
Abstract
Aim:
The aim of this study was to assess and compare the visual, refractive, and topographic outcomes of keratoconic eyes treated with corneal collagen cross-linking combined with and without same day intrastromal corneal ring segment over the first 12 months.
Methods:
This prospective randomized study analyzed 38 eyes of 30 consecutive keratoconus patients aged 26.21 ± 6.97 (range = 15–41) years. A total of 20 eyes were treated with collagen cross-linking alone, and 18 eyes underwent collagen cross-linking combined with simultaneous femtosecond laser-assisted intrastromal corneal ring segment. Visual acuity, manifest refraction, and corneal topography (using a rotating Scheimpflug topographer) were assessed and compared between the two groups at baseline, 6, and 12 months.
Results:
On an average follow-up duration of 12.2 ± 0.50 (range = 11–13) months, both collagen cross-linking alone and collagen cross-linking with simultaneous intrastromal corneal ring segment implantation were effective. However, collagen cross-linking plus intrastromal corneal ring segment resulted in an additional improvement of uncorrected distance visual acuity of 0.16 (95% confidence interval = 0.01 to 0.32) logarithm of the minimum angle of resolution units (p = 0.035), cylindrical power by 1.16 D (95% confidence interval = 0.25 to 2.06, p = 0.014), and spherical equivalent by 1.40 D (95% confidence interval = −2.71 to −0.08, p = 0.038) at 1 year. During the study period, no serious intraoperative or postoperative complications were noted in either group.
Conclusion:
One-year follow-up results suggest that collagen cross-linking with simultaneously combined intrastromal corneal ring segment implantation could yield an additive visual and refractive outcome. The combined procedure is safe and merits consideration for the treatment of progressive keratoconus to achieve better visual rehabilitation.
Introduction
Keratoconus (KCN) is a bilateral, asymmetric, chronic corneal ectasia, characterized by progressive thinning of the corneal stroma, steepening and scarring of the cornea that leads to severe visual impairment if left untreated. 1 It is more prevalent with earlier onset and greater progression in the population of Indian origin as compared to the white population.2,3 Furthermore, the cornea of the Indian population is markedly thinner and steeper than other races posing a greater risk of KCN.4,5 Hence, there is a need to identify an effective treatment option for this condition. The two treatment procedures identified to have gained popularity over the years are corneal collagen cross-linking (CXL) with riboflavin and ultraviolet-A (UV-A) and intrastromal corneal ring segments (ICRS). 6
Randomized controlled studies have reported that corneal CXL with riboflavin and UV-A is mainly a stabilizing procedure that has no aim to correct the refractive error associated with KCN. However, CXL is sometimes associated with unpredictable and uncontrollable improvement in the refractive status of KC mainly in the myopic component.7–12 ICRS is based on arc-shortening effect within the cornea; the additional volume of ICRS redistributes the biomechanical stress of the corneal lamellae, thus flattening the central cornea.13,14 Regardless of the type, ICRS targets to flatten the cornea to improve the myopic and astigmatic components of KCN. Several studies have confirmed the efficacy of ICRS in corneal ectatic disorders.15–19 However, since ICRS has no role in the prevention of KCN progression, it has to be combined with CXL. 20
CXL slows or halts progression while ICRS flattens the cornea; both significantly benefit a KCN patient. The mechanism of improvement differs between the procedures, hence theoretically, a simultaneously (same sitting) combined procedure could produce a potential additive outcome. However, there are no studies to test the hypothesis. The aim of this study was to assess and compare the vision, refraction, and corneal topography over a period of first 1 year and determine whether CXL with simultaneous ICRS implantation was significantly better than CXL alone for the management of KCN.
Subjects and methods
Study design and participants
This was a prospective, randomized study and recruited consecutive KCN patients from Eye7 Chaudhary Eye Centre, New Delhi. All the examinations, treatments, and follow-ups were carried out at the same center between January 2015 and August 2016. The approval for the study was obtained from the Institutional Ethical Committee (ICE) of Amity University, Haryana, India, and conformed to the tenets of the Declaration of Helsinki and ICMR-ICH-GCP guidelines. Prior to the enrollment in the study, detailed information sheets were provided to the subjects and informed consent obtained stating their acceptance to voluntarily participate in the study and use of the clinical data for publication.
