
Abstract
Purpose:
To describe a case of retinal arterial macroaneurysm associated with macular pucker with good response to subthreshold laser treatment.
Presentation:
Two-year follow-up of a patient with decreased vision in one eye for the past 6 months. Baseline best-corrected visual acuity was 20/40 in the affected eye. Multiple retinal arterial macroaneurysms were diagnosed on biomicroscopy fundus examination, with the presence of subretinal fluid and hard exudates on macula. Multimodal imaging including optical coherence tomography and fluorescein angiography confirmed the diagnosis and presence of macular pucker, which complicated the treatment choice. The largest retinal arterial macroaneurysm was treated 2 days after the diagnosis by means of subthreshold micropulse laser using an infrared diode laser with 1400 mW power, 200 ms exposure and 10% duty cycle.
Results:
Five months after the treatment, despite absorption of subretinal fluid, there were increased hard exudates at the posterior pole and best-corrected visual acuity was unchanged. Progressively, the exudates were absorbed and vision improved. Eighteen months after the treatment, best-corrected visual acuity was 20/25. Hard exudates were almost completely reabsorbed, with no evidence of fluid. Macular pucker was unchanged, with no retinal traction or complications related to conventional laser treatment.
Conclusion:
Subthreshold laser treatment could be the treatment of choice in complicated cases of retinal arterial macroaneurysm with macular pucker, as it is able to modify the vessel permeability, without any thermal negative effect.
Introduction
Retinal arterial macroaneurysm (RAM) is acquired, focal dilation of retinal arterial vessels that can present with haemorrhagic or exudative manifestations. RAM is often found in the temporal retina, mostly at the level of second-order retinal arterioles and can be associated with capillary telangiectasias, vascular remodelling and retinal oedema. 1 RAM can also occur secondary to a branch retinal vein occlusion, diabetic retinopathy, radiation retinopathy and retinal arteritis. Vision loss can occur from macular oedema and hard exudate deposition, end-arteriole occlusion by thrombosis, or haemorrhage due to rupture of the aneurysm.2–4 Treatment of RAM is controversial and it is especially indicated for symptomatic forms.
We present a case of RAM associated with macular pucker (MP) with good response to subthreshold laser treatment (STLT).
Case report
A 50-year-old male presented in our department complaining of vision loss in the right eye for the past 6 months. Medical history revealed an episode of serous neurosensory detachment in the right eye 4 years ago, with complete and spontaneous functional recovery. Best-corrected visual acuity (BCVA) at baseline examination was 20/40 in the right eye and 20/20 in the left eye. Biomicroscopic fundus examination disclosed several RAMs especially located along the course of the inferotemporal artery with subretinal fluid (SRF) and hard exudate macular deposition, in association with MP (Grade 1). 5 Fundus autofluorescence (FAF) showed large area of hyperfluorescence corresponding to SRF, whereas hard exudates were seen as a large hypofluorescence ring. Fluorescein angiography (FA) confirmed the presence of multiple RAMs along the inferotemporal arcade, showing dye leakage (Figure 1). Optical coherence tomography (OCT) showed a large neurosensory detachment involving the fovea and identified hard exudates in outer nuclear and plexiform layer as well as intraretinal cysts, confirming the coexistence of MP (Figure 2). Left eye examination was insignificant.
