
Abstract
Purpose:
To determine the total corneal refractive power in 1–8 mm corneal zones and the 8 mm Q-value in non-keratoconic patients with Down syndrome and normal subjects aged 10–30 years.
Methods:
Right eye data from 203 Down syndrome patients (mean ± standard deviation age: 17.0 ± 4.7 years) and 189 age- and gender-matched normal subjects (17.1 ± 4.5 years) were compared. Main extracted Pentacam indices were total corneal refractive power in steep and flat axes, and mean and difference (corneal astigmatism) total corneal refractive power in 1–8 mm zones.
Results:
Mean total corneal refractive power in 1–8 mm zones was 45.17–45.74 D and 42.91–43.52 D in Down and normal group, respectively (all p < 0.001). The coefficients of variation of total corneal refractive power from the center to the periphery were similar in the two groups (p = 0.855). None of the mean total corneal refractive powers significantly correlated with age, and all of them were significantly higher in females (p < 0.001). Mean total corneal refractive power–based corneal astigmatism in these zones changed from 1.46 to 1.66 D in Down syndrome patients and 1.64 to 1.99 D in normal group. All corneal astigmatism indices were similar between two groups (all p > 0.05). The prevalence of against the rule and oblique astigmatism in all zones were higher in the Down syndrome group (all p < 0.05).
Conclusion:
Adolescent and young non-keratoconic patients with Down syndrome have a more prolate cornea and a homogeneous keratometry distribution. In this population, females have a steeper cornea.
Keywords
Introduction
Keratometry is one of the main parameters for the diagnosis and treatment follow-up of ocular diseases, such as keratoconus, and is known to vary with age, especially in the corneal periphery. 1 It is suggested that patients with Down syndrome might be more prone to keratoconus;2,3 therefore, knowledge of reference ranges of keratometry in different age groups of Down syndrome patients is necessary for making accurate diagnoses. Ocular biometric studies in patients with Down syndrome suggest structural differences in these individuals compared to the general population and steeper corneas compared to normal individuals.4–6 These studies have used the 3-mm keratometry in the anterior cornea (simulated keratometry (sim-K)), which is calculated based on the assumption that the corneal thickness and the ratio between the anterior and posterior curvature are constant.
In addition to sim-K, other indices such as true net power (TNP) and total corneal refractive power (TCRP) can be used to represent corneal power. The TNP is calculated using the Gaussian formula in which the anterior and posterior surfaces and different refractive indices are taken into account. TCRP, which provides a more realistic measure, is calculated based on Snell’s law using the same four factors (anterior and posterior curvature and refractive indices of the cornea and aqueous humor) within a given corneal diameter. In calculating this index, refractive indices are 1 for air, 1.376 for the cornea, and 1.336 for aqueous humor. The disadvantage of TNP to TCRP is that the Gaussian formula is prone to error in irregular corneas. 7 Studies have shown that TCRP has a higher accuracy than the other two parameters (TNP and sim-K)7–10 and has good repeatability. 11
Since the total refractive power (anterior and posterior) of the cornea as well as keratometric changes beyond, the central 3 mm have an important role in clinical decision-making, and on the contrary, there is high variation in keratometric measurements in Down syndrome patients, 6 knowledge of the reference ranges of the anterior and posterior keratometry is essential for this patient population. Therefore, in the present report, in addition to the anterior keratometry in the central 3 mm (front sim-Ksteep and sim-Kflat), we examined the keratometric pattern and shape from the center to the periphery in a population of Down patients with normal corneas free of any clinical signs of keratoconus and compared them to an age- and gender-matched normal population.
Materials and methods
Study population
This article is part of a larger comparative population-based study which began in 2016 and recruited 250 patients with Down syndrome from the nation’s special needs schools, relevant non-profit organizations, and the Down Syndrome Society. Inclusion criteria of the original study were diagnosis of Down syndrome with no concurrent intellectual disability (e.g. Klinefelter syndrome, autism) and age between 10 and 30 years. Diagnosis of Down syndrome was confirmed in their medical records based on karyotype testing. For the comparison group, 200 age- and gender-matched normal subjects were recruited from candidates of refractive surgery presenting for their first work-up session (87 cases) as well as normal subjects presenting for a vision check-up (113 cases).