The study enrolled subjects of Indian origin with progressive KCN, and participants were graded using RETICS classification based on the level of preoperative visual acuity. 21 Patients with spectacle-corrected distance visual acuity (CDVA) > 0.04 logarithm of the minimum angle of resolution (logMAR; 0.9 decimal) was Grade 1, CDVA of 0.04 logMAR (0.9 decimal) or less but equal to or better than 0.22 logMAR (0.60 decimal) was Grade 2; CDVA worse than 0.22 logMAR (0.60 decimal) but equal to or better than 0.40 LogMAR (0.4 decimal) was Grade 3; CDVA less than 0.40 LogMAR (0.4 decimal) but equal to or better than 0.7 logMAR (0.20 decimal) was Grade 4; and CDVA less than 0.7 logMAR (0.20 decimal) was Grade Plus.
Subjects recruited exhibited (1) corneal irregularity, as determined by distorted keratometric mires and/or scissor retinoscopic reflex, and (2) at least one slitlamp biomicroscopic sign (Vogt’s striae, Fleischer’s ring of more than 2 mm of arc, or corneal scarring typical of KCN). However, subjects below the age of 12 years, pregnant, or breastfeeding females at the time of recruitment were excluded. Eyes with ocular pathology other than KCN, previous history of refractive or corneal surgery, thinnest pachymetry of fewer than 400 µm, and pupillary diameter more than 7.0 mm were also excluded from the study.
Randomization and blinding
Eligible participants were recruited and a list of participant identity numbers was prepared. Using it, computer-generated randomization was done to allocate the participants to Group 1 (CXL alone) and Group 2 (CXL with simultaneous ICRS implantation) to undergo the procedures. Data were collected by a trained optometrist, blinded to the two treatment options. The participants could not be blinded due to the nature of the study. The data analyst was also blinded to the intervention.
Examination protocol
All the surgical procedures were performed by the same surgeon (R.B.), and investigations were carried out by the same optometrist (I.P.S.) following standardized and uniform techniques. Preoperatively, all the subjects underwent a comprehensive ophthalmic examination, which included distance visual acuity assessment with logMAR chart at 4 m, manifest refraction (sphere, cylinder, and spherical equivalent) with a streak retinoscope (Heine Beta 200), anterior segment evaluation using slitlamp biomicroscope (SL-D2; Topcon), intraocular pressure measurement with Goldmann applanation tonometry (Haag-Streit AG), and retina evaluation with indirect ophthalmoscope. It was followed by corneal topography measurements using a rotating Scheimpflug camera (WaveLight® Oculyzer II; Alcon). All the participants underwent the procedure within 1 month of the preoperative investigations.
Surgical techniques
In Group 1, CXL was performed according to the standard Dresden Protocol. The eye was anesthetized with topical eye drop (proxymetacaine hydrochloride 0.5%), and the central 8 mm of the corneal epithelium was removed. The standard epithelium-off CXLwas considered as the treatment of choice as it gave better results in KCN. 22 It was followed by applying the riboflavin solution (0.1% riboflavin-5-phosphate and 20% dextran T-500) for 30 min before irradiation and every 5 min during irradiation to the corneal surface. The cornea was then exposed to the radiation using UV-A light double diodes (370 nm) with 3 mW/cm2 irradiance at 1 cm distance for 30 min.
In Group 2, ICRS implantation was done prior to CXL. The intrastromal tunnel was created with the help of Femtosecond Laser (WaveLight FS200; Alcon), and the ICRS (Intacs®; Addition Technology, Inc.) was implanted manually at 70%–80% corneal depth. After the insertion of the Intacs, the incisions were closed with a 10-‘0’ nylon suture. The number, arc-length, and thickness of the ICRS were selected based on the manufacturer’s nomogram. Following the ICRS implantation, the standard epithelium-off CXL was performed as described for Group 1.