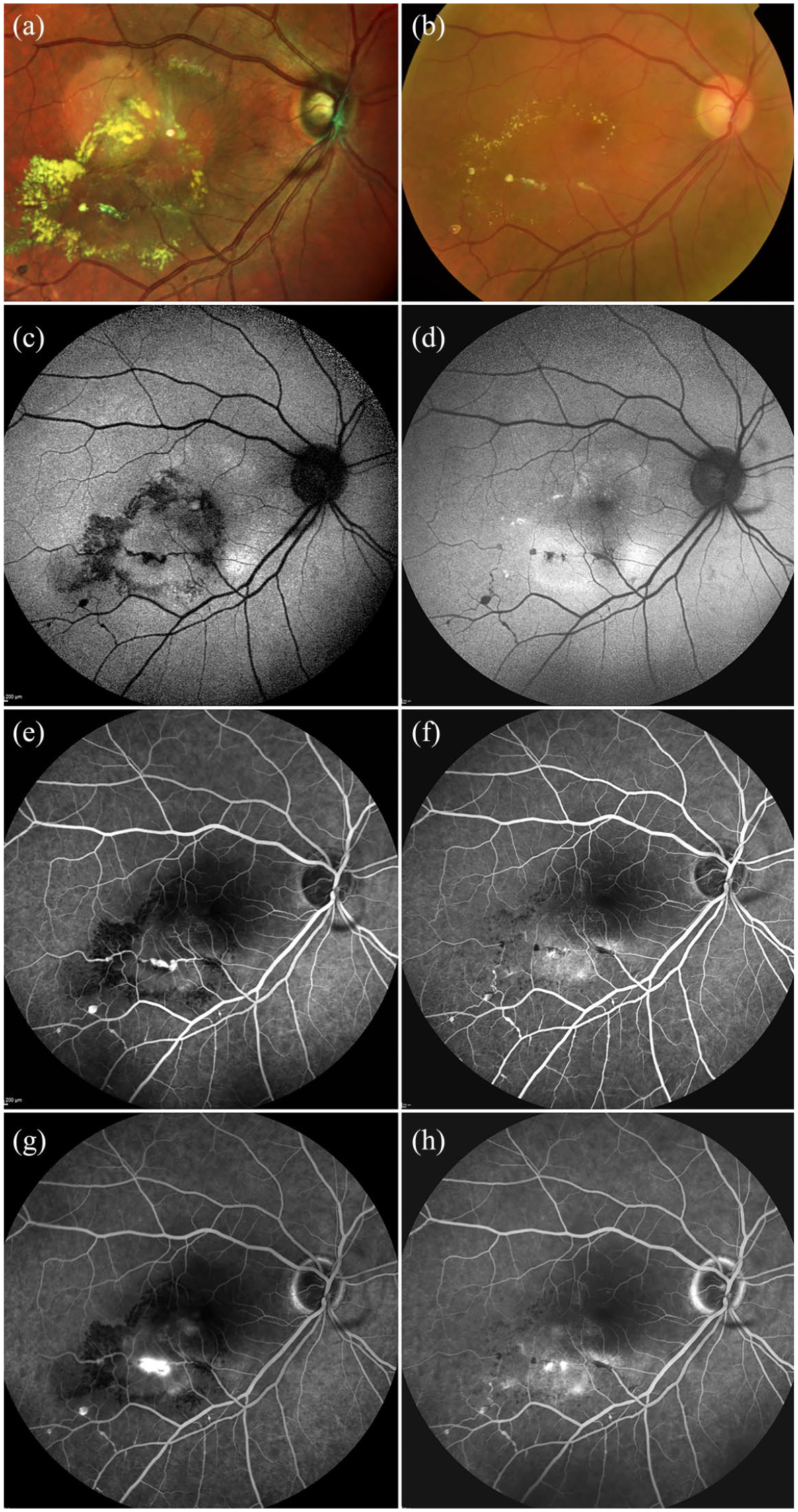
Retinal multimodal imaging at baseline and last follow-up post subthreshold laser treatment (STLT). Colour fundoscopy: at baseline, general dilation of vascular arch is associated with the presence of aneurysm in small and large arterial vessels on inferior temporal arcade. (a) Presence of marked macular pucker, large subretinal fluid (SRF) and a circinate ring pattern of hard exudates in posterior pole. (b) 18 months post STLT, hard exudates have almost disappeared, and no SRF is present. (c) Fundus autofluorescence (FAF): at baseline, large area of hyperfluorescence corresponding to SRF, hard exudates are seen as a large hypofluorescence ring. (d) At last follow-up, no evidence of fluid or hard exudates is seen. (e, g) Fluorescein angiography (FA): early and late phases: at baseline, multiple vascular aneurysms are present in inferior temporal arcade without signs of vasculitis, showing dye leakage in late phase. (f, h) At last follow-up, arterial macroaneurysm remodelling is observed without any signs of leakage in late phase.
