
Abstract
Objective:
To outline the incidence of posterior segment injuries related to soccer-ball blunt trauma in children.
Methods:
Retrospective search of the computerized hospital medical database between the years 2007 and 2017. All pediatric trauma cases were reviewed and cases with blunt trauma related to direct orbital/ocular hit from a soccer-ball were included. Cases were divided into two groups (non-severe and severe) based on the presence of sight-threatening findings on presentation (e.g. retinal tear, vitreous hemorrhage, retinal detachment, and macular edema).
Results:
Out of 343 pediatric patients with relevant diagnoses, 14 (4.1%) were treated for injuries related to soccer-ball trauma. All patients were males at their early-to-mid teens (14.3 ± 2.1 years). The most common funduscopic finding was peripheral commotio retina (13, 93%). There was equal distribution between the two groups (seven each). Retinal injury in the severe group included retinal tear (3), vitreous hemorrhage (4), retinal detachment (1), and macular hole (1). Five patients in this group presented with visual acuity of 20/25 or better. Rate of external signs of injury were similar in both groups.
Conclusion:
Soccer-ball blunt trauma in children can cause significant posterior segment injuries regardless of the presence of external injury or ocular complaints. A thorough ocular exam is mandatory in all cases for the detection of vision-threatening retinal injuries.
Keywords
Introduction
Sports-related trauma is a well-known cause of ocular injury and morbidity accounting for up to 40% of all eye injuries.1,2 Eye injury has been reported to occur in nearly every sport type, with the majority of cases occurring in ball-related sports such as basketball, soccer, tennis, or baseball. 3 In these sports, the injury is usually caused by blunt trauma from a heavy object (e.g. the ball) thrown at high velocity. The site and force of impact as well as the size, shape, and material of the blunt object determine the severity and location of the injury. 4 Soccer-ball ocular injuries were previously assumed to be less harmful due to the misconception that the large ball is blocked by the orbital rim and direct injury to the eye is minimized, with most of the impact transmitted to the bony orbit. However, lab experiments confirmed that soccer balls deform upon a significant impact, allowing a small “knuckle” of the ball to enter the orbit and impact the globe. 4 In such cases, soccer-ball-related injuries may result in severe damage including corneal abrasions, hyphema, traumatic retinal edema, retinal breaks and detachment, macular hole, and choroidal hemorrhages.
Soccer is one of the most popular sports in Israel and it is considered to be one of the major causes of sports-related injury in the country. 5 Previous reports described substantial retinal damage after soccer-ball-related blunt trauma in both children and adults.6,7 In theory, it is logical to assume that children would present with relatively mild injuries, due to weaker kick energy, however previous reports negate this assumption.6,7
In this study, we examined the incidence of soccer-ball-related retinal trauma among children in the last decade in a tertiary referral center in Israel.
Materials and methods
The study was approved by the institutional review committee of the Sheba Medical Center. It includes all cases of retinal trauma related to soccer-ball injury treated at the Goldschleger Eye Institute, Sheba Medical Center, Tel-Hashomer, Israel between January 2007 and December 2017. Cases were identified through search of the computerized hospitals medical database with International Statistical Classification of Diseases and Related Health Problems (9th revision; ICD-9) codes representing retinal diagnoses that might be associated with blunt trauma to the eye (e.g. blunt orbital trauma, perforation of globe, retinal tear, retinal detachment, retinal edema, and vitreous hemorrhage). All patients of age 18 years or younger at the time of presentation were reviewed. We included only cases with specific description of blunt orbital and ocular trauma from a soccer-ball. Demographic data (age and gender), general and ocular history, clinical findings at presentation and follow-up, treatment and procedures were collected and summarized. Subjects were divided into two groups based on severity of injury: group 1 (non-severe)—mild signs of retinal trauma with traumatic retinal edema involving up to one retinal quadrant; and group 2 (severe)—severe signs of retinal trauma, for example, atleast one of the following: vitreous hemorrhage, retinal tear, and/or retinal detachment, macular hole, traumatic retinal edema extending more than one quadrant. The various parameters at presentation and follow-up were compared between the two groups Wilcoxon signed-rank test and Pearson’s chi-square test for continuous and categorical variables, respectively. A p-value of less than 0.05 was considered statistically significant.