After the surgical procedure, the eye was washed with a sterile saline solution, antibiotic eyedrop was applied, and a bandage contact lens was inserted. Postoperatively, antibiotic-steroid eye drop was prescribed for 2 weeks and bandage contact lens was removed after 3 days.
Outcome measures
Subjects of both the groups were evaluated preoperatively (baseline), at 6 months, and at 12 months from the date of treatment. The primary measurements recorded were uncorrected distance visual acuity (UDVA), CDVA, and manifest refraction (spherical power, cylindrical power, and spherical equivalent). The secondary measurements included simulated keratometry (K1, K2), average keratometry (Kavg), maximum keratometry (Kmax), Q-value, pachymetry (pupil center, apex, thinnest), corneal volume, anterior chamber depth (ACD), and D-value (Belin/Ambrosio Display). Q-value is the asphericity factor, and D-value indicates the standard deviation from mean of the final overall map reading taking five parameters into account: (1) changes in front surface (Df), (2) changes in back surface (Db), (3) pachymetric progression (Dp), (4) thinnest pachymetry (Dt), (5) and thinnest pachymetry displacement (Dy) performing a regression analysis against a standard database of normal and KCN corneas.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (IBM SPSS Version 21) for Windows. A sensitivity power analysis using a computer program (GPower 3.0) showed that effect size between the two groups was 1.20 (large) with power (1 − β) set at 0.80 and α = 05, two-tailed. The sample size taken was considered adequate for the study. The demographic characteristics and baseline clinical data were analyzed with descriptive test and one-way analysis of variance (ANOVA), respectively. Student’s t-test was carried out for comparison of the parameters between the two procedures. Variations over time from baseline to 6 and 12 months postoperatively were assessed using ANOVA for repeated measurements and post hoc Bonferroni corrections where applicable. All statistical analyses were two-sided and values of p less than 0.05 was considered as statistically significant.
Results
Demographics
In this study, 44 eyes (of 33 KCN subjects) were enrolled. However, only 38 eyes (of 30 KCN subjects) aged 26.21 ± 6.97 (range = 15–41) years completed the study (follow-up rate of 86.4%).
Group 1 recruited 20 (52.63%) and Group 2 recruited 18 (47.37%) keratoconic eyes. The mean follow-up was 6.7 ± 0.7 months and 12.2 ± 0.5 months for Group 1 and 6.6 ± 0.6 months and 12.1 ± 0.6 for Groups 2 (p > 0.05). In general, the demographic characteristics of the participants of the two treatment groups were similar. The difference in the mean age, gender, and eyes for intervention between the two groups was insignificant (Table 1).
Demographic characteristics of the subjects by treatment group at baseline.
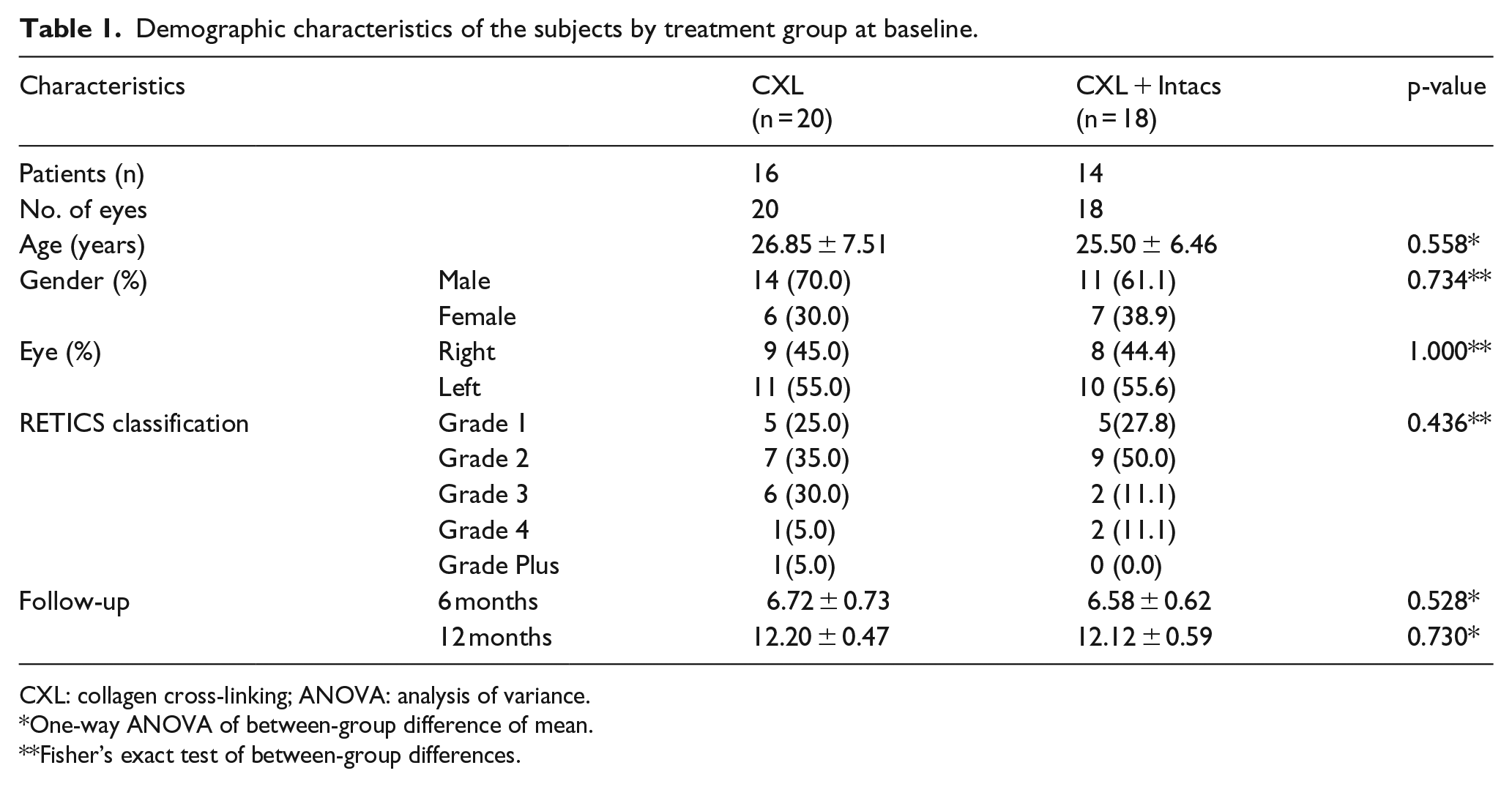
CXL: collagen cross-linking; ANOVA: analysis of variance.
One-way ANOVA of between-group difference of mean.
Fisher’s exact test of between-group differences.
At the baseline (preoperatively), the two treatment groups were matched. There was no significant difference amid vision, refraction, and corneal topography uncorrected distance between the two groups (p > 0.05, 95% confidence interval (CI) for all). Although not significant, astigmatism and Kmax were relatively advanced in the CXL with ICRS group (Table 2).
Clinical characteristics of the subjects by treatment group at baseline.
