
Abstract
Objective:
To describe the retinal imaging characteristics, retinopathy management strategies and visual outcomes in cases of diabetes with chronic myeloid leukaemia.
Design:
Retrospective observational study.
Participants:
Patients with diabetes and chronic myeloid leukaemia managed at our tertiary eye care centre from January 2015 to December 2017.
Methods:
Detailed ophthalmic and systemic evaluation, treatment and follow-up records were reviewed. The main measures studied were visual acuity, intra-ocular pressure, retinopathy severity, and surgical indications and techniques.
Results:
Of the six patients studied, three had diabetes and chronic myeloid leukaemia at presentation, while in three cases chronic myeloid leukaemia was diagnosed following evaluation for proliferative retinopathy. The visual acuity ranged from 20/20 to perception of light. All eyes had marked proliferative retinopathy out of proportion to the exudation. None of the eyes had significant macular oedema. Pan-retinal photocoagulation (10/12, 83.33%), intravitreal anti-vascular endothelial growth factor injection (8/12, 66.67%), vitrectomy (2/12, 16.67%), cataract surgery (2/12, 16.67%) and trabeculectomy followed by cryoablation (2/12, 16.67%) was performed for management of the ocular disease as indicated. Median follow-up was 16.5 months (range: 6–24 months). Final visual acuity ranged from PL to 20/20 with acuity ⩾ 20/100 in eight eyes. Four eyes had advanced optic neuropathy from neovascular glaucoma.
Conclusion:
Accelerated proliferative retinopathy can be seen in cases of diabetes with chronic myeloid leukaemia at the very initial ophthalmic evaluation. Thus, there is a need to alter screening guidelines for retinopathy in cases of diabetes with chronic myeloid leukaemia. Early detection and aggressive management may help preserve visual acuity in such cases.
Introduction
The prevalence of diabetes is rapidly increasing in the world. According to the World Health Organization data, there were an estimated 422 million adults affected with diabetes in 2014. 1 The prevalence of diabetes was estimated at 8.5% in the adult population. 1 The prevalence of chronic myeloid leukaemia (CML) has also risen markedly over the years. It is estimated to range from 18 to 200/100,000 population in various studies. 2 , 3 The survival of patients of CML has improved significantly following the introduction of tyrosine kinase inhibitor therapy. 2 Thus, in the current scenario, oncologists, endocrinologists and ophthalmologists will be encountering more and more patients with a combination of diabetes and CML (active or in remission).
Micro-angiopathy is common to both diabetes and CML. While in diabetes, this occurs due to basement membrane thickening, pericyte loss, and endothelial cell dysfunction; 4 in CML, the underlying cause is hyperviscosity and toxin-mediated endothelial injury. 5 With coexistent diabetes and CML, the occlusive angiopathy is expected to be worse with consequently greater tissue hypoxia. The retinopathy in such cases may not follow the natural course and may be more aggressive to treat. There is paucity of literature with regard to retinopathy in coexistent diabetes and CML.6–8
In this article, we describe our experience of managing the retinal manifestations seen in patients of CML with diabetic retinopathy (DR) and also review the existing literature on the same.
Materials and methods
A record review of patients with Diabetes and CML who presented with a visual decline to a tertiary eye care centre for 3 years (from January 2015 to December 2017) was performed. The research was performed in accordance with the tenets of the declaration of Helsinki and the institutional research guidelines. A formal Ethics committee approval was obtained for the study.
Demographic details, detailed history and ocular as well as systemic treatment records were reviewed. The key information looked for in history was the duration of diabetes, duration of CML, the phase of CML and treatment undertaken for CML at the time of initial presentation and subsequent management of proliferative retinopathy.
The ocular examination details included visual assessment (Snellen chart), intra-ocular pressure (IOP), slit lamp assessment for neovascularization of iris or angle (NVI/NVA), and dilated fundus evaluation for the stage of DR and macular thickness/oedema. Colour fundus imaging, fundus fluorescein angiography (FFA) and macular optical coherence tomography (OCT) details were reviewed, wherever performed. A note was made of the central macular thickness and presence of macular oedema on the OCT scans.