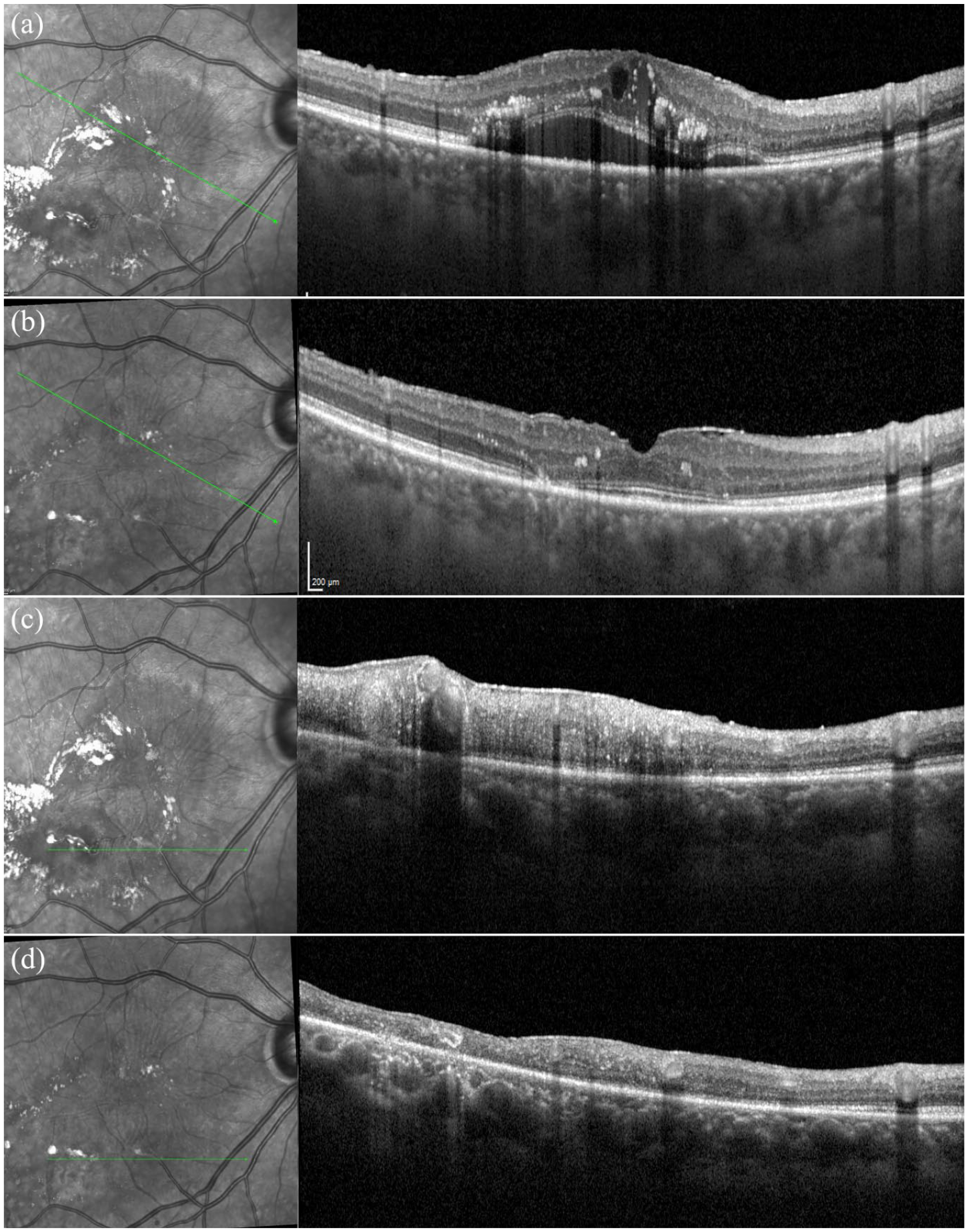
Optical coherence tomography (OCT) at baseline and 18 months post STLT. (a, c) At baseline OCT, there are large neurosensory detachment involving the fovea, presence of hard exudates in outer nuclear and plexiform layer and some intraretinal cysts and the coexistence of macular pucker. (b, d) At last follow-up, subretinal fluid and retinal cyst are absent. Limited loss of outer nuclear layer and ellipsoid zone close to the fovea is observed.