Exclusion criteria for this report were any corneal disease, such as pterygium or keratoconus, and any history of ocular surgery. The presence of keratoconus was detected by two subspecialists using clinical (Munson’s sign, Vogt’s striae, Fleischer’s ring, apical thinning, or Rizutti’s sign) and topographic (maximum keratometry, ART-max, inferior-superior asymmetry (IS-value), Belin–Ambrosio Deviation value (BAD-D), minimum corneal thickness (MCT), and posterior elevation map) findings.
Examinations and parameters
In addition to vision testing and a comprehensive ophthalmic examination, all participants underwent imaging with Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany), which was done between 8:00 a.m. and 12:00 p.m. Data were extracted using Oculus Inc. software version 6.08r27 and Pentacam 1.21r24 software. If necessary, imaging was repeated until OK status was generated. When imaging was repeated more than three times, another imaging session was scheduled in 2–3 days to avoid imaging error.
The parameters examined in this report included the central 3 mm anterior keratometry in two perpendicular axes and their average (sim-Ksteep, sim-Kflat, and Kmean), the maximum keratometry (Kmax) in the 8 mm zone, the TCRP in the steep and flat axes, mean TCRP in corneal zones 1–8 mm in diameter, TCRP-based corneal astigmatism (CA) in 1–8 mm zones (calculated as the difference between steep and flat axes TCRP), asphericity (Q-value) in the central 8 mm of the cornea, and anterior and posterior elevation at the corneal apex (based on a best fit sphere). CA was classified based on the meridian of the flat axis (based on TCRP) as with-the-rule (WTR: 0°−22.5° and 157.5°−180°), against-the-rule (ATR: 67.5°−112.5°), and oblique (all other).12,13
Ethical consideration
The research proposal was reviewed and approved by the Ethics Committee of Tehran University of Medical Sciences (ID: 1397-091) and adhered to the tenets of the Declaration of Helsinki in all steps. Since Down individuals are legally considered to lack the capacity to consent to research, the purpose and methods of the research were fully explained to potential participants and their parents/guardians, and we obtained parent consent and subject assent.
Statistical analysis
The fellow eyes in the Down group showed strong correlations for all studied variables. The lowest correlation coefficient was 0.882 for Ksteep of TCRP-1 mm and the highest was 0.947 for Kflat of TCRP-8 mm. Therefore, from both groups, only right eye data were used in the analyses.
Descriptive analyses were done to summarize the studied indices as mean ± standard deviation (SD) and 95% confidence intervals (CIs) of the mean. To examine the effect of Down syndrome (independent dichotomous variable: Down/normal) on the parameters of interest (dependent variables: TCRP, CA, Q-value, and elevation), we used multiple linear regression and controlled for confounders of age, gender, and refractive astigmatism. To examine the effect of Down syndrome on the prevalence of different types of astigmatism (dependent trichotomous variable: WTR, ATR, and oblique), we used multinomial logistic regression. In this model, WTR was entered as the reference, and refractive astigmatism was treated as a confounder. The coefficient of variation (CV) of change in the mean TCRP from the center to the periphery (1–8 mm zones) was calculated as the SD/mean.
Results
After applying the inclusion and exclusion criteria, right eye data of 203 patients with Down syndrome and 189 normal subjects were used in the analyses for this report. The mean age was 17.0 ± 4.7 and 17.1 ± 4.5 years in the Down and normal groups, respectively (p = 0.836), 52.7% of the Down and 48.1% of the normal subjects were male (p = 0.367), and mean refractive astigmatism was −1.83 ± 1.19 and −2.05 ± 1.57 D in the Down and normal groups, respectively (p = 0.126).
Corneal power
In the Down and normal groups, mean front sim-Ksteep was 46.60 ± 1.65 D and 44.47 ± 1.51 D, front sim-Kflat was 44.94 ± 1.49 D and 42.52 ± 1.46 D, and front Kmax was 47.20 ± 1.70 D and 44.93 ± 1.55 D, respectively (all p < 0.001). Mean TCRP in 1–8 mm zones was statistically significantly different between groups (p < 0.001) (Table 1) and genders (p < 0.001); mean TCRP values were higher in Down syndrome patients and female subjects (Figure 1). The CV for mean TCRP in 1–8 mm zones was 0.006 ± 0.003 and 0.006 ± 0.002 in Down and normal groups, respectively (p = 0.855).