Ocular treatment details included the need for pan-retinal photocoagulation (PRP), intravitreal anti-vascular endothelial growth factor (VEGF) injection, vitrectomy, and management of neovascular glaucoma (NVG), wherever present, with filtration surgery/trabeculectomy and/or cryoablation. The final follow-up visual outcome, IOP and retinal status were noted.
The data was entered into an Excel sheet and analysed using STATA SE 12·1 software. For descriptive purposes, non-parametric data were expressed as median (range), parametric qualitative data as a percentage and quantitative data as the mean ± standard deviation (SD).
Results
Six patients with diabetes and CML were evaluated in this study. The mean age was 55·2 ± 8·9 years. Five patients were male, and one was female. The disease characteristics of these patients are provided in Table 1.
Characteristics of patients with diabetic retinopathy and chronic myeloid leukaemia.
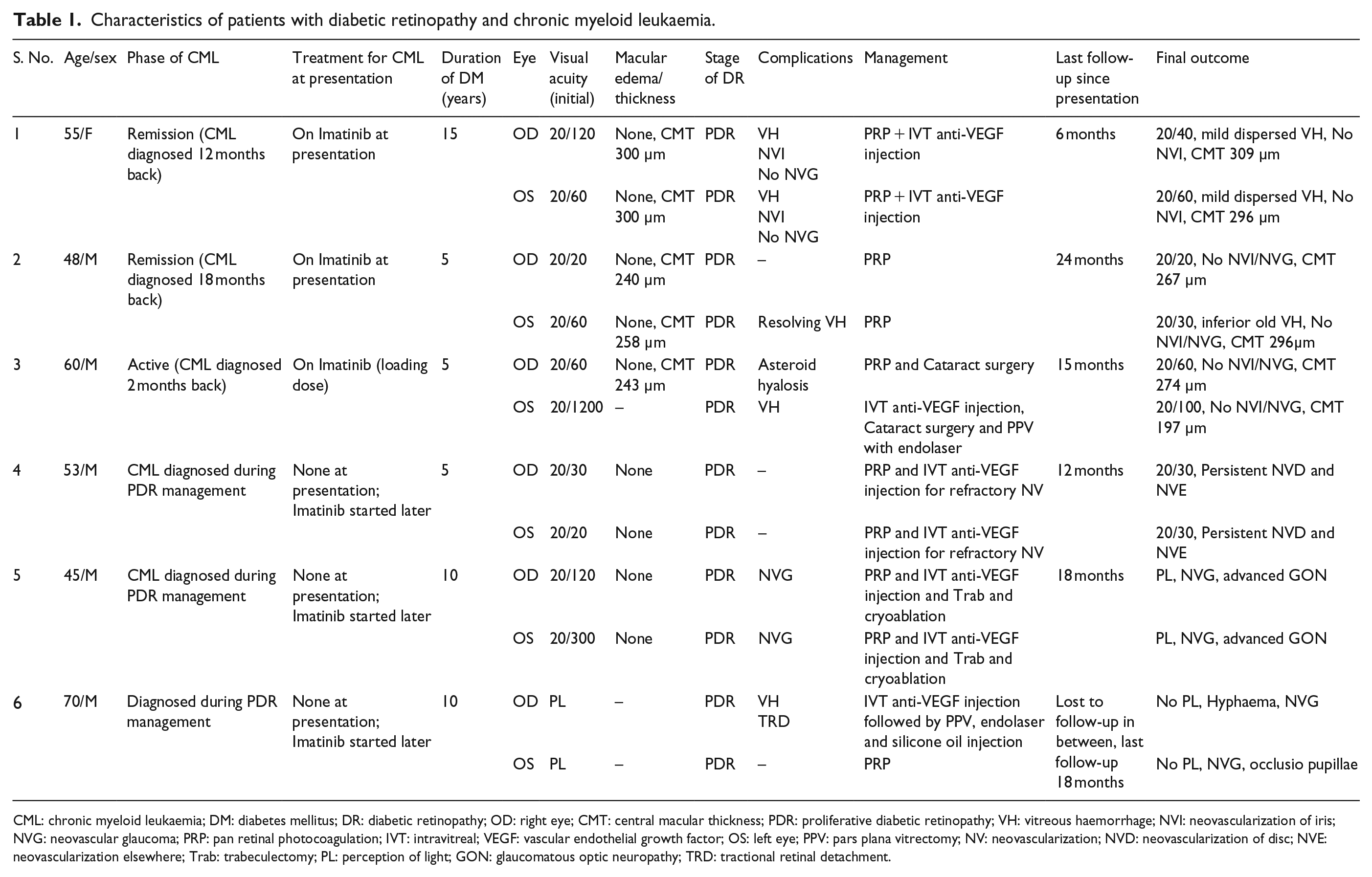
