
Abstract
Dysfunction of the third cranial nerve can be provoked by a number of different conditions. An isolated cranial neuropathy as a first clinical sign of a non-Hodgkin lymphoma is very infrequent. We represent here an atypical case of lymphoblastic lymphoma revealed by an isolated third cranial nerve palsy. The patient was managed by alternating cycles of cyclophosphamide, vincristine, and prednisone. She made a full recovery with a complete resolution of the symptomatology.
Introduction
Third cranial nerve palsy may be caused by lesions located anywhere along its path between the mesencephalon and the orbit. 1 It can be provoked by various diseases, and the differential diagnosis should consider many factors such as patient’s medical history, his age, and the clinical presentation. Lymphoma is not a common diagnosis of oculomotor dysfunction. It can be the result of direct invasion of the nerve, infiltration of the cavernous sinus, or dissemination to the surrounding leptomeninges. 1 , 2 We describe the case of a female patient who presented with an isolated oculomotor nerve palsy as an initial and uncommon manifestation of lymphoblastic lymphoma.
Case report
A 30-year-old Tunisian female, with no medical history, was admitted to the Department of Internal Medicine for acute right ptosis and diplopia, associated with fatigue and weight loss. The patient reported also a secondary amenorrhea for 3 months. Vital signs were within normal limits except for a heart rate of 110 beats per minute. The conjunctivae were pale and mucous membranes were dry. The abdominal examination revealed a defenseless abdomen with a diffuse distension. The ocular examination revealed a unilateral major ptosis of the right eye (Figure 1). The motility exam showed right ophthalmoplegia due to paralysis of the third nerve with limitation of adduction, elevation, and depression (Figure 2). The patient’s best corrected visual acuity (BCVA) was 20/20 in the left eye and 20/25 in the right eye. Both eyes had a normal pupillary reflex. Fundus examination found bilateral hemorrhagic sites with cotton wool spots (CWSs; Figure 3). Fluorescein angiography and spectral domain optical coherence tomography identified no abnormalities in both eyes. Cerebral magnetic resonance imaging (MRI) revealed a voluminous long-axis sellar process (21 mm) invading the sinus cavernous in isosignal intensity on T1-weighted imaging with heterogeneous enhancement after gadolinium injection. Laboratory results showed a normocytic anemia with a hemoglobin level of 5.5 g/dL, white blood cell count at 6320 E/mm3, and platelet count at 105,000 E/mm3. The serum protein electrophoresis revealed a polyclonal peak (g/dL) in the β-region. The bone marrow examination showed a cellular marrow with reduced megakaryopoiesis and myelopoiesis. The abdominal computed tomography (CT) showed pancreatic, ganglionic, and bone infiltrative involvement with paravertebral thickening at the level of D8–D9. The diagnosis of lymphoblastic lymphoma B was established by a peritoneal biopsy. The patient received cures of chemotherapy using cyclophosphamide, vincristine, and prednisone. It was an effective treatment for the patient and all her symptoms resolved within 2 months. The ptosis of the right eye has totally disappeared. Cerebral MRI was normal.

The examination showing severe ptosis of the right eyelid and exotropia of the primary look of the right eye.

Motility exam showing right ophthalmoplegia secondary to third nerve palsy. The central image represents forward gaze, and each image around it represents gaze in that direction. The exam revealed defective adduction, elevation, and depression. The abduction was normal.
