
Abstract
Purpose
To compare enhanced depth imaging in swept-source optical coherence tomography and non–enhanced depth imaging optical coherence tomography in their ability to capture choroidal and scleral details.
Methods
Averaged foveal B-Scans were obtained from 40 eyes of 20 healthy volunteers by swept-source optical coherence tomography with and without enhanced depth imaging. Visibility and contrast of vascular details within the choroid, choroidoscleral junction, and sclera were evaluated by masked readers using an ordinal scoring scale. Outcomes were analyzed using the Wilcoxon signed rank-sum test.
Results
Visibility of the choroidal vascular details (Z = 5.94, p < .001), the choroidoscleral junction (Z = 5.85, p < .001), and the sclera (Z = 6.80, p < .001) was significantly higher with enhanced depth imaging than with non–enhanced depth imaging swept-source optical coherence tomography. Similarly, image contrast was significantly higher with enhanced depth imaging than with non–enhanced depth imaging swept-source optical coherence tomography for the choroidal vascular details (Z = 9.47, p < .001), for the choroidoscleral junction (Z = 9.28, p < .001), and for the sclera (Z = 9.42, p < .001).
Conclusion
Enhanced depth imaging applied to swept-source optical coherence tomography–averaged foveal B-scans enhances visualization of the choroidal details, of the choroidoscleral junction, and of the sclera. This novel modality can easily be implemented in clinics and could improve our understanding of conditions involving the choroid or the sclera.
Keywords
Introduction
The in vivo structure of the choroid in health and disease is incompletely visualized by traditional imaging modalities, including fluorescein angiography, and ultrasonography. 1 Conventional spectral domain optical coherence tomography (SD-OCT) allows visualization of structures beyond the retinal pigment epithelium (RPE), but it is influenced by melanin content in the RPE and light scatters through blood and vessels. 1
In order to improve the visualization of the choroid, Spaide 2 proposed a novel way of acquiring pictures using commercially available SD-OCT: enhanced depth imaging (EDI). Simply put, this technique shifts the focus deeper into the tissue.2–4
The advent of EDI-OCT imaging of the choroid has opened a window for fertile research and a better understanding of physiological and pathological processes of the choroid.1,5–7 Still, EDI-OCT has its weaknesses: external outer border cannot always be visualized and choroidal elements often lack resolution and clarity.8,9
Since the description of EDI, a new generation of OCTs has been made available, based on swept-source technology (SS-OCT). This innovative technology can perform faster, deeper scans, neutralize background noise, and decrease motion artifacts. Swept-source OCT also allows better light exposure since it has a built-in dual balanced detection. As SS-OCT necessitates a narrow-line swept-source, it enables better spectral resolution when compared to SD-OCT. 10 Moreover, the longer wavelength used in commercially available SS-OCT is able to better penetrate deeper tissues than the relatively SD-OCT that operates in relatively shorter wavelengths. 10 Averaged pictures obtained by SS-OCT seem to be more precise in detecting the choroid-scleral interface than by spectral domain EDI-OCT.8,9,11–16 There are, however, trade-offs with SS-OCT.1,17
Regarding the possibility of improving detection of deeper structures by applying the EDI modality to SS-OCT, the arguments that explain the advantage of EDI in SD-OCT should also be valid for SS-OCT. Since the light source has a finite bandwidth and for deeper object’s layers the successive reflected wavelengths are modulated with higher modulation frequencies, the modulation values between successive reflected wavelengths decrease. 18 In this case too, the decrease in the modulation values decreases the resolution of deeper object’s layers and limits the maximal deepest layer that can be resolved. Thus, it is expected that in SS-OCT too, shifting the device closer to deeper layers purposefully and configuring it to place the deeper choroidal sections near the zero optical path difference relative to the reference mirror, the sensitivity of the imaging of those layers will be improved and the resolution will increase. Such a technique, easy to be implemented in clinics, would define new frontiers in imaging of the choroid and could therefore become the gold standard for in vivo analysis of the deepest ocular structures in health and disease.
In this study, we aim to apply the EDI method to SS-OCT, by modifying the image acquisition protocol, based on the technique described by Spaide for SD-OCT.
Methods
This prospective, non-interventional case series was performed in agreement with the tenets set forth in the Declaration of Helsinki. Ethics authorization was acquired from our institutional Ethics Committee.