CML: chronic myeloid leukaemia; DM: diabetes mellitus; DR: diabetic retinopathy; OD: right eye; CMT: central macular thickness; PDR: proliferative diabetic retinopathy; VH: vitreous haemorrhage; NVI: neovascularization of iris; NVG: neovascular glaucoma; PRP: pan retinal photocoagulation; IVT: intravitreal; VEGF: vascular endothelial growth factor; OS: left eye; PPV: pars plana vitrectomy; NV: neovascularization; NVD: neovascularization of disc; NVE: neovascularization elsewhere; Trab: trabeculectomy; PL: perception of light; GON: glaucomatous optic neuropathy; TRD: tractional retinal detachment.
All patients had type 2 diabetes mellitus. The median duration of diabetes was 7·5 years (range 5–15 years). None of the patients had received any ocular treatment for DR before presentation at our centre. The corrected distance visual acuity (CDVA) at presentation ranged from a perception of light (PL) to 20/20. CDVA < 20/60 was noted in six eyes. All eyes had proliferative retinopathy changes with neovascularization out of proportion to exudation (Figure 1). FFA revealed extensive capillary non-perfusion (CNP) areas in all the cases (Figure 1). Neovascularization of the disc (NVD) and neovascularization elsewhere (NVE) was also noted consequent to the marked