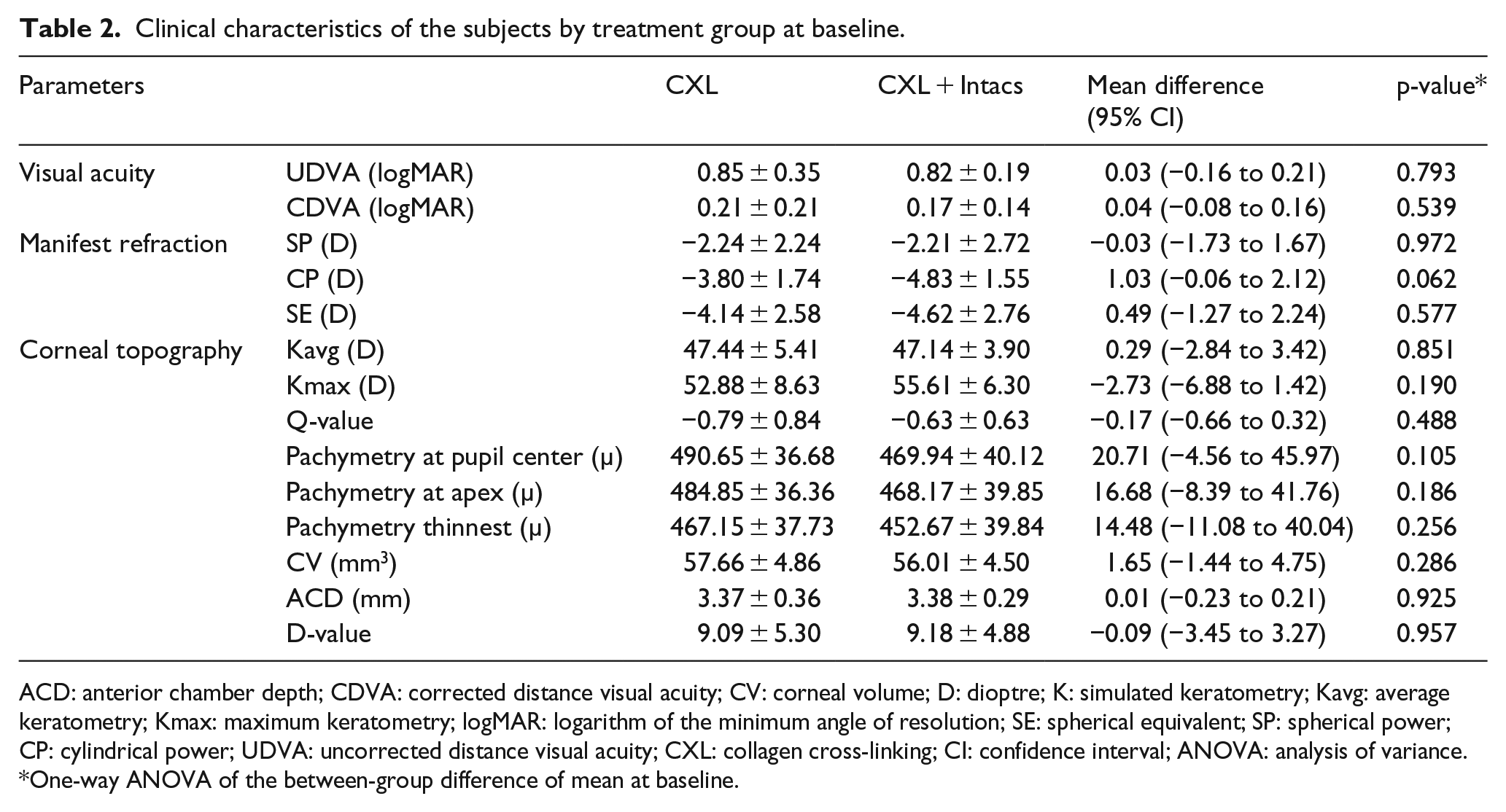
ACD: anterior chamber depth; CDVA: corrected distance visual acuity; CV: corneal volume; D: dioptre; K: simulated keratometry; Kavg: average keratometry; Kmax: maximum keratometry; logMAR: logarithm of the minimum angle of resolution; SE: spherical equivalent; SP: spherical power; CP: cylindrical power; UDVA: uncorrected distance visual acuity; CXL: collagen cross-linking; CI: confidence interval; ANOVA: analysis of variance.
One-way ANOVA of the between-group difference of mean at baseline.