Participants and imaging protocol
Twenty healthy volunteers aged 18 years or older were prospectively recruited at the ophthalmology department, Shaare Zedek Medical Center, Jerusalem, Israel. All subjects had no known ocular pathology and refractive error below ±2 diopters. OCT scans were obtained without pupil dilatation, in a dark room under the same light scenery, with an SS DRI OCT-1 Atlantis (Topcon Medical Systems Inc., Oakland, NJ, USA; 1050 nm, ver. 9.10). Subjects were imaged by the same experienced operator. All examinations were completed within 3 days. Since no tracking option enabled automated location of the scans in a given patient, the scans were manually located in the same place, using the hyperreflectivity at the vitreoretinal interface of the fovea as an anatomic landmark. For each eye, averaged B-scan lines at the fovea were obtained by two techniques, with the hyperreflectivity at the bottom of the foveal pit as an indicator of correct scan position. Classical pictures were first taken according to the instructions of the manufacturer. Then, according to the method described by Spaide, EDI scans were obtained by bringing the device closer to the anterior surface of the eye to create a reversed figure at the upper portion of the display. Sufficient separation was used to avoid image blurring. 4
Image evaluation
All pictures were transferred to image software. Those obtained by EDI, that presented originally with the choroid up and the retina down, were inverted, so masking of the acquisition technique could be guaranteed. The images were evaluated by four independent, masked ophthalmologists (K.B., J.H., T.L.V., and Y.W.). To evaluate the visibility of the choroidal vascular details, the choroidoscleral junction, and the sclera, each image line was independently evaluated and the percentage of visible structure was graded using a scoring system as described previously by Waldstein et al.: “1, below 10% of the choroidoscleral junction visible; 2, between 11% and 50% of the choroidoscleral junction visible; 3, between 51% and 90% of the choroidoscleral junction visible; and 4, over 90% of the choroidoscleral junction visible.” 19 Furthermore, the overall contrast of the choroidal vasculature, choroidoscleral junction, and the sclera was graded as follows: “1, not visible; 2, poor contrast; 3, medium contrast; and 4, high contrast.” 19 Contrast was defined by the ability to distinguish a specific structure from its surroundings. Specifically, it reflected the ease of identifying choroidal vessels as such, of locating the choroidoscleral junction, and of differentiating the sclera from its environment.
Statistical analysis
SPSS (version 20) was used for statistical analysis. Cohen’s κ was used to evaluate intra-observer reproducibility. Inter-observer reproducibility was assessed using intra-class correlation coefficient (ICC). Gradings of the four assessors were grouped for statistical analysis. Criterion for accepting research hypothesis, alpha (α) = .05.
Results
The mean age (±standard deviation (SD)) was 37.7 ± 8.5 years. EDI images were easily obtained for all eyes. The software provided with the DRI-OCT attempts to average 96 pictures and indicates how many pictures were actually used to get the averaged image we used for comparison. There was no significant difference in the number of averaged eyes between the non-EDI (93.4 ± 6.5) and EDI series (91.9 ± 9.6; p = .4). There was a good inter-observer reproducibility with a Cronbach’s alpha of .849 for averaged measures. Intra-observer reproducibility was assessed for 10 eyes for one observer (J.H.) and was found to be high (κ = .877). The observers’ scores appear in Table 1. For every structure, the frequency of best score (4: corresponding to >90% visibility or excellent contrast) is superior for pictures taken with EDI than with non-EDI.
Frequency of scores with EDI versus non-EDI SS-OCT for each considered structure.
