in the left eye. A vitreous biopsy was reported negative for infective organisms. Eventually, bilateral viscocanalostomies were performed and vision improved to 0.24 logMAR in both eyes with intraocular pressures of 8 mmHg in the right eye and 10 mmHg in the left eye.
Conclusion:
We present a rare presentation of phaco-antigenic glaucoma following an uncomplicated cataract surgical procedure with good results following timely intervention.
Introduction
Phaco-antigenic glaucoma occurs in less than 1% of cataract surgeries.1–3 Managing this rare complication is challenging, especially when there are few documented cases reported. We describe the challenges of managing a case of bilateral phaco-antigenic glaucoma following uncomplicated cataract surgery requiring viscocanalostomy.
Case description
An 82-year-old asthmatic lady with a history of atopy (latex and codeine) underwent bilateral uncomplicated cataract surgery. She was otherwise fit and well and had no other relevant past medical or surgical history. She has no family history of glaucoma. She presented to eye casualty (8 days post right eye (RE) and 4 days post left eye (LE) surgery) with a 2-day history of painful, injected RE and blurry vision.
Best-corrected vision was 0.22 logMAR RE and –0.08 logMAR LE. Slit-lamp examination revealed an injected conjunctiva, corneal oedema and mild anterior chamber inflammation (+1 cells) in the RE with no hypopyon. Vitreous was clear with no retinal haemorrhages seen. The anterior and posterior segment in the LE was quiet. The intraocular pressure (IOP) was 38 mmHg RE and 24 mmHg LE. The optic disc was healthy in both eyes.
In light of the history and findings, the patient was treated for early postoperative raised IOP with G. apraclonidine 1% and oral acetazolamide 250 mg. IOP dropped to 27 mmHg. She was continued on oral acetazolamide as well as postoperative G. tobramycin/dexamethasone drops.
Management of uncontrolled IOP
A day later, she re-presented in accident and emergency with severe headache, nausea and vomiting. Best corrected visual acuity (BCVA) had dropped to HM (hand movements) RE and 0.60 logMAR LE. Both eyes were injected and had corneal oedema and mild anterior chamber inflammation (+1 cells). The anterior chamber remained deep with no hypopyon. IOP was 48 mmHg RE and 46 mmHg LE. There was no clear view of the fundus RE due to corneal oedema but no obvious vitreous cells or retinal haemorrhages LE.
The patient was commenced on medical treatment including G. travoprost, G. brinzolamide, G. apraclonidine and intravenous (IV) acetazolamide. However, IOP remained refractory at 48 mmHg RE and 36 mmHg LE. IV mannitol was given and IOP eventually subsided to 22 mmHg RE and 18 mmHg LE. Patient was continued on G. travoprost, G. apraclonidine, G. brinzolamide and G. cyclopentolate. Corticosteroid-induced glaucoma was suspected as IOP remained high postoperatively despite treatment. Therefore, G. tobramycin/dexamethasone was switched to G. ketorolac and G. chloramphenicol.
Over the next 11 days, the patient re-presented to eye casualty and accident and emergency six times with uncontrollably high IOP 22–36 mmHg RE and 28–40 mmHg LE. Despite no presence of hypopyon, an infective cause of bilateral raised IOP and anterior segment inflammation needed to be ruled out. In view of this, a multidisciplinary approach was taken with an urgent vitreoretinal (VR) opinion. An RE vitrectomy was performed with vitreous biopsy and intravitreal vancomycin and ciprofloxacin given. Postoperatively G. tobramycin/dexamethasone was re-prescribed to both eyes as it was becoming more apparent that it was not corticosteroid-induced glaucoma/hypertension. The vitreous sample was negative for herpes simplex virus (HSV), herpes zoster virus (HZV), venereal disease research laboratory (VDRL) and cytomegalovirus (CMV) and IOP remained high. Interestingly, white blood cells were seen on Gram staining.