Results
The database search yielded 4306 potential subjects diagnosed with relevant ICD-9 codes during the study period, of which 343 were pediatric patients and 14 (4.1%) were treated for injuries related directly to soccer-ball injuries. A summary of the cases is presented in Table 1. All patients were males at their early-to-mid teens with the exception of one patient aged 9.5 years (median, 14.4; range, 9.5–16.7 years). Past medical and ocular history was insignificant except for mild–moderate myopia in four (29%) subjects. The right and left eyes were affected equally. Time from injury to presentation was several hours in the vast majority of cases with a range of up to 4 days from the incident. In all cases the globe was intact.
Study population characteristics.
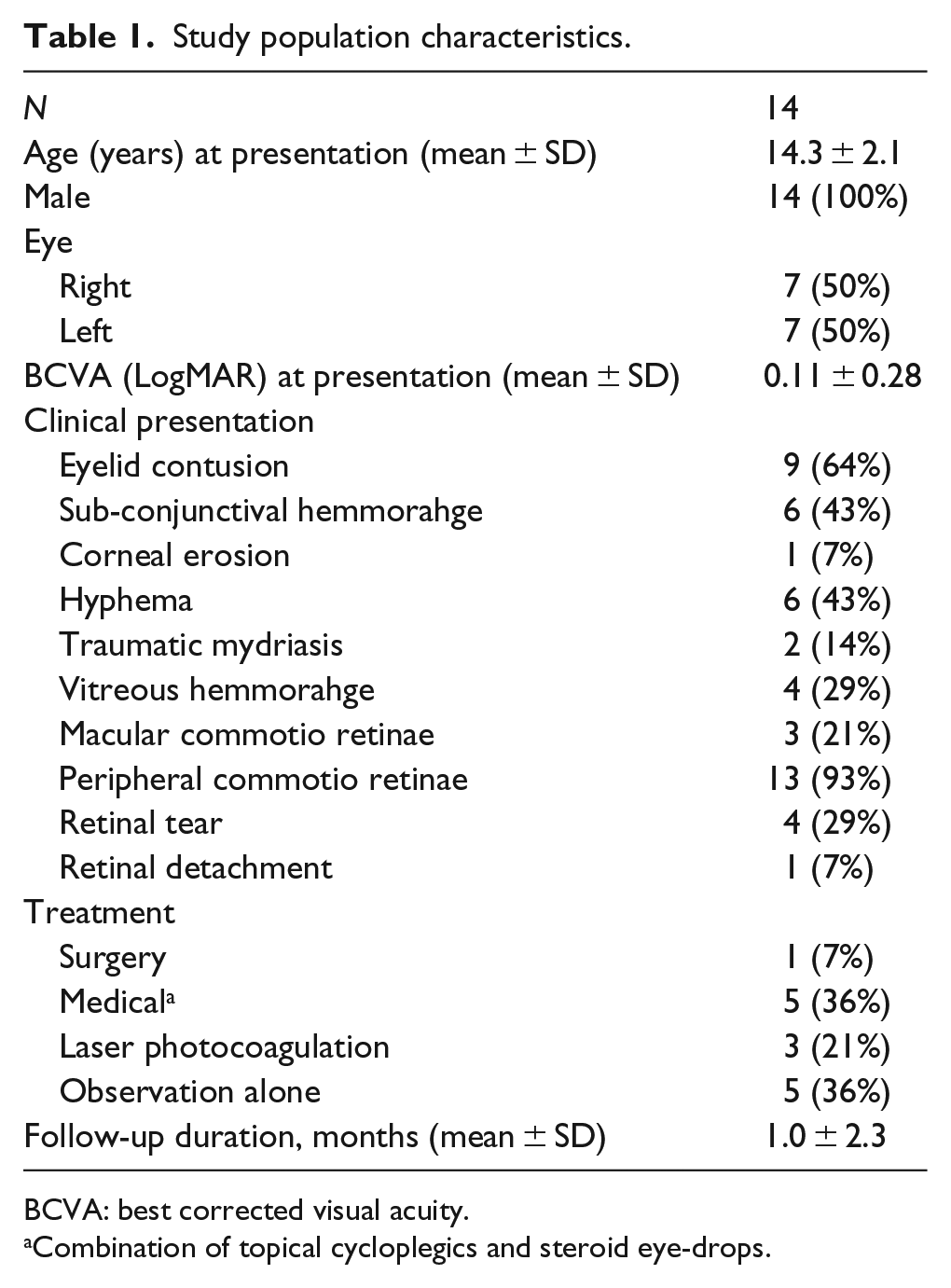
BCVA: best corrected visual acuity.