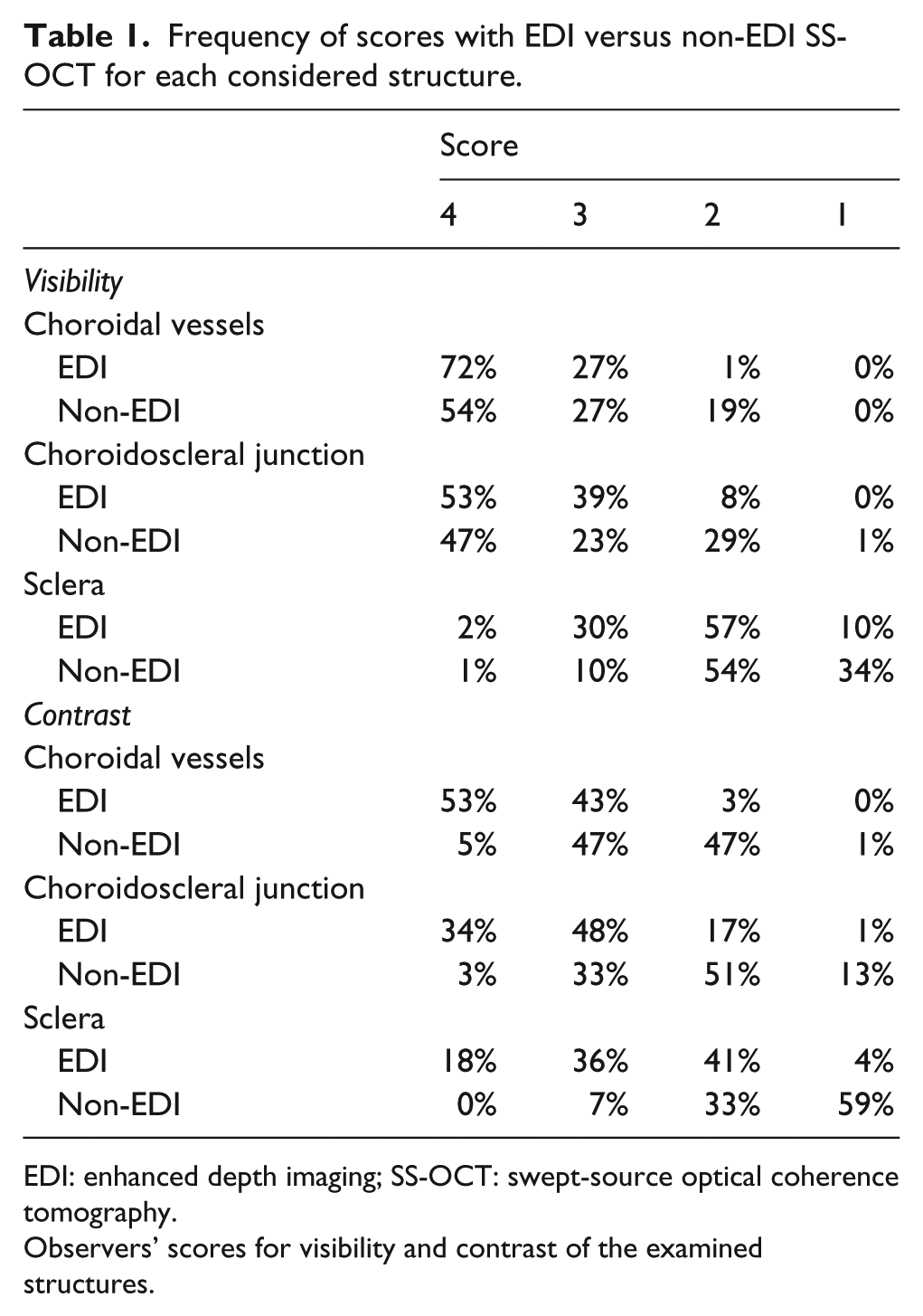
EDI: enhanced depth imaging; SS-OCT: swept-source optical coherence tomography.
Observers’ scores for visibility and contrast of the examined structures.
The superiority of SS-OCT EDI over classically acquired images was substantially more marked in contrast than visibility comparison. For every considered structure, the percentage of best scores (4: corresponding to >90% visibility or excellent contrast and 3: corresponding to 51%−90% visibility or high contrast) is superior for pictures taken with EDI than with non-EDI. On the histogram offering an overall comparative view (Figure 1), EDI appears to be superior to non-EDI SS-OCT for each structure, and this advantage is more pronounced when relating to visibility than contrast.