Uncontrolled IOP despite maximum medical treatment was a concern. Therefore, surgical options were discussed with the patient. Viscocanalostomy was performed as a less invasive approach (Figures 1 and 2). Patient was commenced on G. loteprednol etabonate postoperatively for 1 month. At 1 year post viscocanalostomy, BCVA was 0.12 logMAR RE and 0.14 logMAR LE, and pressures remained well controlled at 9 mmHg RE and 10 mmHg LE.
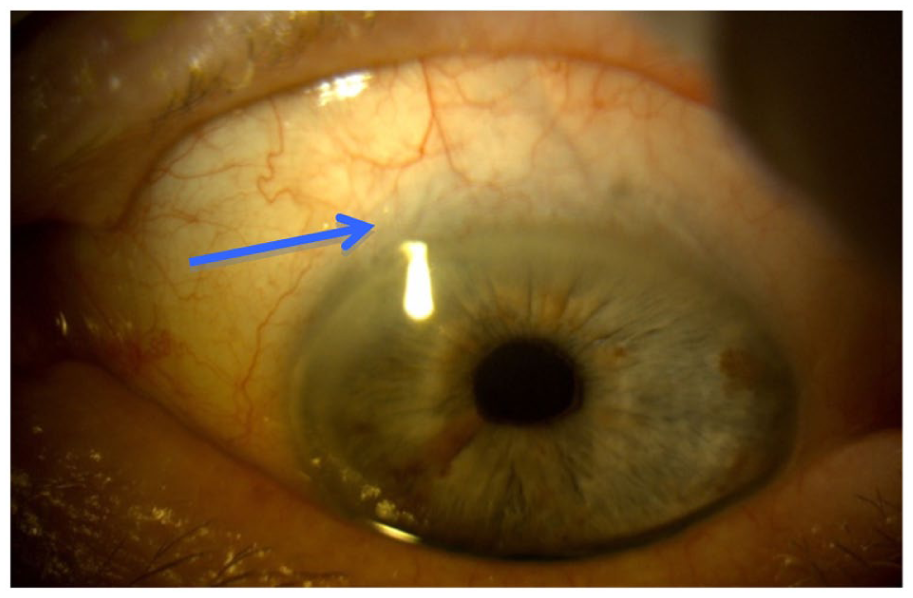
Demonstration of the left viscocanalostomy site.
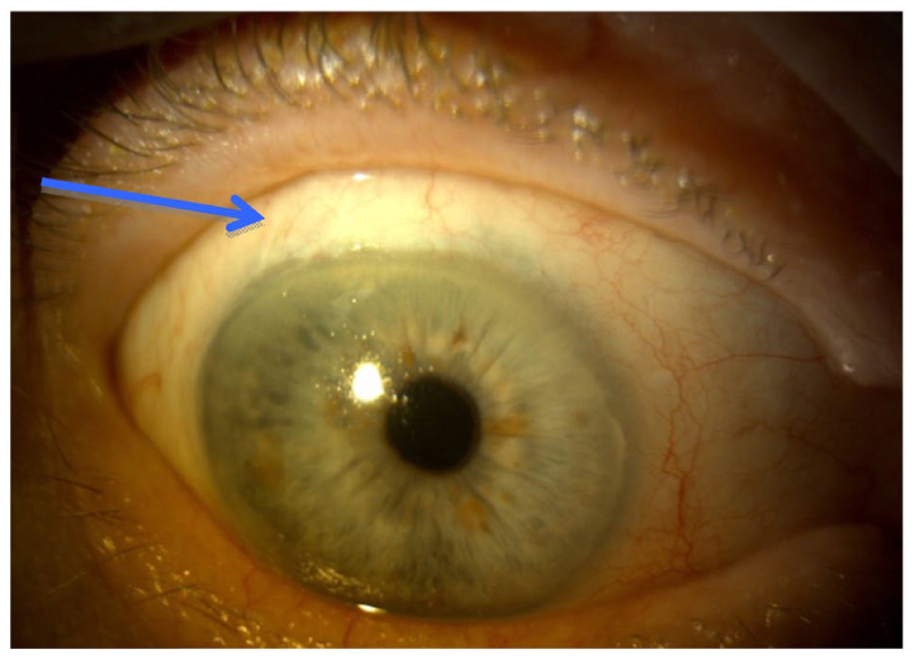
Demonstration of the right viscocanalostomy site.