Clinical outcomes
The visual, refractive, and topographic outcomes between the groups were compared at 6 and 12 months. The CXL with ICRS group showed an additional improvement over CXL alone for UDVA, cylindrical power, and spherical equivalent at 6- and 12-month follow-ups. The combined procedure had an additive effect of 0.16 (95% CI = 0.01 to 0.32) logMAR units (p = 0.035) and compared to CXL alone at 1 year (Figure 1). Furthermore, additional decrease in cylindrical power by 1.16 D (95% CI = 0.25 to 2.06, p = 0.014) and spherical equivalent by 1.40 D (95% CI = −2.71 to −0.08, p = 0.038) was achieved in the CXL plus ICRS group at 1 year (Figure 2). The difference in corneal volume noted at 6 months (p = 0.026) was not significant at 12 months (p = 0.124). The comparison of the visual, refractive, and corneal topographic outcomes between the two treatment groups at 6 and 12 months after the procedure is shown in Table 3.
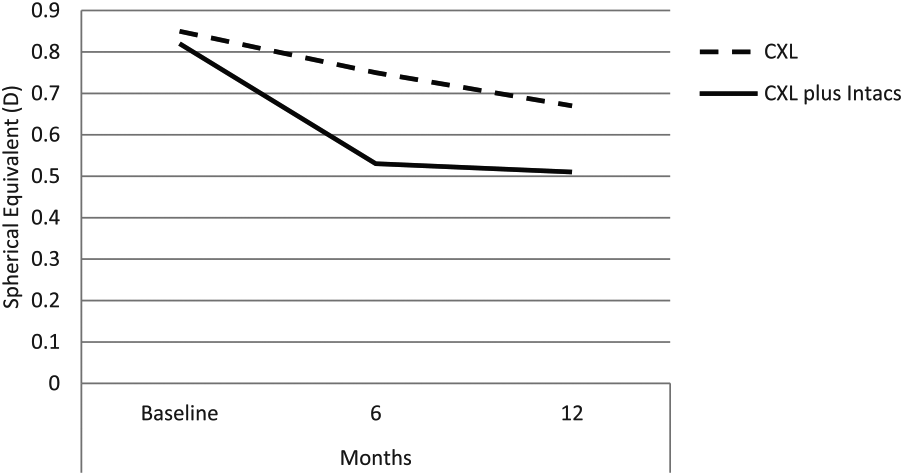
Changes in uncorrected distance visual acuity (logMAR) by groups over time.
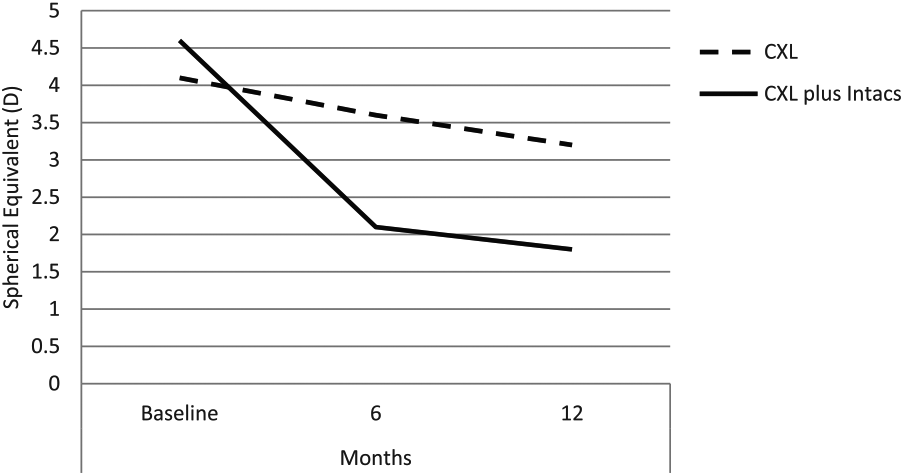
Changes in spherical equivalent (dioptre) by groups over time.
Comparison of the clinical changes at 6 and 12 months between the two groups.