ischaemia (Figures 2 and 3). The fundus images and angiograms also reveal the extent of non-perfusion and proliferation to be out of proportion to the exudates and microaneurysms (Figure 3). None of the eyes had significant macular oedema on OCT. The complications arising secondary to proliferative retinopathy were vitreous haemorrhage (VH; n = 5 eyes), NVI (n = 4 eyes) and NVG (n = 2 eyes).
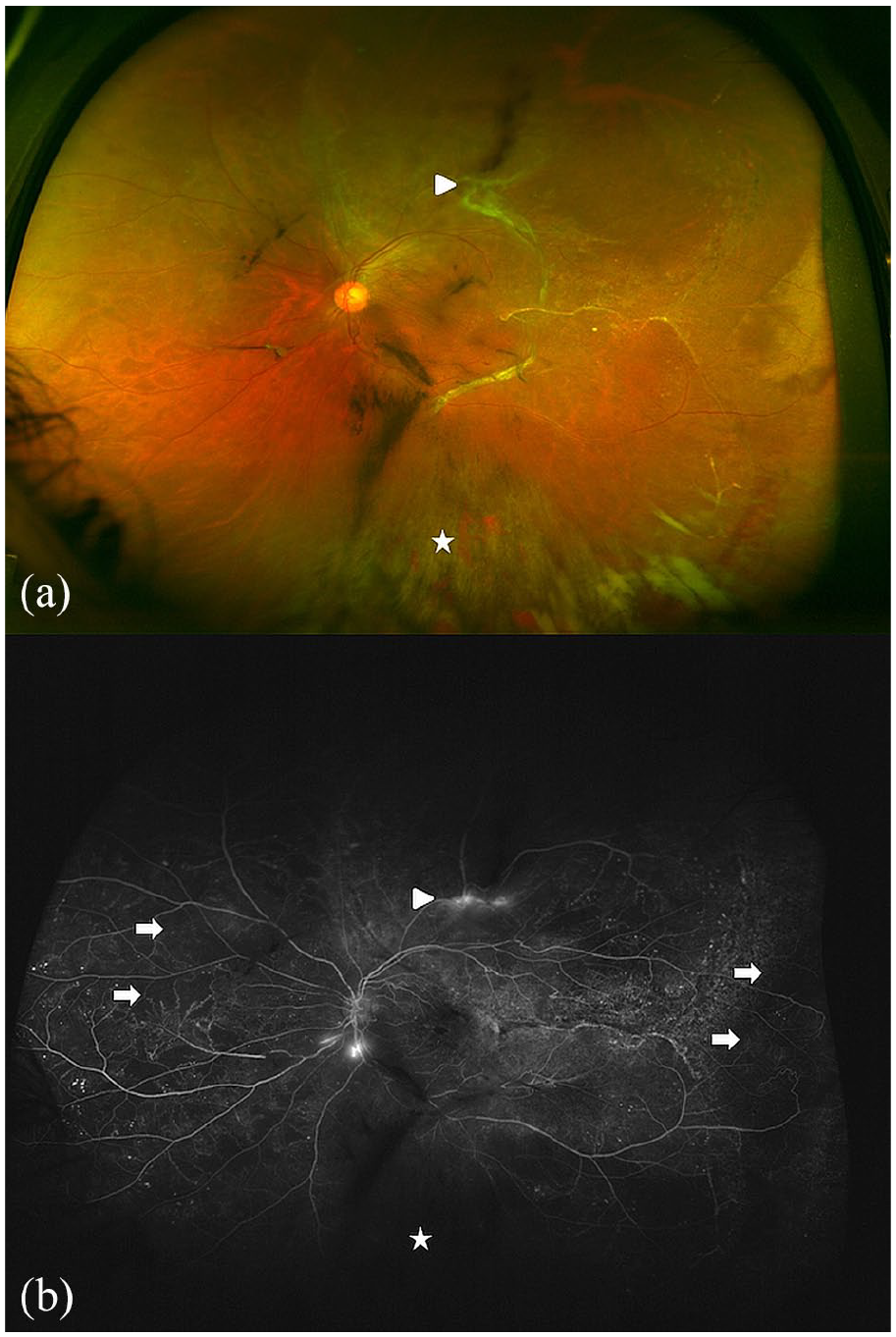
Ultra-wide-field fundus imaging of left eye of a 48-year-old male patient with type 2 diabetes mellitus and chronic myeloid leukaemia in remission on Imatinib therapy (case 2). (a) Pseudo-colour image shows fibro-vascular proliferation (white arrowhead) along the supero-temporal arcade, inferior vitreous haemorrhage (white star) and absence of macular exudation. (b). Fundus fluorescein angiography shows leakage along the supero-temporal arcade (white arrowhead) and at the disc suggestive of neovascularization, extensive peripheral capillary non-perfusion (white arrows), and blocked fluorescence inferiorly from vitreous haemorrhage (white star) and absence of leakage at the macula.