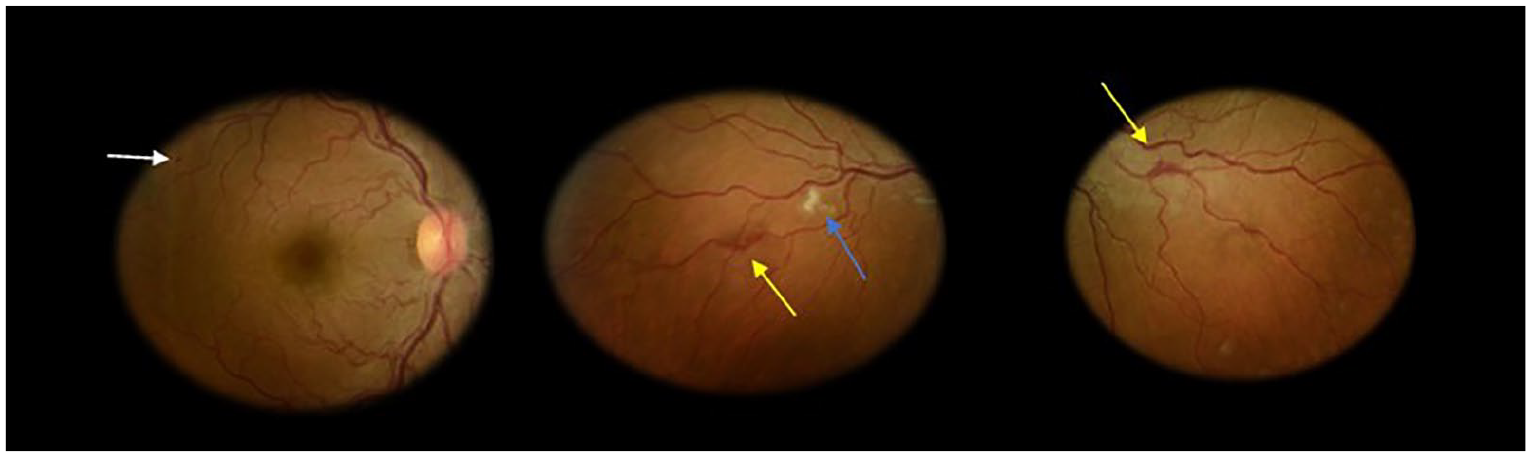
Fundus examination found microaneurysms in the right eye (white arrow) associated with blot hemorrhages (yellow arrows) and cotton wool spots (blue arrows) in both eyes.
Discussion
Although lymphomas affect mainly lymphoid tissue, they may involve extranodal organs, of which gastrointestinal tract is the most common one. Cranial nerves and cavernous sinus are often involved in lymphomas. Nevertheless, unilateral isolated oculomotor palsy as the first presenting manifestation of a lymphoma is very uncommon. 3 , 4 The most cranial nerve affected by this condition is the facial nerve. In our case, isolated third cranial nerve palsy was the first manifestation of lymphoma, and it was also a part of a systemic dissemination with physical examination abnormalities and laboratory results that guided us toward a valid diagnostic conclusion. In fact, hypergammaglobulinemia, observed in our case, is the most frequent cause of hyperviscosity syndrome and is commonly associated with lymphoplasmacytic lymphoma. This subtype of lymphoma may present with uncommon and devastating symptoms. The weakness, headache, dizziness, bleeding, and visual disturbance which have been described in these patients are due to hyperviscosity. 4 , 5
After thorough review of the English-language published literature, we found detailed case reports of 19 patients presenting central nervous system (CNS) lymphoma who had isolated oculomotor dysfunction (Table 1). The cell types were specified in all cases: seven had large B-cell lymphoma and four had Burkitt lymphoma. There was a single patient affected by each of the following conditions: Hodgkin lymphoma and a natural killer cell lymphoma. 5 – 23
Case reports of patients manifesting isolated oculomotor nerve palsy due to lymphoma.
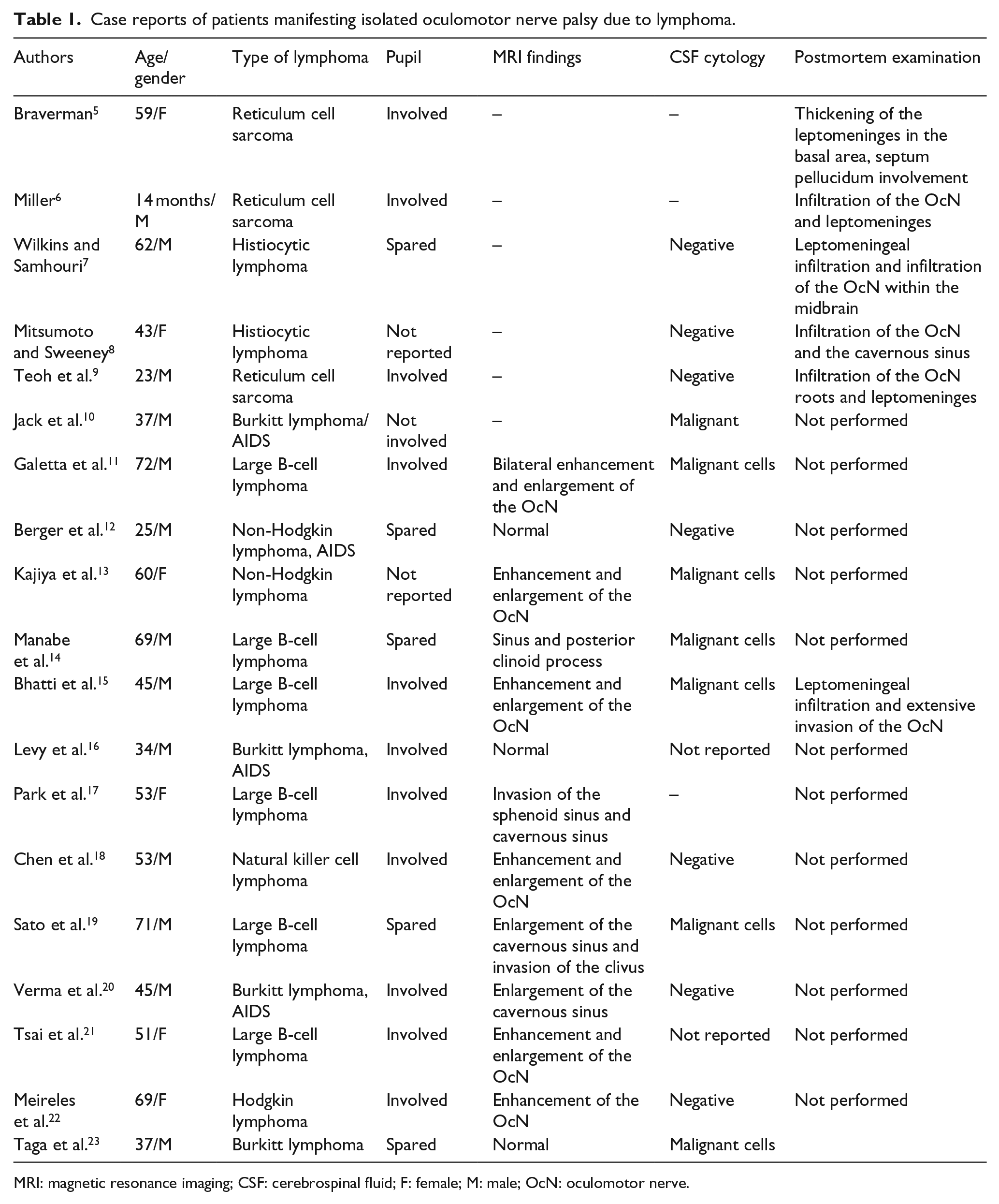
MRI: magnetic resonance imaging; CSF: cerebrospinal fluid; F: female; M: male; OcN: oculomotor nerve.