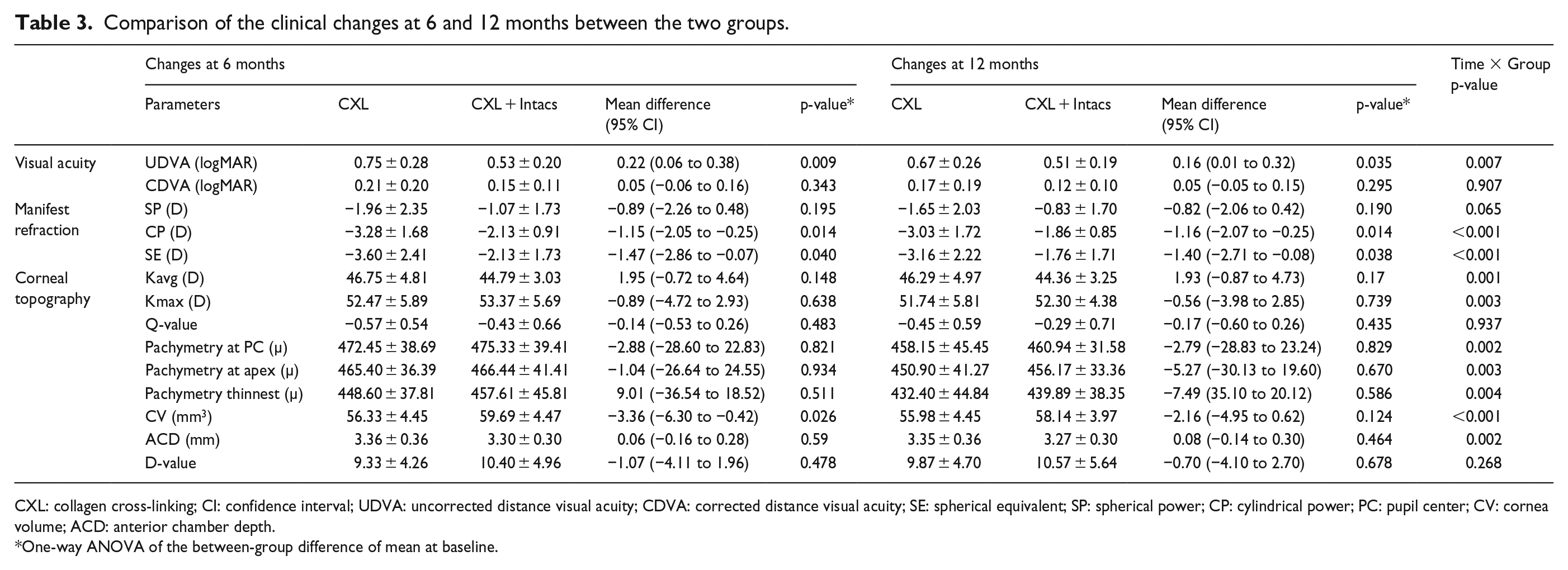
CXL: collagen cross-linking; CI: confidence interval; UDVA: uncorrected distance visual acuity; CDVA: corrected distance visual acuity; SE: spherical equivalent; SP: spherical power; CP: cylindrical power; PC: pupil center; CV: cornea volume; ACD: anterior chamber depth.
One-way ANOVA of the between-group difference of mean at baseline.
All interventions were well tolerated and no serious intraoperative or postoperative complications were noted in both the procedures during the study period. There were no reports of infectious keratitis, corneal scarring, extrusion of the segments, or perforation of the eye. Minor conditions like CXL-associated corneal haze and ocular discomfort were resolved in all participants within the first 3 months of the intervention.
Discussion
The effectiveness of CXL and ICRS for management of KCN is well established. This 1-year pilot study provides evidence to support that CXL combined with simultaneous ICRS implantation is safe and, particularly, more effective than CXL alone.
During the first year follow-up, both treatment options were effective to treat progressive KCN. However, the comparison of the vision, refraction, and corneal topography demonstrated that the combined procedure had an additive effect over CXL alone. CXL plus Intacs showed an additional improvement of 0.22 logMAR units (more than 2 lines) at 6-month follow-up and 0.16 logMAR units (more than 1.5 lines) at 12-month follow-up. This result concurred with a similar study where Keraring® combined with CXL improved UDVA from 1.18 ± 0.42 logMAR to 0.44 ± 0.22 logMAR units. 23 The improvement in UDVA could be attributed to a decrease in astigmatism (cylindrical power). However, there was no contrast in CDVA amid the two groups which could mean a similar improvement after refractive correction. The increase in unaided visual acuity may indicate that the patient may become more satisfied and less dependent on optical correction like spectacles or contact lenses after undergoing the combined procedure.