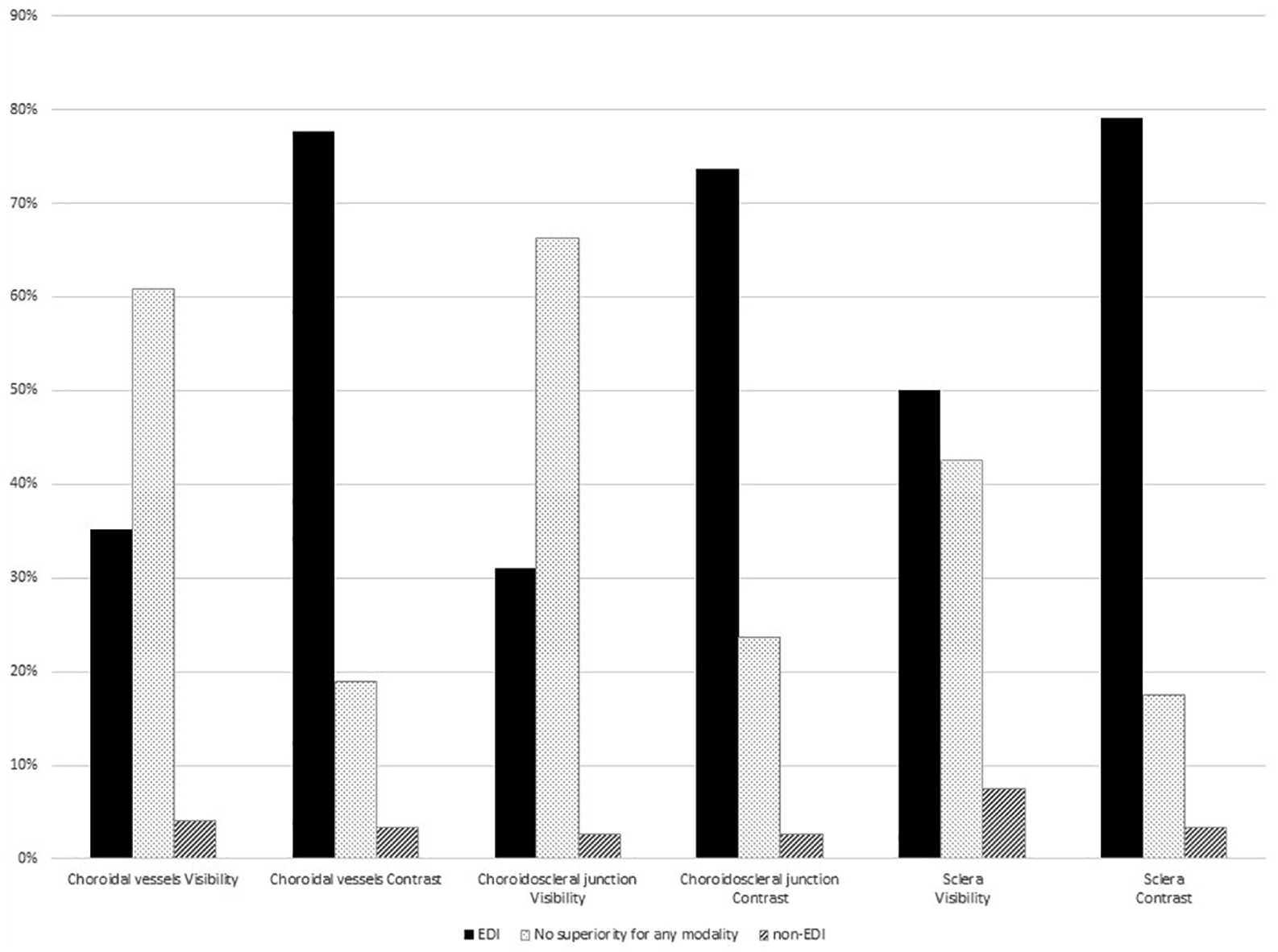
Overall assessment of averaged B-scans taken by SS-OCT with or without EDI at the fovea. This graph shows the clear advantage of EDI over conventional SS-OCT when assessing contrasts, as for each considered structure, most of the eyes obtained a better mark with EDI than with non-EDI. Evaluators also gave better visibility scores for EDI than for non-EDI (N = 148; p < .001 for all compared values).