Discussion
Uncontrolled high IOP, post cataract surgery even if uncomplicated, can pose many challenges. We would like to discuss the various differential diagnoses of this case and demonstrate that phaco-antigenic glaucoma as the only plausible diagnosis in this patient. The differential diagnoses include early postoperative raised IOP, corticosteroid-induced glaucoma/hypertension, acute post-cataract infective endophthalmitis, Posner–Schlossman syndrome, aqueous misdirection, toxic anterior segment syndrome (TASS) and phaco-antigenic glaucoma (Table 1).
List of differential diagnoses with arguments for and against.
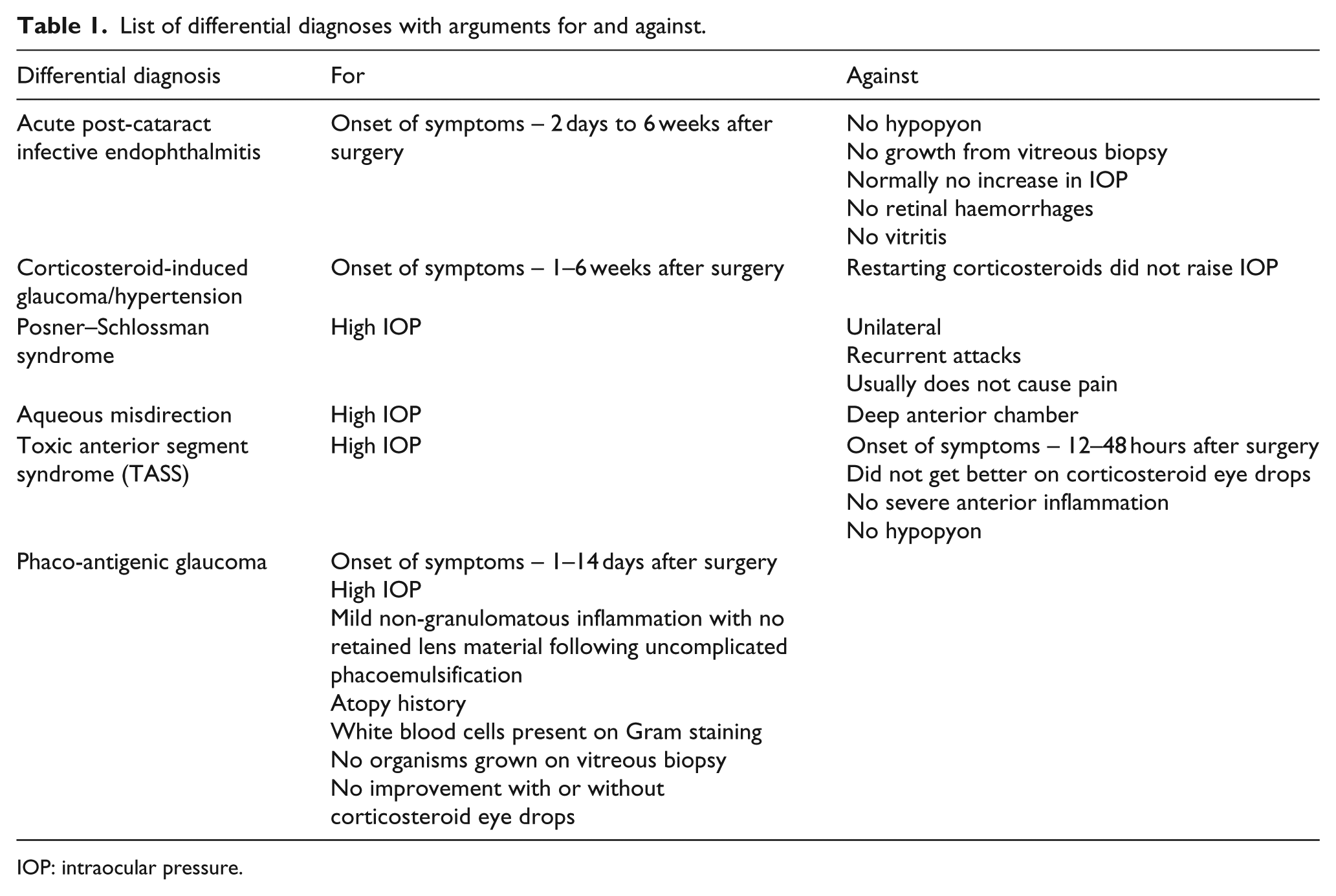
IOP: intraocular pressure.