Total corneal refractive power and shape in a 10- to 30-year-old cohort of patients with Down syndrome (n = 203 eyes) and normal subjects (n = 198).
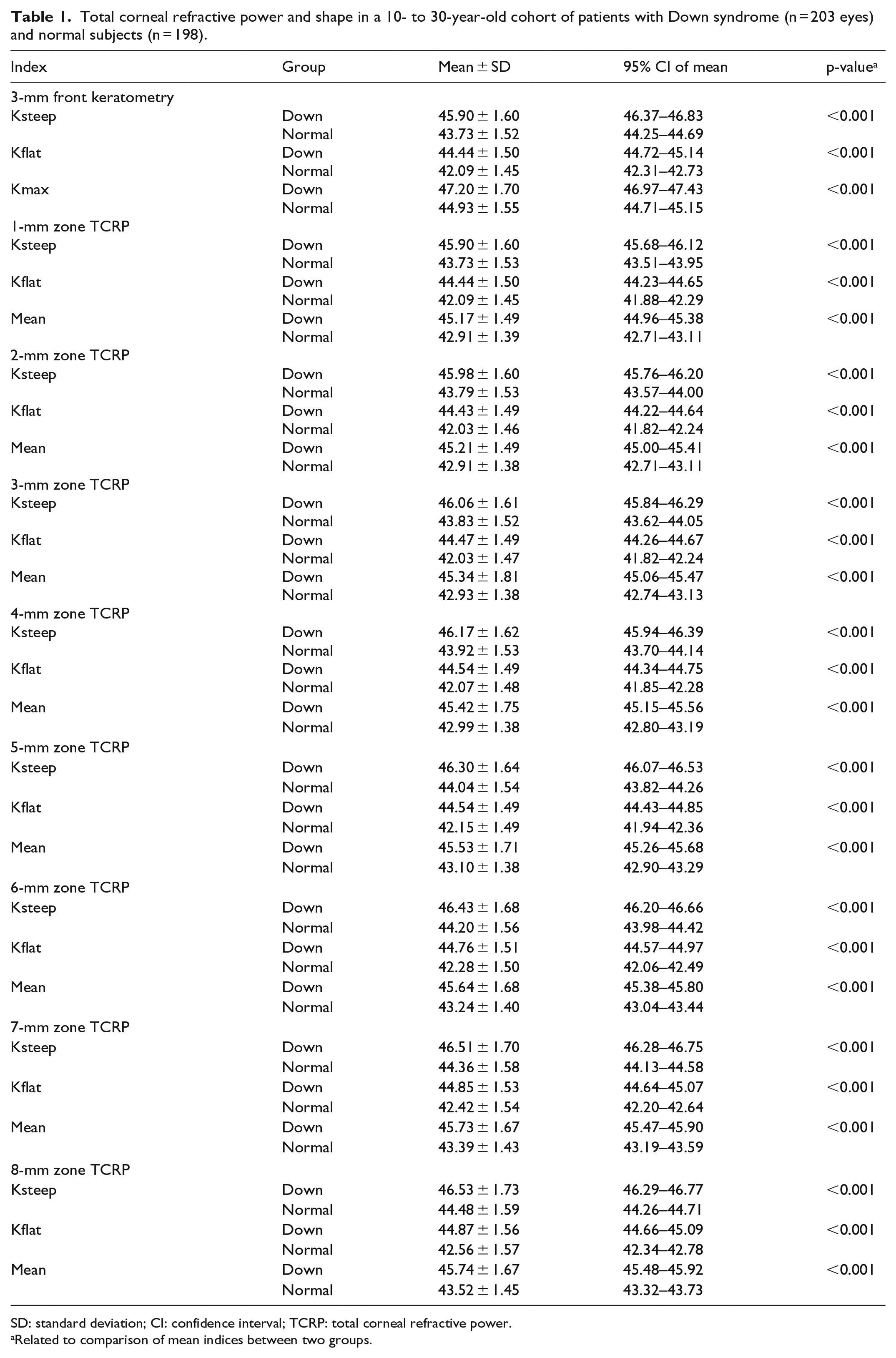
SD: standard deviation; CI: confidence interval; TCRP: total corneal refractive power.
Related to comparison of mean indices between two groups.