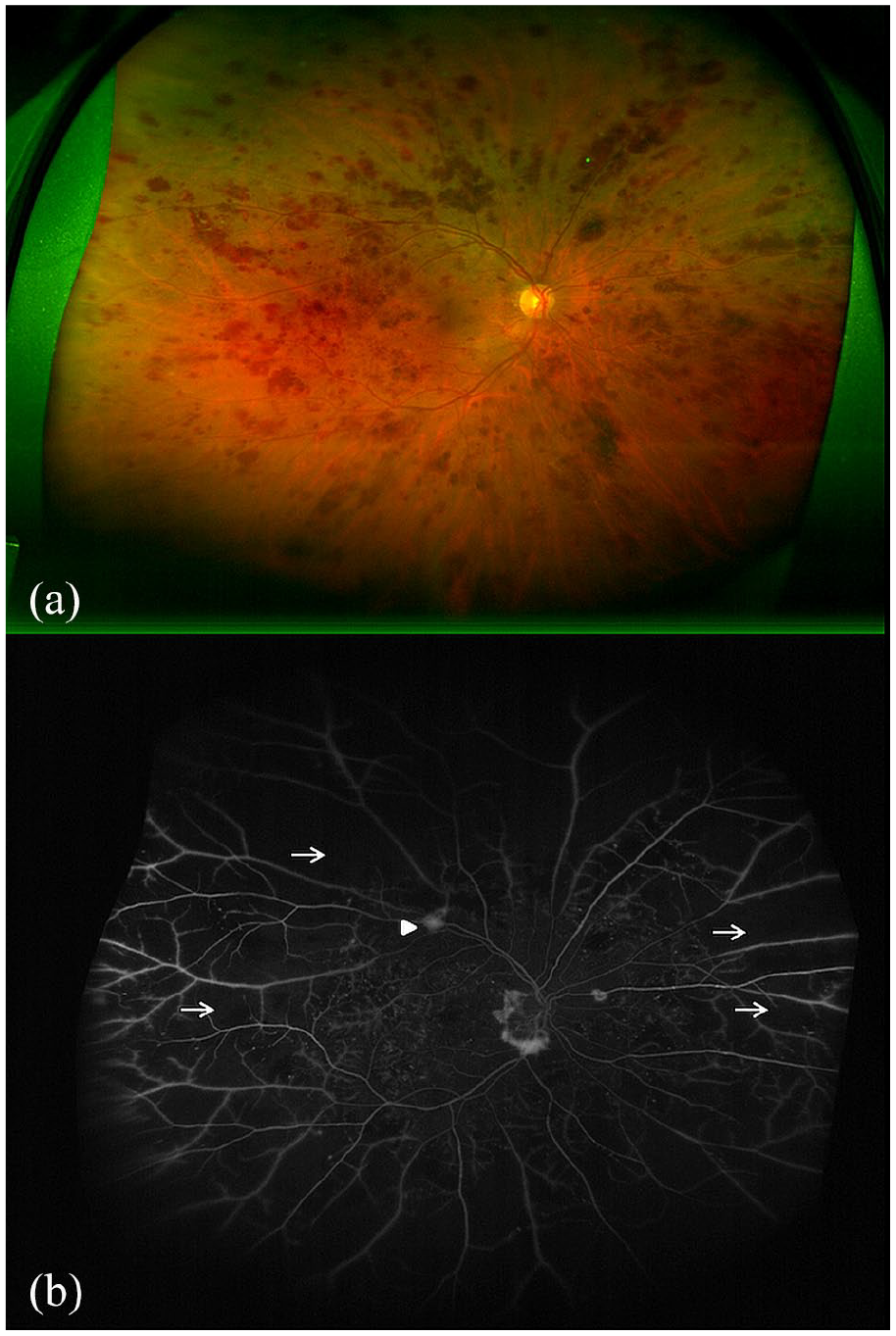
Ultra-wide-field fundus imaging of right eye of a 60-year-old male patient with type 2 diabetes mellitus and recently diagnosed chronic myeloid leukaemia (case 3). (a) Pseudo-colour image shows widespread dot-blot retinal haemorrhages and absence of macular exudation. (b) Fundus fluorescein angiography shows leakage along the supero-temporal arcade (white arrowhead) and at the disc suggestive of neovascularization, extensive capillary non-perfusion (white arrows) and absence of leakage at the macula.