In most of the cases, lesions causing oculomotor nerve palsy were the infiltration of the cavernous sinus and the enclosing of the leptomeninges with or without oculomotor nerve invasion. Diagnosing these previous lesions on MRI or fluorodeoxyglucose-positron emission tomography (FDG-PET) was not always successful. In old reported cases in the literature, the diagnosis was made by postmortem examination. Only one case report 15 correlated the MRI findings with the histopathologic finding. Even though the histology of the lesions detected on MRI in the cavernous sinus was not confirmed directly in our case, the pathogenic relevance of lymphoma in oculomotor nerve palsy was strongly suspected by MRI findings and the clinical history and biopsy in another site. The sensitivity of brain MRI in the diagnosis of leptomeningeal disease had been studied in a few researches. T1-weighted imaging is the most sensitive technique, with a reported sensitivity within 60%. 24 MRI abnormalities consistent with leptomeningeal involvement include leptomeningeal, subependymal, dural, or cranial nerve enhancement, superficial cerebral lesions, and communicating hydrocephalus. 24
Patients with cavernous sinus syndrome often report a history of headache, diplopia, ophthalmoplegia, ptosis, and facial insensibility. Clinical features may differ depending on the extent of invasion of cavernous sinus. In our case, in the fundus examination, we have found bilateral hemorrhage sites and CWSs. These lesions represent signs of serious vascular damage. In fact, CWSs on the fundoscopic examination represent retinal nerve fiber layer infarcts, a sign of retinal hypoperfusion, which necessitates performing fluorescein angiography. They occur after arteriolar obstruction in the limits of large ischemic zones. Microaneurysms can be observed at the edge of some CWSs in different conditions with retinal ischemia. Cho and Yoon 25 reported a case of systemic non-Hodgkin lymphoma in a 63-year-old man presenting with CWSs.
In conclusion, this case report emphasizes the importance of recognizing isolated third cranial nerve palsy as a first clinical manifestation of lymphoma. Prompt treatment of this chemosensitive disease can lead to complete remission of the symptomatology with good results. Since a diagnosis of lymphoma was made based on peritoneal biopsy, our patient was able to start systemic chemotherapy and exhibited a good response.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed written consent was obtained from the patient.