In the visibility evaluation of the choroidal vessels, 35% of the examined eyes received a better score with EDI and only 4% with non-EDI (Z = 5.94, p < .001). Regarding visibility of the choroidoscleral junction, 31% of the examined eyes received a better score with EDI versus 3% with non-EDI (Z = 5.85, p < .001). For visibility of the sclera, 50% of the eyes received a better score with EDI versus 7% with non-EDI (Z = 6.80, p < .001). On assessment of the contrast of the choroidal vessels, EDI was graded as superior in 78% of the eyes as only 3% of the eyes were better noted with non-EDI (Z = 9.47, p < .001). Concerning contrast of the choroidoscleral junction, 74% of the eyes received a better score with EDI versus 3% with non-EDI (Z = 9.28, p < .001). For contrast of the sclera, 79% of the eyes received a better score with EDI and 3% with non-EDI (Z = 9.42, p < .001).
Discussion
In this study, we describe a new method of obtaining images of the choroid and sclera, by combining EDI and SS-OCT. Applying the EDI method to SS-OCT is easily performed with commercially available devices. As compared to non-EDI SS-OCT, EDI SS-OCT showed significantly superior contrast and visibility for the choroidal vascular details, the choroidoscleral junction, and the sclera (Figures 2 and 3).
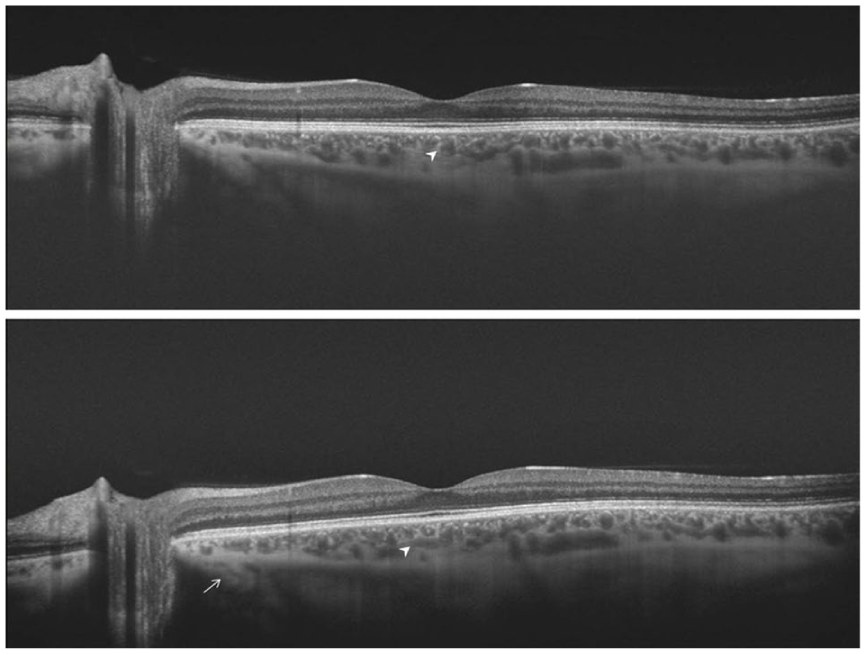
Visibility and contrast enhancement with EDI. The above B-scan was conventionally captured with SS-OCT and the bottom B-Scan using EDI. The texture of the choriocapillaris looks denser when EDI is used. Vascular walls of medium vessels are better discriminated with EDI (arrowheads). EDI enables a better differentiation from its surroundings and a higher visualization of its lumen. Some vessels running through the sclera are captured by EDI (arrows) but are not retrieved on conventional imaging. Regarding this specific eye, the visibility score for the choroidal vessels was 3.0 in conventional pictures and 3.8 with EDI (p < .001).