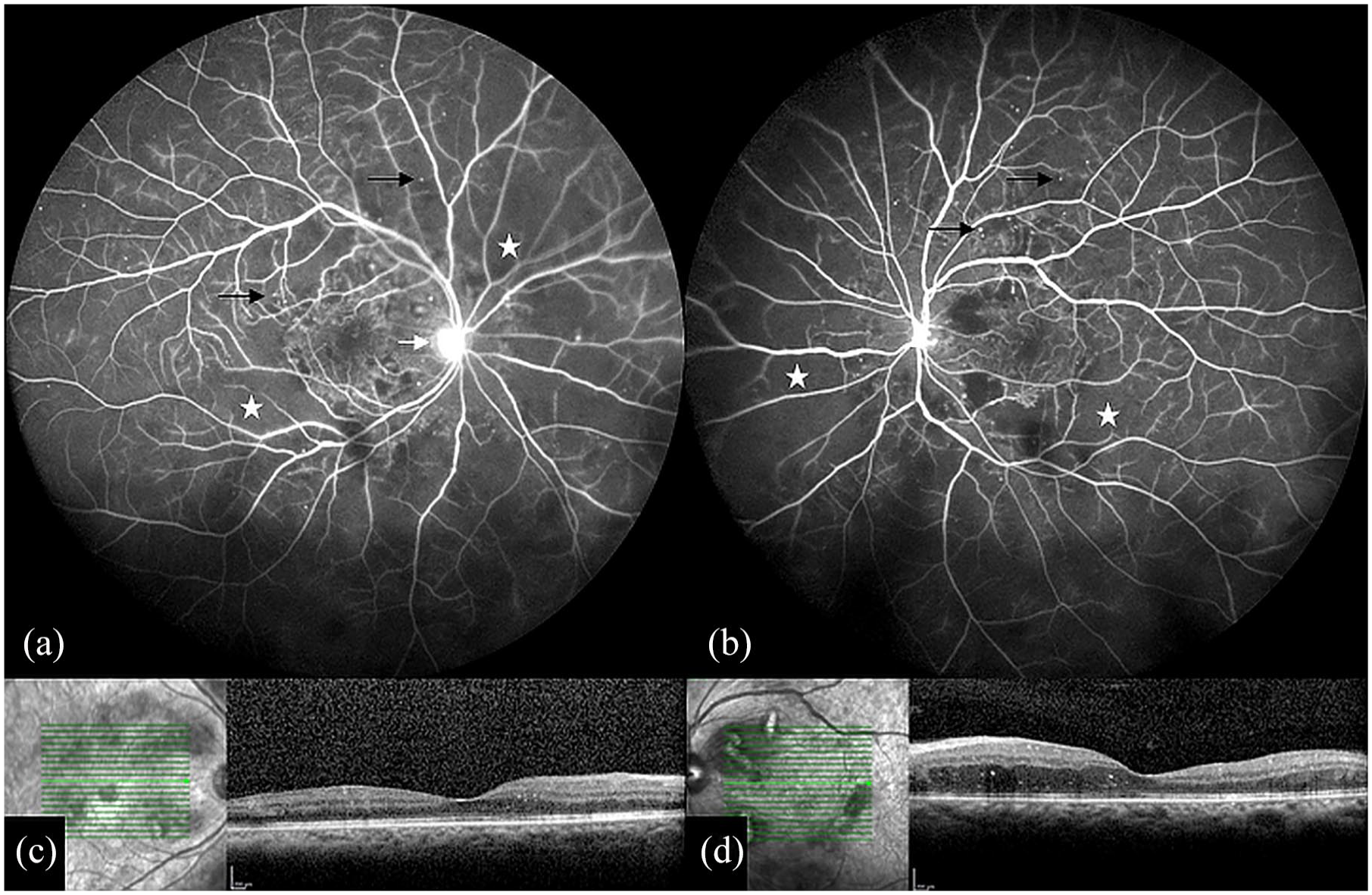
Fundus imaging of a 53-year-old male patient with type 2 diabetes mellitus (case 4). (a) and (b) Wide-field fluorescein angiography shows extensive capillary non-perfusion (white star) and relatively few microaneurysms (black arrows) in both the eyes. Leakage from the neovascularization at the disc is seen in the right eye (white arrow). (c) and (d) The corresponding optical coherence tomography scans of the macular area shows an absence of cystoid or spongiform oedema in both the eyes. This patient was diagnosed as having chronic myeloid leukaemia following detection of proliferative retinopathy.
CML was diagnosed before presentation to us in three patients (2–18 months back). Two of these were in haematological remission on imatinib mesylate therapy, and one had an active phase of CML. In the rest, it was diagnosed during the course of treatment for DR and follow-up. These three patients did not have systemic complaints suggestive of leukaemia at the time of presentation. On routine follow-up, in these patients, an abnormally raised total leucocyte count raised suspicion, and therefore, they were referred to the hemato-oncologist for evaluation. All patients received Imatinib mesylate therapy under the supervision of the treating hemato-oncologist.