Combination of topical cycloplegics and steroid eye-drops.
A total of 11 patients (79%) presented with good best corrected visual acuity (BCVA) (20/25 or better). Three patients (21%) presented with decreased visual acuity (VA). Of these patients, one patient had central retinal edema with a macular hole and VA of 20/120. The macular hole closed spontaneously but VA did not improve. The second patient had mild vitreous hemorrhage, traumatic retinal edema, and a giant retinal tear and retinal detachment, and presented with BCVA of 20/200. He underwent retinal and cataract surgery, and the BCVA improved to 20/50 at the final follow-up. The third patient presented with VA of 20/200 due to moderate hypema, and improved to 20/20 with resolution of the hypema.
External ocular signs of injury (e.g. eyelid hematoma, sub-conjunctival hemorrhage, and corneal erosion) were documented in 11 eyes (79%). Hyphema was observed in six eyes (43%), two of which also presented with traumatic mydriasis. Treatment for hyphema included a combination of topical steroids and cycloplegics drops.
All eyes but one presented with peripheral traumatic retinal edema (13 eyes, 93% of cases) that was observed mostly in the superior-temporal quadrant (9 eyes, 70% of commotion retina cases). There was a marked variation in other retinal findings among subjects.
Group 1—non-severe (7 eyes, 50%): All eyes but one in this group presented with normal VA of 20/20, and all presented with mild signs of traumatic retinal edema involving up to one retinal quadrant with no additional funduscopic findings. One patient presented with VA of 20/200 due to anterior chamber hypema, traumatic mydriasis, and supero-temporal retinal edema. After the hypema resolved, VA improved to 20/20. No intervention was required in this group of eyes. Patients were shortly followed at our clinic, and were referred to the opthalmologists in their community, with instructions to return in case of any new symptoms.
Group 2—severe (7 eyes, 50%): All cases but one presented with retinal edema (one patient presented only with a retinal tear). Additional funduscopic finding in this group included: retinal tear (four eyes), macular edema (three eyes), vitreous hemorrhage (four eyes), retinal detachment (one eye), and macular hole (one eye). Five patients in this group presented with VA of 20/25 or better, and two patients presented with decreased VA, one with 20/120 and the second with 20/200.
In four eyes (29%), a retinal tear was detected at presentation. All tears where located at the superior or supero-temporal retina. Two out of four cases presenting with retinal tears in our series had no external ocular signs of injury. The retinal tear was treated promptly by laser photocoagulation in three eyes, with no further interventions. The fourth patient had retinal detachment at presentation with a superior giant retinal tear. He underwent posterior vitrectomy and silicon oil tamponade combined with scleral buckle (Figure 1(a)). Two months later, the oil was removed and an epiretinal membrane was removed, with internal limiting membrane (ILM) peeling. After 15 months, he underwent cataract surgery with implantation of intraocular lens. His BCVA improved from 20/200 at presentation to 20/50 at last follow-up (20 months). Mild central macular thickening (400 μm) was observed on optical coherence tomography (OCT) scan at the last visit (Figure 1(b)). Traumatic macular edema was detected in three subjects (21%). In accordance with current common practice for traumatic macular edema, no medical treatment was initiated although the patients were kept under close observation and one of whom subsequently developed a macular hole. The macular hole closed spontaneously during the follow-up period (Figure 2), however the VA did not improved and remained 20/120, due to the traumatic damage to the retina. This patient also developed increased intraocular pressure that was controlled with topical medications. Vitreous hemorrhage was observed in four eyes (one of which developed retinal detachment as previously described). The vitreous hemorrhage resolved spontaneously without any intervention in three eyes. One of these patients developed pigmentary retinal changes in the macula but VA was not affected and remained 20/20.