Differential diagnosis
Initially, early postoperative raised IOP was presumed diagnosis. This is extremely common occurring in 2.3%–8.9% of cataract surgeries4,5 but subsides with treatment. Ophthalmic viscosurgical devices (OVDs) commonly cause postoperative raised IOP. Even with the removal of OVD at the end of surgery, it can be compartmentalised behind the intraocular lens (IOL) or the posterior chamber. 6 It generally lasts a couple of days and does not require prolonged treatment.7,8 Our patient however continued to have raised IOP despite appropriate treatment.
Corticosteroid-induced glaucoma/hypertension was postulated on re-presentation of uncontrollable IOP. Researchers have shown the presence of corticosteroid-induced glaucoma/hypertension in nine different species. 9 Corticosteroids alter trabecular meshwork morphology causing reduced aqueous outflow and a rise in IOP. 10 A third of the normal population will be sensitive to steroids.11,12 Risk factors include family history of primary open angle glaucoma, high myopia, type 1 diabetes and connective tissue disease. 13 Typically corticosteroid-induced glaucoma/hypertension occurs between 3–6 weeks of continuous topical ophthalmic corticosteroid use, but a rise can be demonstrated within 1 week.14,15
Drops were switched from G. tobramycin/dexamethasone to G. ketorolac and G. chloramphenicol. Corticosteroid-induced glaucoma/hypertension usually normalizes after cessation of corticosteroids in the following 3–4 weeks, and irreversible elevation of pressure is unusual occurring if use is prolonged. 16 However, in our patient, pressures remained uncontrolled despite the use of alternative non-corticosteroid drops for 3 weeks. Corticosteroids were restarted as the inflammation was not adequately controlled with non-corticosteroids and second there was no change/improvement in IOP. Furthermore, there was no further increase in IOP after reinstating topical corticosteroid treatment.
Acute post-cataract infective endophthalmitis has similar early onset of symptoms and signs with 75% of patients presenting within 1 week of cataract surgery. 17 One would expect a more severe inflammatory process with hypopyon or retinal haemorrhages, and worsening of symptoms on topical corticosteroids, which were not demonstrated. In total, 90% of vitrectomy specimens have a positive culture, 17 whereas no organisms were detected on vitreous biopsy in this case.
Posner–Schlossman syndrome and aqueous misdirection can both cause high IOP. However, Posner–Schlossman syndrome is usually painless, unilateral and has a history of recurrent attacks, which are not seen here. Aqueous misdirection was also considered. However, in our case, the anterior chamber was consistently deep as opposed to shallow anterior chamber in aqueous misdirection syndrome.