The proliferative retinopathy was managed with PRP alone (n = 4 eyes) or combination (either simultaneous or sequential) of PRP and intravitreal anti-VEGF injection (n = 6 eyes) or vitrectomy with endolaser (n = 2 eyes). Before vitrectomy, an intravitreal anti-VEGF injection was given as an adjunct. In addition, both eyes of case 5 required filtration surgery in the form of trabeculectomy. In view of refractory glaucoma, cyclo-cryotherapy was later performed in both eyes of this patient.
The median follow-up was 16.5 months (range 6–24 months). The final CDVA ranged from PL to 20/20. Final CDVA ⩾ 20/100 was achieved in eight eyes. The reason for poor vision in the rest of the four eyes was advanced optic neuropathy from NVG. Persistent NVD/NVE was noted in two eyes. None of the eyes developed significant macular oedema during the course of follow-up. One patient was lost to follow-up during the course and returned a year later with end-stage NVG in both eyes (case 6).
Discussion
Diabetes causes microangiopathy leading to changes in the retinal vasculature which evolve from mild non-proliferative retinopathy to severe proliferative retinopathy predominantly over the posterior pole with or without macular oedema. 9 These changes are a consequence of capillary endothelial dysfunction which leads to the development of CNP areas. 4 The retinal ischaemia up-regulates the VEGF pathway and subsequently causes aberrant neovascularization and its complications. 9 , 10 Along with these, a break-down of the blood-retinal barrier with leakage into the retina and the inflammatory cascade also play a role in the etiopathogenesis of the entire spectrum of DR. 11
Leukaemic retinopathy is a common ocular manifestation and presenting feature of systemic leukaemias. 5 , 12 The factors responsible include hyperviscosity due to increased blood counts, endothelial damage by toxins released from tumour cells, anaemia and thrombocytopenia. 5 , 13 Acute leukaemias present with features of anaemia and thrombocytopenia in the form of retinal and preretinal haemorrhages, Roth spots, hard exudates and cotton wool spots. Chronic leukaemias present with features of venous stasis and peripheral retinal ischaemia. Proliferative retinopathy, comprising of mid-peripheral sea-fan fibro-vascular proliferation and its sequelae like tractional retinal detachment and VH may occur secondary to peripheral ischaemia, particularly in CML.14–22 However, a majority of such cases of proliferative retinopathy in CML are diagnosed with the haematological malignancy during the course of ocular treatment. 15 , 16 , 18 , 20 , 21 In addition, certain chemotherapy drugs such as Arabinoside-C may also aggravate the vasculopathy leading to much severe ischaemia in leukaemias. 23
The microvascular complications are expected to worsen in the presence of both diabetes and CML. A combination of diabetes and CML can be expected to have a rapid progression of retinal vasoproliferative changes which are a consequence of extensive CNP and tissue hypoxia. Only a few case reports exist on proliferative retinopathy in patients with diabetes and CML.6–8, 16 A summary of cases of proliferative retinopathy in patients of CML with or without diabetes is provided in Table 2. Schmid et al. 7 have reported a case of transient severe non-proliferative DR in an adolescent with type 1 diabetes and CML, which regressed later with the treatment of CML alone. Raynor et al. 6 and Figueiredo et al. 8 reported cases of type 2 diabetes with sudden worsening of DR to proliferative stages, which was consistent with the development of CML in these cases. The factors which may contribute to the development and rapid worsening of DR include enhanced endothelial dysfunction, vascular stasis, and retinal ischaemia due to associated anaemia. 8 , 24 In addition, the serum VEGF levels are also up-regulated in patients with CML alone. 25
Review of literature on proliferative retinopathy in patients with chronic myeloid leukaemia.