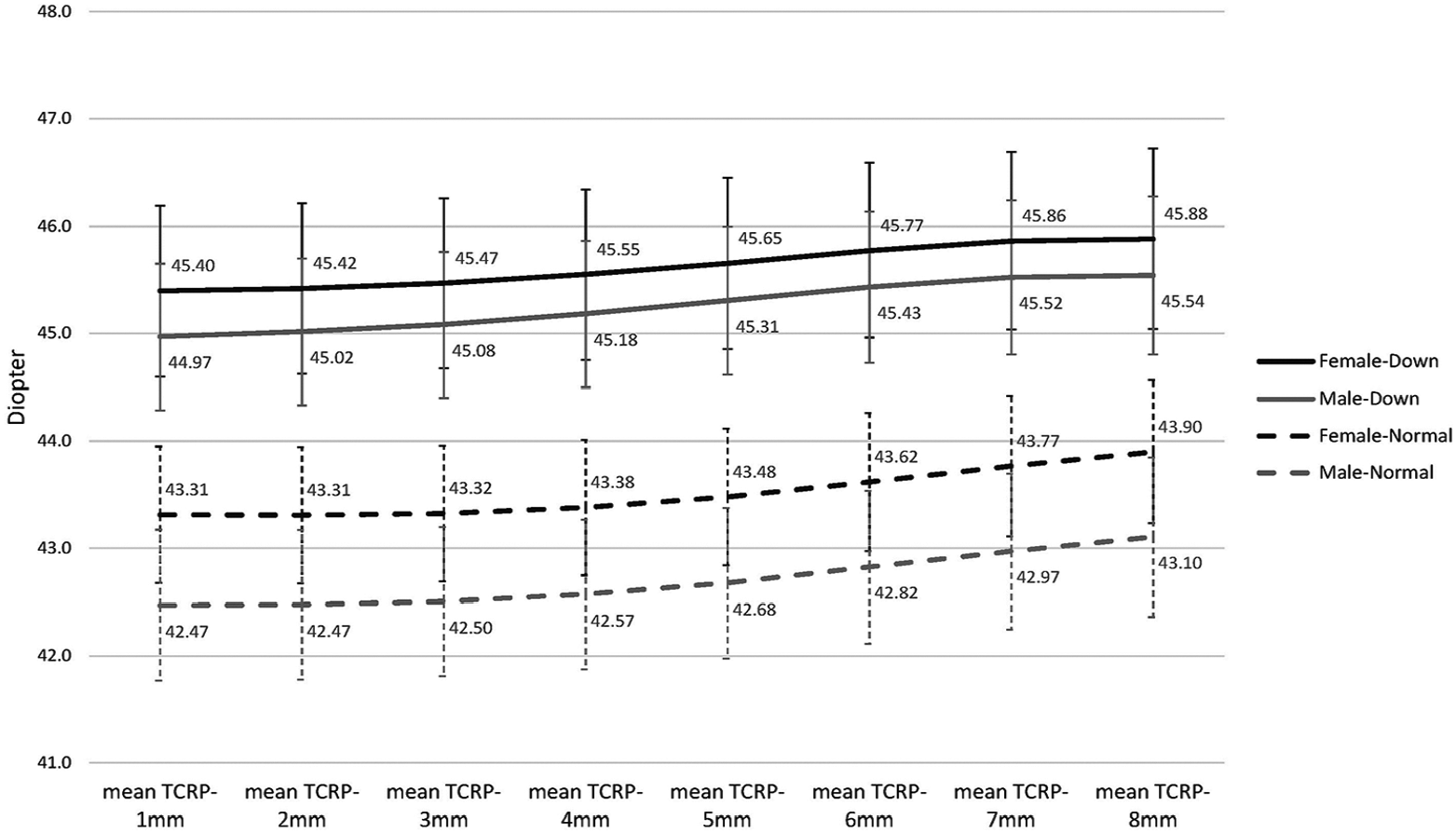
Inter-gender comparison of mean total cornel refractive power (TCRP) in patients with Down syndrome and normal subjects.
TCRP-based astigmatism
TCRP-based CA in 1–8-mm zones is shown in Figure 2. The multiple linear regression model showed that mean CA values were not statistically significantly different between the two groups (all p > 0.05). A significant correlation was also observed between age and CA-4 mm (β = −0.02, p = 0.05), CA-5 mm (β = −0.02, p = 0.037), CA-6 mm (β = −0.03, p = 0.030), CA-7 mm (β = −0.03, p = 0.032), and CA-8 mm (β = −0.02, p = 0.037). Inter-gender difference of all CA indices was non-significant (all p > 0.05).