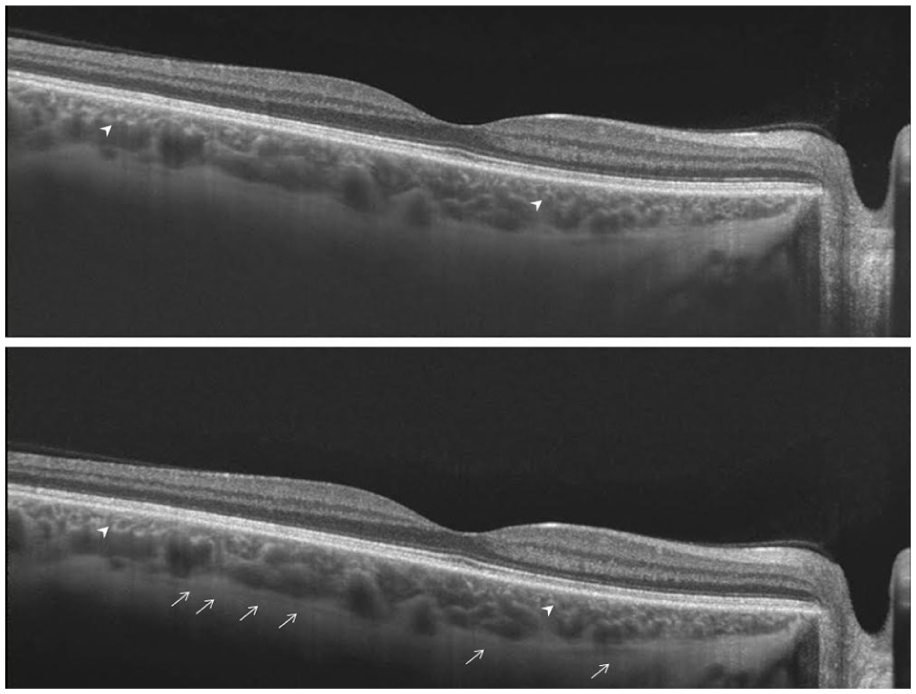
Improving choroidal imaging and capturing the suprachoroidal space with EDI. Comparison of visibility and contrast of the vascular structures in the choriocapillaris (arrowheads) suggests an advantage for EDI SS-OCT (bottom). Deeper choroidal structures also appear with a greater precision in the EDI image. The suprachoroidal space, hardly detected with conventional imaging, can be followed on most of the B-Scan when EDI is used (arrows).
According to recent publications, averaged pictures obtained by SS-OCT seem to be more precise in detecting the choroid-scleral interface than by SD-EDI-OCT.8,9,11–16 Nonetheless, there are some trade-offs with SS-OCT. 17 Although tissue penetration is greater with longer light wavelengths, melanin-containing tissues in particular, vitreous humor absorbs longer wavelengths of light due to its high water content. This discrepancy causes attenuation of the long light wavelengths that are intended to demonstrate the deep layers of the retina and choroid, practically reducing the actual usable bandwidth of the light source. 1
Our results indicate that, by applying the EDI technique to SS-OCT, we can circumvent those trade-offs, enhancing resolution and contrast of the deepest ocular structures. The light source has a finite bandwidth; for deeper object’s layers, the successive reflected wavelengths are modulated with higher modulation frequencies. As the modulation values between successive reflected wavelengths decreases, 18 it affects the resolution of deeper object’s layers, thereby limiting the deepest layer that can be properly seen. In SS-OCT, like in SD-OCT, when purposefully shifting the device closer to the deeper layers, so that the deep choroid layers are located closer to the zero optical path difference relative to the reference mirror, we enhance the sensitivity of those structures and increase their resolution.
To our knowledge, our study is the first head-to-head comparison of EDI-SS-OCT and SS-OCT for averaged pictures at the fovea in healthy eyes. 20 Our method may be further extended with the use of EDI-SS-OCT to three-dimensional (3D) volumetric scanning. Visualization of the sclera was also improved with EDI SS-OCT (Figure 2). The fine details of the sclera are poorly captured by existing technologies including ultrasonography and SD-OCT. SS-OCT has already increased visualization of the sclera. EDI-SS-OCT could further improve our understanding of the sclera in health and disease.12,19,21 We expect that enhanced imaging techniques will assist with the diagnosis and treatment of diseases of the outer retinal layers, and beyond.15,22,23
Limitations of our study include subjective assessment of the pictures, the modest number of patients, and the use of a single brand of SS-OCT, as several are commercially available. However, data from this study seem to be sufficiently clear cut to promote further research in this direction.
Although currently it may not represent an obvious advantage in daily practice, improvement of choroidal resolution on OCT is of undeniable interest for research, as there is a growing interest in previously poorly explorable ocular structures. For instance, the suprachoroidal space is gaining attention.24–33 EDI-SS-OCT could be a tool of choice for studying this structure in health and disease or for documenting the effect of novel therapies delivered via this way. It could also complement ultrasound in studying scleral diseases.
In conclusion, the EDI technique applied to SS-OCT enhances visualization of the choroidal details, of the choroidoscleral junction, and of the sclera. This modality could improve our understanding of normality as well as disease and response to therapy in conditions involving the choroid or the sclera.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.