
Abstract
Purpose:
To report the morphological and clinical features of a case of pachychoroid disease with focal choroidal excavation and large choroidal excavation complicated by choroidal neovascularization.
Methods:
The patient underwent a complete ophthalmologic examination including best-corrected visual acuity assessment, anterior segment and dilated fundus examination, fluorescein and indocyanine green angiography, and spectral-domain optical coherence tomography.
Results:
During the previous follow-up, the 57-year-old man received a diagnosis of central serous chorioretinopathy in the right eye with a late appearance of a choroidal neovascularization. The best-corrected visual acuity was 20/125 and 20/20 in the right and left eye, respectively. Dilated fundus examination, fluorescein angiography, and indocyanine green angiography confirmed a large subretinal fibrosis corresponding to the evolution of the choroidal neovascularization in the right eye. Spectral-domain optical coherence tomography clearly demonstrated in the right eye a large choroidal excavation below the fibrotic neovascular lesion with multiple hyperreflective foci inside the cavity, and in the left eye, a conforming focal choroidal excavation, bowl-shape type, associated with increased choroidal thickness with pachyvessels.
Conclusion:
Large choroidal excavation has been rarely reported. Although the pathogenetic mechanisms leading to the formation of large choroidal excavation are still only hypotheses, a combination of primary degenerative inflammatory factors sustaining the focal choroidal excavation formation and disruptive process of the choroidal neovascularization could be retained responsible for the large choroidal excavation.
Introduction
Pachychoroid disease is composed by a wide spectrum of clinical pictures including central serous chorioretinopathy (CSC), pachychoroid pigment epitheliopathy, pachychoroid neovasculopathy, polypoidal choroidal vasculopathy, or more recently defined aneurysmal type 1 neovascularization, focal choroidal excavation (FCE), and peripapillary pachychoroid syndrome.1,2 These manifestations share common morphological features characterized by focal or diffuse increase in choroidal thickness involving primarily the choroidal vessels in Haller’s layer, by a thinning of the choriocapillaris and Sattler’s layer, and by changes of retinal pigment epithelium (RPE) adjacent to the choroidal anomalies.
Here, we described a case with pachychoroid disease with FCE and large choroidal excavation (LCE) complicated by choroidal neovascularization (CNV).
Case report
A 57-year-old man with history of a previous single episode of neurosensory detachment in the right eye (RE) and later complicated by appearance of CNV underwent to a complete clinical examination by our Ophthalmology centre.
Clinical history confirmed the previous diagnosis of CSC in the RE occurring in 2013. During the follow-up, the patient did not receive any treatment and he was managed conservatively with simple observation. In an unspecified period of the follow-up, the patient developed a CNV which was unnoticed due to reduced visual acuity secondary to CSC, and no treatment was suggested for lack of CNV activity.
The ophthalmic examination disclosed a best-corrected visual acuity (BCVA) of 20/125 with metamorphopsia in the RE and 20/20 in the left eye (LE) and an emmetropic state. Anterior segment examination was unremarkable. Dilated fundus examination revealed a large subretinal fibrosis in the posterior pole and occupying the whole macula area in the RE and few scattered pigmentary changes resembling drusen combined with reduced fundus tessellation in both eyes.
Fluorescein angiography (FA) of the RE displayed a hypo-fluorescence at the early frames and hyper-fluorescence at late frames corresponding to the evolution of the CNV in the stage of the submacular fibrosis, whereas in the LE, an area of irregular hyper/hypo-fluorescence corresponding to the RPE changes was demonstrated.
Indocyanine green angiography revealed multiple areas of choroidal hyperpermeability in both eyes. In addition, in the RE, a progressive hyperfluorescent staining of the entire fibrous lesion with no late leakage was observed. In the LE, an early hypofluorescence could be observed in the site of FCE with an irregular hyperfluorescence around the FCE in the late phase.
Spectral-domain optical coherence tomography clearly demonstrated in the RE the presence of a large well-defined hyper-reflective subretinal fibrotic CNV with an overlying retinal disorganization and atrophy and an intralesional cavitation (Figure 1(a)). Multiple cystic area could be observed in the inner retina associated with outer retinal tubulation (ORT) localized temporally to the fovea. Of note, a LCE was clearly observed below the most central area of the fibrotic neovascular lesion with multiple hyperreflective foci inside the cavity. In this site, the normal choroidal anatomy was no longer detectable with the lack of the choriocapillaris, the Sattler’s and Haller’s layers. An increased choroidal thickness with dilated choroidal vessels or pachyvessels were easily recognizable outside the area of the LCE. In the LE, a conforming FCE, bowl-shape type, juxtafoveally localized was demonstrated (Figure 1(b)). Also in the LE, an increased choroidal thickness with pachyvessels were detectable outside the FCE with a choroidal thinning with highly reflective choroidal tissue and a poor defined choroidal-scleral junction beneath the area of the FCE.