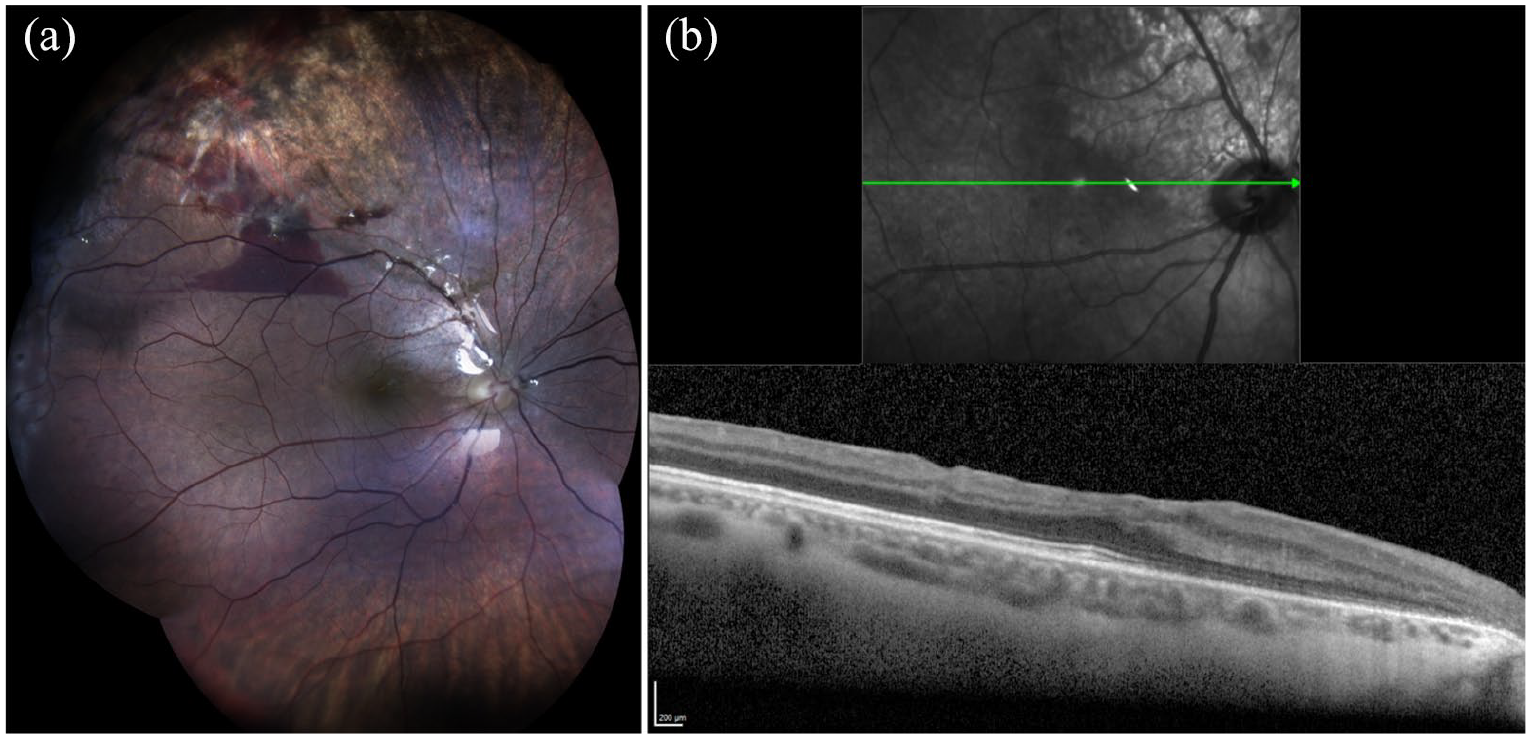
(a) Composite color fundus photography of a 14-year-old patient, 2 weeks post vitrectomy with silicone oil tamponade for traumatic giant retinal tear and detachment following a direct injury from a soccer-ball. Sub-retinal hemorrhage adjacent to the superior arcade is seen, as well as significant pigmentary changes in the supero-temporal region which correlates to the area of resolved traumatic retinal edema. Reflections from the retina are due to silicone tamponade. (b) The macular OCT scans taken 5 months post cataract surgery. The lack of the normal contour is apparent with irregularities of the inner retinal layers (a) and mild cystoid edema can be seen in the sub-foveal area (b).