TASS must also be considered in the differential diagnosis. TASS is an acute severe anterior intraocular inflammation secondary to many factors including denatured OVD, cleansing solution used in sterilizing surgical instruments, skin preparations, insertion of air into the anterior chamber, intraocular or topical medication and preservatives.18–24 Monson et al. 25 first named TASS following several reported cases of severe anterior chamber infections caused by toxic substances in 1980s. Patients usually present postoperatively with reduced vision and corneal oedema (exactly like this case). It does not involve the vitreous. Secondary glaucoma is caused by damage to the trabecular meshwork. 26 Patients with TASS usually has onset of symptoms 12–48 h after surgery, have severe anterior inflammation with occasional hypopyon and tend to do well on topical corticosteroids, 27 whereas our patient seemed to show no significant improvement despite intensive corticosteroid use.
Phaco-antigenic glaucoma
Straub first described phaco-antigenic glaucoma in 1919.28,29 Anaphylaxis was used to describe this acute onset in inflammation, but this is a misnomer as it does not involve an allergic reaction. Immunoglobulin G binds to lens particles, which forms an immune complex in an Arthus-type immune reaction.30,31 This leads to a granulomatous reaction causing increased IOP secondary to blocking the trabecular meshwork. Lens proteins have been found to be present in low quantities in the aqueous of normal individuals.32,33 However, high concentrations of lens proteins are insulated within the lens capsule. Therefore, there needs to be an alteration in lens structural integrity by trauma or surgery to create a response.
Clinical presentation occurs 1–14 days post surgery, but latency has been documented up to 59 years. 32 Signs include conjunctival injection, corneal oedema and anterior chamber/anterior vitreous inflammation. Inflammation is usually granulomatous, but non-granulomatous inflammation has been reported as in our case. Definitive diagnosis of phaco-antigenic glaucoma requires white blood cells (in particular polymorphonuclear leukocytes, epithelioid and giant cell and mononuclear cells) 34 present in a vitreous biopsy. These were isolated during Gram staining in our case. No retained lens matter was demonstrated following uncomplicated phacoemulsification. The latency at presentation and signs seen in our patient are consistent with this diagnosis.
We postulate that an immune reaction was precipitated on exposure to lens particles during the first cataract operation. The first presentation, 8 days later, also coincided with a similar response in the second eye 4 days post operation. The earlier presentation in the second eye could be explained by the fact that this was already sensitized following the onset of the immune reaction in the first eye.
Phaco-antigenic glaucoma is a rare complication following cataract surgery. In this case, we have excluded other differential diagnosis making this the most likely cause of the patient’s condition. We believe that this is the first reported case of phaco-antigenic glaucoma treated successfully by viscocanalostomy.
Challenges to management of phaco-antigenic glaucoma
There is very little published evidence on this condition.28,29,31 As the patient failed to respond to maximum medical treatment and continued to have uncontrolled IOP, a surgical option was offered. Surgical treatment and timing of surgery are never to be taken lightly. A holistic approach was taken, and a detailed discussion with the patient on various surgical options including trabeculectomy, glaucoma drainage devices and viscocanalostomy was offered.
Viscocanalostomy is a non-penetrating surgical treatment for glaucoma, which aims to lower IOP with a potentially lower incidence of complications compared to trabeculectomy. 35 There were no complications post viscocanalostomy. The patient was off treatment 1 month later, and vision and pressures have remained excellent (Figures 1 and 2).
Conclusion
Phaco-antigenic glaucoma is a rare cause of glaucoma following cataract surgery with limited case reports and discussion of management. A diagnosis of phaco-antigenic glaucoma is often difficult in vivo and must be a diagnosis by exclusion. This case highlights the importance of managing high IOP postoperatively with appropriate treatment leading to excellent results. It further demonstrates that non-penetrating surgical option can be a viable treatment for phaco-antigenic glaucoma.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement and the meeting on which it was based were sponsored by Novartis (tracking number OPT19-C005). Novartis did not contribute to the content and all authors retained final control of the content and editorial decisions. Novartis have checked that the content was compliant with the Association of the British Pharmaceutical Industry Code of Practice.