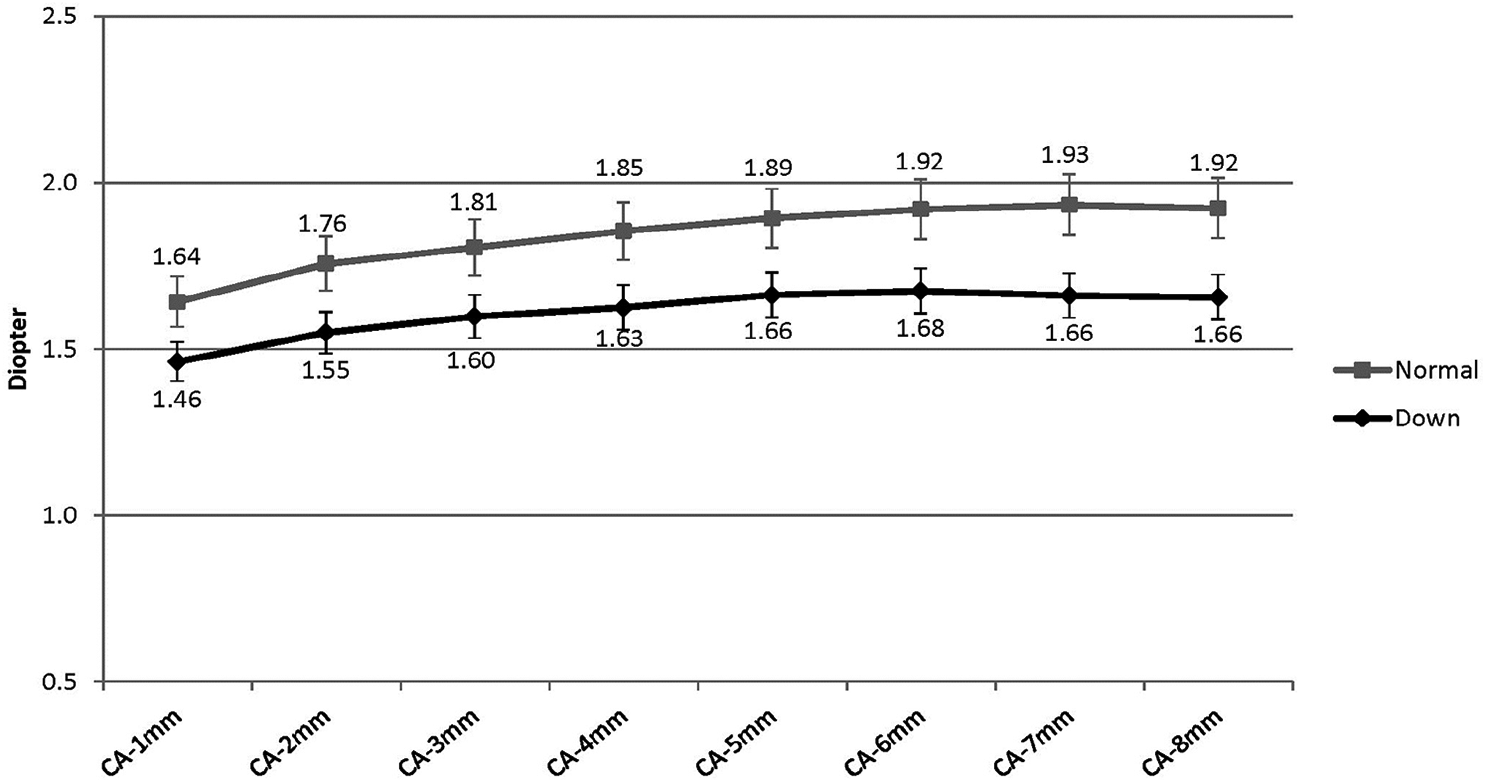
Corneal astigmatism (CA) calculated from the total corneal refractive power (TCRP) in corneal zones 1–8 mm in Down syndrome and normal group.
Figure 3 demonstrates the percentage distribution of WTR, ATR, and oblique astigmatism in 1–8 mm corneal zones in the two groups. The prevalence of ATR and oblique astigmatism in all zones were higher in the Down syndrome group (all p < 0.05). The prevalence of ATR and oblique astigmatism increased with aging (all β ⩽ −0.02, all p < 0.05).