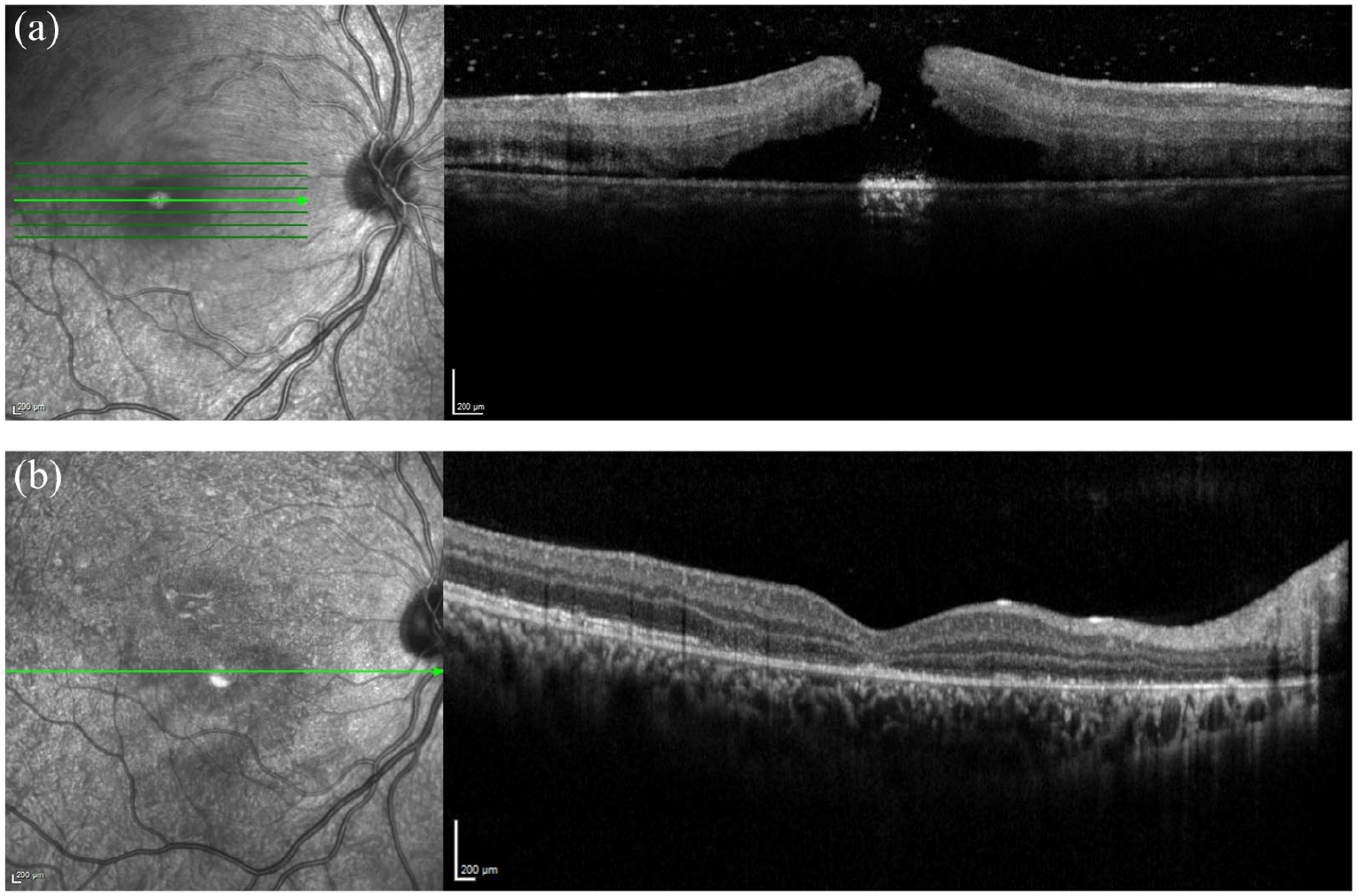
Macular OCT of a 14-year-old patient following direct blunt trauma from a soccer-ball. (a) At presentation: a full thickness macular hole with subretinal fluid and mild vitreous hemorrhage. (b) 12 days following injury: spontaneous closure of the traumatic macular hole with absorption of subretinal fluid (SRF) and foveal thinning of the outer retinal layers.