CML: chronic myeloid leukaemia; DM: diabetes mellitus; DR: diabetic retinopathy; OD: right eye; OS: left eye; HMCF: hand movements close to face; PR: proliferative retinopathy; FVP: fibrovascular proliferation; VH: vitreous haemorrhage; PRP: pan retinal photocoagulation; PPV: pars plana vitrectomy; TRD: tractional retinal detachment; NVD: neovascularization of disc; NPDR: non proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy; DME: diabetic macular edema; NVG: neovascular glaucoma; OU: both eyes; NV: neovascularization; IVT: intravitreal; NVI: neovascularization of iris; Trab: trabeculectomy; TRP: Targeted retinal photocoagulation; SHH: Sub hyaloid haemorrhage.
Retinopathy in such cases is typically refractory to ocular treatment alone (PRP) and needs treatment of the underlying systemic disease also, that is, chemotherapy.6–8 In our series, three patients who had CML at presentation and were on chemotherapy showed complete regression of the proliferative retinopathy with PRP/anti-VEGF treatment. Imatinib is known to have a direct effect on endothelial cells and downregulates VEGF production. 26 This may be an additional benefit of Imatinib therapy. However, the patients who developed CML later had worse diabetic proliferation and persistent neovascularization despite ocular and systemic therapy.
Reviewing the existing literature and our data, we feel that the following points need consideration. A subset of patients presenting to an ophthalmologist would already be known to have diabetes and CML. These need to be screened much earlier and followed up at shorter intervals than the standard recommendations for DR. 27 , 28 Early detection of proliferative changes will help both the ophthalmologist and oncologist to take better tertiary preventive measures. Better hemodynamic control and prophylactic laser photocoagulation may prevent advanced proliferative disease in specific high-risk scenarios such as extensive CNP.
A subset of patients may be known diabetics but also have underlying undiagnosed CML. Presence of unexpectedly more areas of CNP on fluorescein angiography, with early neovascularization in the absence of other characteristic changes of DR like prominent microaneurysms and hard exudates, should alert the ophthalmologist to get a hemogram with peripheral smear done. This may reveal the underlying haematological disorder.
Despite the proliferative retinopathy, these patients initially seem to have a healthy macula. Fluorescein angiograms of these patients revealed a relative lack of microaneurysms and associated hard exudates/retinal oedema. However, these patients lose vision later due to an early progression of the neovascular retinopathy leading to VH and NVG.
Proliferative retinopathy developing in cases of diabetes and CML needs to be aggressively managed. Along with systemic treatment, a combination of PRP, anti-VEGF agents and vitrectomy as and when required can help maintain vision in most cases. Early vitrectomy may be needed if traction sets in, threatening or involving the macula or if VH occurs.
Few questions remain unanswered and our beyond the scope of our series. First, despite remission, why do cases of CML with diabetes develop rapidly progressing proliferative retinopathy? It might be that the acute endothelial insult at the time of active CML initiates a cascade of events eventually leading to proliferative retinopathy despite the CML going into remission. Diabetes may enhance this process markedly. However, this is just a hypothesis. Second, why does severe macular oedema not develop in such cases? We don’t have a definite answer to this. However, what appears from the angiograms is that CNP and ischaemia similar to venous stasis retinopathy is accelerated in such cases. Microaneurysmal changes and exudation, on the other hand, are slow to develop and thus macular oedema is not seen despite the patient presenting with complications of the proliferative retinopathy. A larger series and macular vessel density and perfusion analysis with OCT-angiography might help prove/disprove our observations.
Limitations of our study are that the conclusions are based on the retrospective review of only six cases and similar reports that we found from literature. However, we feel that based on these observations there is a need to formulate guidelines for ophthalmologists, endocrinologists and oncologists managing patients of diabetes with CML. The present study highlights the need to perform an ophthalmic examination early and more frequently in diabetic patients with CML. In addition, it stresses the importance of investigating and ruling out a haematological abnormality when unexpectedly large areas of peripheral retinal nonperfusion are observed, especially out of proportion to the other DR lesions in the fundus. Early diagnosis of proliferative DR and prompt and aggressive treatment are needed to preserve visual acuity in such patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.