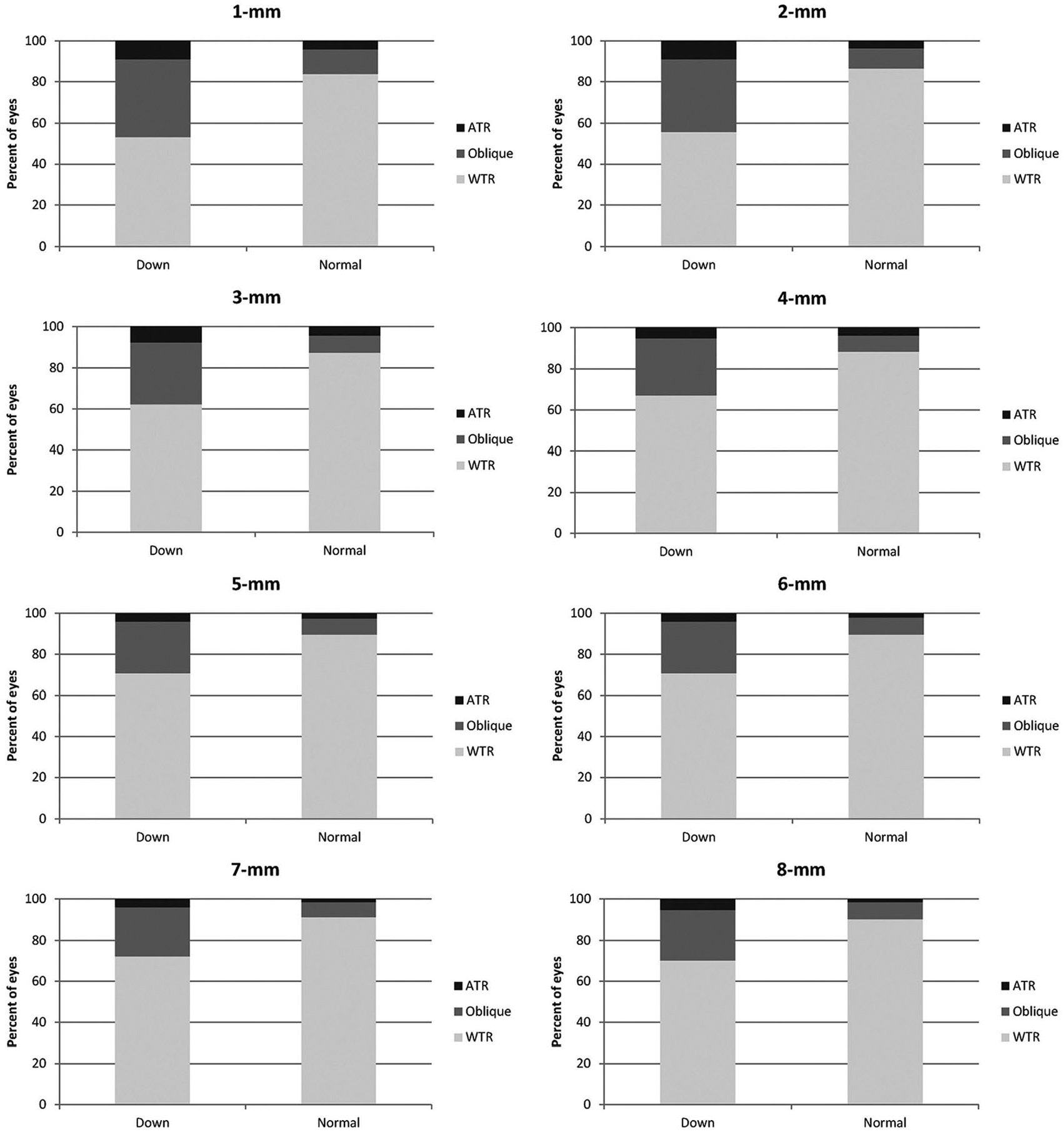
Comparison of types of corneal astigmatism (CA; calculated from the total cornel refractive power) between the Down syndrome and normal group.