Duration of hospital clinic follow-up was up to 6 weeks in five cases (three eyes with retinal tear and two eyes with vitreous hemorrhage) in this group. VA was not affected and remained 20/20. These patients were considered eligible for follow-up in their community. Three patients were followed for 2 months or more: the patient with spontaneous closer of macular hole was lost for follow-up after 2 months and another patient with normal VA and macular pigmentary changes was followed for 8 months. The third patient that was treated for retinal detachment was followed for 20 months.
There were no significant differences between the severe and non-severe groups in terms of age at presentation, BCVA at presentation, or signs of external ocular injury (Table 2).
Comparison between severe a and non-severe groups at presentation.
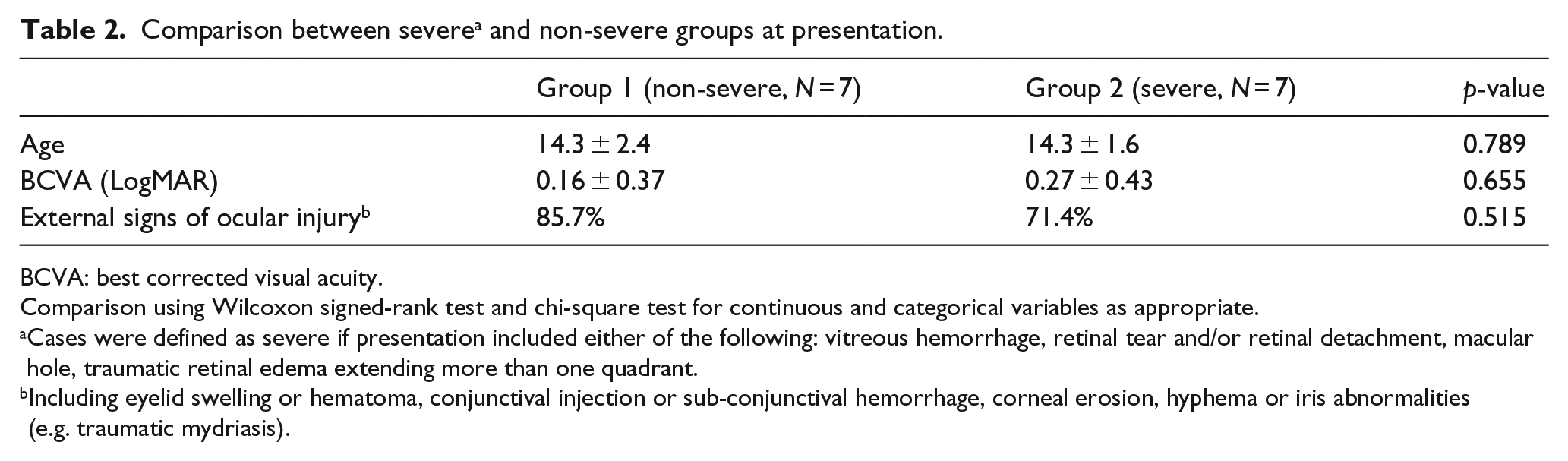
BCVA: best corrected visual acuity.
Comparison using Wilcoxon signed-rank test and chi-square test for continuous and categorical variables as appropriate.
Cases were defined as severe if presentation included either of the following: vitreous hemorrhage, retinal tear and/or retinal detachment, macular hole, traumatic retinal edema extending more than one quadrant.
Including eyelid swelling or hematoma, conjunctival injection or sub-conjunctival hemorrhage, corneal erosion, hyphema or iris abnormalities (e.g. traumatic mydriasis).
No signs of permanent pupil abnormalities were documented in any of the cases during the follow-up period including cases where traumatic mydriasis was observed at presentation.