The patient underwent subthreshold micropulse laser treatment addressed to the largest RAM 2 days after the diagnosis. STLT was performed using an infrared diode laser (Iris Medical Oculight, SLx Photocoagulator, Iridex Corp, Mountain View, CA). The laser parameters used were 125 mm laser spot diameter, 200 ms exposure and 10% duty cycle. The laser power was set at 1400 mW, with confluent spots directed on the RAM and the surrounding retina. 4
Five months after the treatment, SRF was reabsorbed, but there was an increased hard exudate deposition at the posterior pole. BCVA was unchanged. The patient was regularly re-examined every 4 months. Over the follow-up period, there was a progressive reabsorption of the hard exudates with a BCVA improvement. Eighteen months after the treatment, BCVA was 20/25. Hard exudates were almost completely reabsorbed, with no evidence of fluid. FA revealed an RAM vessel remodelling with no dye leakage (Figure 1). Limited loss of outer nuclear layer and ellipsoid zone close to the fovea were visible on OCT (Figure 2). No laser scar was visible. It is noteworthy that the MP turned out to be unchanged, with no effects of the subthreshold laser application.
The consent to share and publish these findings and images has been gathered from the patient.
Discussion
RAM treatment is controversial with no general consensus about the best management.3,4 Although in many cases spontaneous resorption may occur, progressive photoreceptor damage may follow the long persistence of blood or SRF, with irreversible visual impairment.6,7
In our case report, we describe a more complex form of RAM associated with MP, probably due to the long-standing exudation secondary to RAM. Aim of treatment was the RAM remodelling, promoting the SRF and hard exudates reabsorption, without exacerbating the macular traction due to MP. Conventional laser treatment could have not been considered an appropriate choice as it might have aggravated MP and retinal traction due to thermal effects.7,8 In addition, vascular occlusion, arteriovenous shunts, enlargement of laser scar, choroidal neovascularization and subretinal fibrosis could have been further complications, related to conventional laser treatment.7–10
Anti-vascular endothelial growth factor (VEGF)-based approach has been proposed for RAM with significant results in literature, as it acts by decreasing vascular permeability and blocking angiogenesis, leading to reduce bleeding and exudation. But in this specific case, the rapid vascular effects on RAM could lead to an exacerbation of macular traction, with potential visual function deterioration. In addition, it has been demonstrated that in complicated RAM cases with recurrence of cystoids macular oedema (CME) after a series of VEGF injections, ultimately focal laser photocoagulation was needed for stabilization of vision. 9
In an attempt to achieve a vision improvement minimizing the adverse effects of treatment, we decided to treat the patient with STLT. The results were positive, with RAM remodelling, fluid and exudates reabsorption and visual acuity improvement, without any negative side effects.7,8 Mechanisms of action of STLT are not completely known, but they involve the release of cytokines which are able to modify the vessel permeability, without any thermal negative effect.
In conclusion, STLT can be an effective treatment for RAM associated with MP. Further studies are warranted to confirm our preliminary data.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.B.P. and F.B. confirm they are, respectively, an associate editor and the editor in chief of this journal and were not involved in the peer review process of this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.