Asphericity and elevations
In the Down and normal groups, Q-value was −0.55 ± 0.16 (95% CI: −0.57 to −0.53) and −0.41 ± 0.12 (95% CI: −0.42 to −0.39), respectively (p < 0.001). Q-value correlated with age (β = −0.004, p = 0.012) and became more negative (more prolate) up to the age of 30 years. The correlation between Q-value and gender was not significant (β = 0.003, p = 0.855). There was a significant correlation between Q-value and all CA indices (all β ⩽ −0.02, all p < 0.001), except for CA-8 mm (β = −0.01, p = 0.124).
Best fit sphere apical anterior elevation was 3.40 ± 3.19 µm (95% CI: 3.19 to 3.62) and 2.61 ± 0.95 µm (95% CI: 2.48 to 2.75) (p < 0.001) and posterior elevation was 2.55 ± 2.59 (95% CI: 2.19 to 2.91) and 2.38 ± 2.12 (95% CI: 2.07 to 2.68) (p = 0.476), in the Down and normal groups, respectively. Anterior apical elevation was independent of age but significantly higher in females (β = 0.295, p = 0.028). Apical posterior elevation was also independent of age and higher in females (β = 0.626, p = 0.009).
Discussion
Pentacam has been used for measuring the corneal curvature in various studies of normal populations. One of the advantages with this device is the measurement of the posterior corneal curvature which can be used for the accurate estimation of corneal power. Although some authors believe posterior corneal indices add no value to the diagnosis of keratoconus, 14 others suggest that posterior corneal curvature has an important role in different fields, such as differentiation of subclinical keratoconus from normal, 15 and in the accurate calculation of intraocular lens (IOL) power in cataract patients. 16 The importance is highlighted in patients with Down syndrome due to their higher risk for keratoconus 2 and higher prevalence of cataract. 17
TCRP is the preferred measure of corneal power compared to other indices. In fact, TCRP is the most accurate measure of corneal power and astigmatism before refractive surgery. 10 TCRP, as measured with Pentacam, is also highly repeatable, especially in larger diameters, and the repeatability is better than that for sim-K in almost all zones. 11 Also, in irregular corneas that diverge from the Gullstrand formulas, ray-tracing TCRP can generate a more precise model. 7 Given the quicker stabilization after therapeutic interventions, TCRP can even be a good index for surgical planning in sequential approaches. 18 Therefore, in this study, this index was studied in addition to sim-Ks, and it was used to show the patterns of corneal curvature in this sample of patients with Down syndrome.
In agreement with our results, several population-based studies have reported sim-Ksteep and sim-Kflat to be approximately 44.0 and 43.0 D in normal samples in this age range (10–30 years).19–21 Although different devices (Pentacam and Orbscan) have been used in these studies, there is no significant variation among the reported ranges. To the best of our knowledge, no population-based studies have yet reported the reference range of TCRP-based Ksteep and Kflat in patients with Down syndrome or normal subjects.
In the Down syndrome group of this study (with participants’ average age of 17 years), mean sim-Ks were approximately 46.6 and 45.0 D, Kmean was 46.0 D, and no correlation was observed with age. In other studies of Down syndrome samples, Kmean was 46.7 D in 7-year-olds, 22 45.5 D in 9-year-olds, 23 45.6 D in 13-year-olds, 24 46.6 D in 15-year-olds, 25 and 46.4 D in 20-year-olds. 5 Although different devices were used in these studies, overall, results indicate that the 3-mm keratometry of the anterior cornea in patients with Down syndrome is higher than the normal population. None of these studies assessed mean TCRP.
In our study, the variation (CV) of TCRP from the corneal center to periphery in our sample of non-keratoconic Down syndrome patients suggested a homogeneous pattern of curvature distribution in Down syndrome patients in favor of a prolate shape. Therefore, it is necessary to define the normal range of sim-Ks specifically for Down syndrome patients. Based on the 95% CI in non-keratoconic Down syndrome cases in this study, sim-K can range from 44.7 to 45.1 D in the flat axis and from 46.4 to 46.8 D in the steep axis, and the upper limit of front Kmax can be 47.4 D without any clinical sign of keratoconus. While, in normal subjects, 95% CI of sim-Ksteep and sim-Kflat was 44.2–44.7 D and 42.3–42.7 D, respectively, and the upper limit of Kmax was not higher than 45.1 D.