Discussion
Closed globe soccer-ball-related blunt injury can lead to significant ocular morbidity in children. In this study, we reviewed all pediatric cases diagnosed with any form of retinal injury due to a soccer-ball ocular trauma over a 10-year period. A total of 50% of the cases were considered severe and 28% of patients, presented with significant injuries requiring immediate intervention due to retinal tears and detachment, and in two cases, the injury resulted in significant and permanent visual loss. No apparent risk factors for retinal injury (e.g. pathologic myopia) were found in any of the cases and all the children were injured during recreational activity and had no professional soccer training experience. All of the cases were males in our study, probably since soccer games are much more popular among boys than girls in Israel.
Capão Filipe et al. 7 prospectively collected data from 163 cases of soccer-related ocular injuries, with direct ball hit being the most common mechanism of injury. When compared to other ball-sports, the soccer-ball was found to penetrate less but remained in the orbital space 2.5–10 times as long. Out of 83 cases of vitreoretinal injury, a retinal break developed in 15 (18%) which progressed to retinal detachment in 7 cases. Vinger and Capão Filipe 4 describe the mechanics by which a soccer-ball kicked at high velocity can cause direct eye injury by entering the orbit. As the ball is usually kicked upward, the injury occurs mostly in the superior quadrant of the retina, similar to the findings in our series. This upward trajectory of the ball also suggests a higher velocity during impact as opposed to impact from the ball during its downward trajectory (i.e. closer to the kick-point), which might have also played a role in the mechanism of injury. However, this remains a speculation as all studies to lack exact data regarding the balls’ force of impact or vector.
The single most common cause of severe eye injury among children is sports. 8 Although, one might assume that soccer-ball trauma are less likely in children due to lower kick velocity and weaker impact than in adults, this assumption is most probably incorrect. Horn et al. 6 presented a collection of 13 cases of soccer-ball-related retinal injury, all but three were aged 14 years or younger. In their series, nearly half of the patients required surgical intervention. They suggested that the high frequency of pediatric eye injuries in their series was at least in part due to the flat orbital rims in the prepubescent and early teenage years which gives the globe greater prominence, theoretically enhancing the risk of injury. 9 In another larger series, out of 163 patients, which included both adults and children with traumatic soccer-related injuries, 22 (13.5%) required surgical intervention. 7 In our study, the rate of surgical intervention was much lower (7.5%), however, the severe group in our study composed half the study population, and the progression of retinal complications (e.g. retinal detachment) was probably prevented due to early detection of traumatic retinal tears and and treatment by laser retinopexy. Differences can also be attributed to variation in study population and inclusion criteria, as well as the fact that Horn et al. 6 reported a series of selected rather than consecutive cases.
Retinal injury related to blunt ocular trauma from soccer-ball was relatively uncommon in our pediatric retinal cases during 10 years (less than 5%). The rates of severe and non-severe cases were equal in our series. There were no statistically significant differences between the groups in term of age, VA, or presence of anterior segment findings. Capão Filipe et al. 7 also found no significant association between anterior segment and vitreoretinal lesions. This emphasizes that the lack of external signs of injury and good VA do not rule out the chance of injury to the posterior segment. Two out of four cases presenting with retinal tears in our series had no visible signs of injury and could have been easily missed if dilated fundus examination was not performed at presentation. The importance of a thorough exam, particularly of the peripheral superior retina, cannot be overstated.
The findings of our study also strongly support previous recommendations for use of ocular protection during soccer games to reduce both the incidence and the severity of ocular damage. 10 However, as all of the cases were of non-professional players, it is unlikely to assume that such recommendation will be held.
The main limitations of this study are its retrospective nature, and the short follow-up period in some of the cases, particularly those with mild injury. In addition, the study population is somewhat biased due to the presence of symptoms which lead them to seek eye examination and cannot determine injury rate among those who were not evaluated.
In conclusion, great precautions should be taken in all cases of ocular trauma related to soccer-ball injury in children. A thorough ocular evaluation with examination of the peripheral retina is mandatory regardless of the presence or lack of external signs of injury, preferably, shortly following injury. Ocular protective gear should be considered by all soccer players regardless of age.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.