We also observed a relatively greater decrease in spherical power in the combined procedure. In the CXL with Intacs group, the astigmatism-related parameter showed that manifest cylindrical power reduced from −4.83 ± 1.55 D at baseline to −2.13 ± 0.91 D at 6 months and −1.86 ± 0.85 D at 12 months. This improvement was significantly better than the CXL-alone group. This finding was comparable to ICRS (Keraring) implantation followed by CXL, which resulted in a reduction of astigmatism from −4.68 ± 2.60 D to −2.20 ± 1.67 D at 13 months. 24 Our evaluation of average keratometry (Kavg) indicated that the dual procedure resulted in an additional flattening of 1.93 D at 12 months, but it did not prove significant. Similarly, maximum keratometry (Kmax) indicated an additional flattening of 0.56 D at 12 months, similar to findings reported elsewhere. 25 The further flattening in Group 2 could be elucidated by the redistribution of corneal lamellae and the matrix around it, just as it occurs in an intact cornea with KCN. 26 In contrary, some studies also suggest that Standard Intacs reduce mean keratometry reading by 3.00–5.00 D.27–29 About 1.00 D could be further enhanced by combining Intacs with CXL, and the results were more durable.30,31 It may not be possible to pre-determine the exact additive effect in the refraction of the combined procedure, because the unpredictable and uncontrollable effect of CXL could result in even more unpredictable effect in the refraction of the ICRS. However, analysis of the two groups in this study proves that CXL with ICRS will have a better refractive outcome. These findings were consistent with previous studies which assessed the pre- and postoperative parameters of CXL plus (CXL with femtosecond laser ICRS implantation) and concluded that the combined procedure was successful, effective, and safe.32,33
We noted a comparatively less thinning of corneas at the pupil, apex, and thinnest location in the combined procedure. It was in agreement with a study where central corneal thickness (CCT) decreased from the mean baseline reading (p < 0.003). 34 The corneal volume was found to increase (p = 0.026) in the combined procedure group at 6 months, but with an insignificant difference at 12 months. This initial increase could be attributed to the volume of the Intacs segment. We observed a significant decrease in ACD in both the procedures over the period, a common observation to other studies.35–37 The cause of the decrease is not clearly understood and requires further investigations. The corneal asphericity (indicated by Q-value) remained almost consistent throughout in both the groups. It could indicate that cornea treated with any of the two procedures could produce similar optical aberrations of the eye. During the study period, no surgical or postoperative complication was encountered indicating both procedures were equally safe.
The study was limited by the short follow-up duration and a low number of cases analyzed. Longer follow-up could not be documented as five participants shifted to specialty contact lens after 12 months. To further confirm the additive effect of CXL with ICRS, we suggest performing long-term randomized controlled trials (RCTs).
In conclusion, the clinical outcomes over the 1-year pilot period documented that both treatment approaches were safe and effective. However, the simultaneously combined procedure showed a greater improvement in UDVA and reduction in cylindrical power (astigmatism). The CXL with ICRS implantation could be considered over CXL alone for better visual rehabilitation.
Footnotes
Acknowledgements
The authors thank Dr Sanjay Chaudhary, Director of the Eye7 group of eye hospitals, for the general support during the study and Dr Aparna Gupta, Consultant Ophthalmologist, for the guidance. The authors also thank all the participants for their time and cooperation.
Consent for publication
Written consent for publication of the clinical data of the participant maintaining confidentiality was obtained.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study was approved by the Institutional Ethics Committee, Amity Medical School, Amity University Haryana, India (Approval No. AUH/EC/D/2016/030). Prior to the enrollment in the study, written informed consent was obtained from all participants stating their acceptance to voluntarily undergo the procedures and participate in the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.