In this study, TCRP-based CA increased from 1.5 D in the center to 1.7 D in the periphery. In the study by Doyle et al. 26 on a sample of Down syndrome patients with a mean age of 17.5 years, mean astigmatism was 1.14 D. Knowlton et al. 6 reported a CA of 1.7 D in a 25-year-old sample of patients with Down syndrome. High CA can be due to the characteristic morphology of the eyelids and the unique shape of the palpebral aperture in these patients.27,28
In both groups of our study, the prevalence of WTR astigmatism was higher than other types of astigmatism in all diameters. However, Doyle et al. 26 reported a higher prevalence of oblique astigmatism than WTR astigmatism in their sample of Down patients. This discrepancy is probably because axis orientation was categorized differently: 0 ± 22.5°/90 ± 22.5° in this study and 0 ± 10°/90 ± 10° in theirs. Literature suggests that astigmatism axis orientation can be a factor of eyelid morphology, 29 visual habits, 30 genetic factors, 31 and ametropia. 32
Studies suggest that ATR CA in normal eyes shifts toward WTR between the ages of 4 and 18 years, and it reaches stability afterward up to the age of 40 years; this change has been attributed to eyelid pressure. 33 However, as we observed in this study, Down individuals seem to have a different change in astigmatism orientation, and as illustrated in Figure 2, they experience slow or halted axis rotation. Since they have more prolate corneas, the mechanical pressure from an upslanted palpebral fissure and eye rubbing 5 can intervene the rotation from ATR to WTR and lead to induced oblique or ATR astigmatism in this age range.
The shape of cornea in patients with Down syndrome (−0.55) was more prolate than the normal subjects (−0.41); which in addition to the TCRP distribution provide stronger evidence to previous research suggesting that the corneas in Down patients are more prolate. As such, a similar corneal morphology was observed in the assessment of the corneal thickness and volume in this very sample. 34 The corneal thickness and volume in the corneal center and all rings up to the 8-mm periphery were noticeably less in non-keratoconic Down cases compared to the normal comparison group. Of note, analyses of elevation data showed that the difference between Down patients and the normal sample was mostly in anterior corneal elevation (0.8 µm) than posterior (about 0.2 µm). This could mean that the inter-group difference in corneal shape mostly lies in the anterior corneal surface. Similarly, the difference between sim-k1 and simk-2 in the study by Alio et al. 25 was 3.35 D in the anterior cornea and about 0.3 D in the posterior cornea.
Although Down syndrome participants had steeper corneas, they demonstrated less toricity, that is, while the flat meridian was much steeper than the normal group, the steep meridian was just slightly steeper. This can be due to the upslanted palpebral fissure in Down individuals. There is no consensus on the correlation between asphericity and radius of curvature. Pérez-Escudero et al. 35 showed that steeper corneas are more prolate. Davis et al. 36 found no correlation between apical radius and asphericity. Zhang et al. 37 showed a weak but significant correlation (r =−0.09, p = 0.004). We also observed a weak but significant correlation between TCRP-based CA and asphericity. These inconsistencies may be related to inter-study differences in the age of the subjects, measurement devices, indices, and measurement diameters.
In this study, age-related changes in CA and Q-value were very small (all β ⩽ −0.03) but significant; this could be due to the narrow age range (10–30 years old) of our sample. Other studies with wider age ranges reported greater changes in these indices.38,39 In agreement with other studies,40–42 our results indicated that females have more steep corneas. In contrast, Cheung et al. 43 reported similar Q-values for the two genders, although the small sample size (63 subjects) and low power may be responsible for the non-significant inter-gender difference.
The strength of this double-arm population-based study is the large sample size of Down syndrome patients in a relatively wide age range (10–30 years) and presenting the reference range of novel parameters (TCRPs) from the central to peripheral cornea. Also, sampling was done from different sources which could improve the generalization of the findings. Previous studies4–6 were done on limited clinical samples and evaluated only anterior sim-K without paracentral and peripheral indices. A limitation of our study is that the age range did not allow for the evaluation of age-related changes. Overall, it can be concluded that compared to normal samples, patients with Down syndrome have a more prolate cornea, which is not necessarily indicative of keratoconus. Therefore, it is important to define the diagnostic criteria for pathologic conditions such as keratoconus for patients with Down syndrome. The age-related keratometric changes and its gender distribution are similar to that in non-Down subjects, although the predominant type of astigmatism is WTR, and the rotation is slower than normal subjects or does not occur.
Footnotes
Acknowledgements
The authors alone are responsible for the content and writing of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.