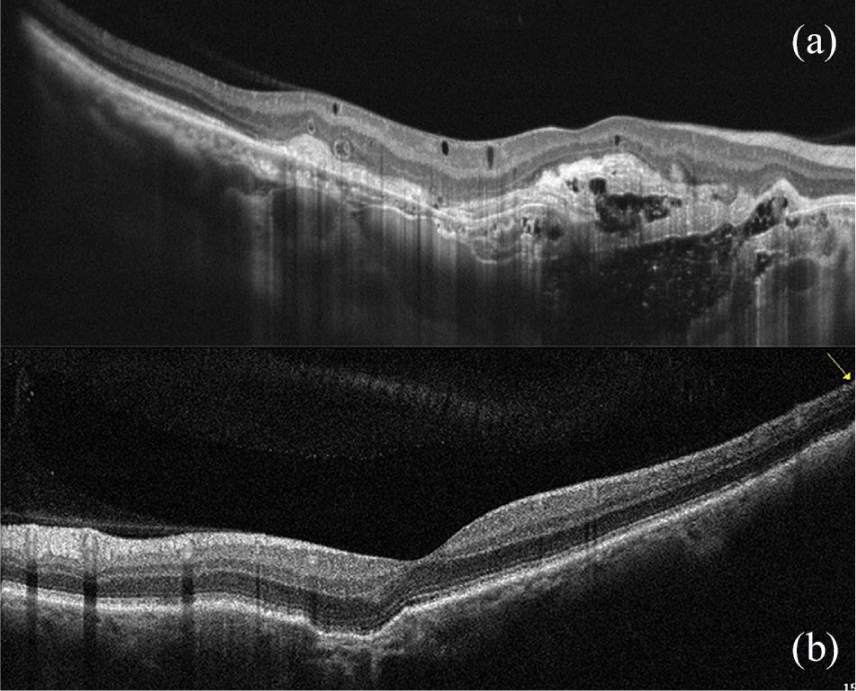
(a) SD-OCT shows in the right eye the presence of a large well-defined hyper-reflective subretinal fibrotic choroidal neovascularization with an overlying retinal disorganization and atrophy. Multiple cystic area can be observed in the inner retina associated with outer retinal tubulation. A large choroidal excavation is clearly observed below the fovea with multiple hyperreflective foci inside the cavity. (b) In the left eye, a conforming focal choroidal excavation, bowl-shape type, juxtafoveally localized, is clearly evident.
Discussion
The association of FCE with pachychoroid spectrum disorders has been widely characterized, and the prevalence of the FCE with CSC is estimated in a range of 1.2%–7.8% of cases.3,4 Differently, LCE combined with pachychoroid spectrum disorders is a novelty finding. In general, LCE is a rare entity and it has been described in association with rubella retinopathy complicated by CNV, combined with toxoplasmosis and North Carolina macular dystrophy.5–7
Pathogenesis is not clearly understood and can be the object of hypotheses. A structural choroidal weakening may represent a predisposing factor elicitated by the CNV development. In particular, CNV contraction over the follow-up may further contribute to the anatomical changes. We could suggest a late evolution of the FCE which in a longer time could extend into deeper planes and on a wider surface. It is could the evolution of a FCE complicated by CNV; in this case, a combination of primary degenerative inflammatory factors sustaining the FCE formation and related to pachychoroid, as suggested by Chung et al., 2 associated with a disruptive process of the CNV may lead to atrophy of the deep choroidal stroma. Although the photodynamic therapy (PDT) with verteporfin was not used in this case, we want to quote the PDT as an additional causative factor in the process of LCE evolution as suggested by Parodi et al. 5 Finally, we evidence that an another morphological characteristic, the ORT, frequently described with CNVs associated with age-related macular degeneration and in one case of fibrous metaplasia in CSC, is now described also in association of CNV complicating a clinical picture of CSC-pachychoroid disease. 8
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research for this paper was financially supported by Italian Ministry of Health and Fondazione Roma.