
Abstract
Purpose:
To evaluate the efficacy and the safety of curcumin-phosphatidylcholine complex in children affected by juvenile idiopathic arthritis–associated uveitis as an adjunctive treatment to chronic systemic immunosuppressive therapy.
Methods:
In this retrospective, longitudinal study, we treated patients affected by juvenile idiopathic arthritis–associated uveitis with residual low-grade inflammatory activity in the anterior chamber with one tablet of curcumin-phosphatidylcholine complex per day, over a year. Low-grade inflammatory activity was characterized by flare 1+ at slit-lamp examination and 10–50 photon counts per ms) at the FC500 laser flare meter. Inactivity of uveitis was defined as complete disappearance of flare at the slit-lamp examination and values <10 ph/ms at laser flare meter. Conversely, recurrence of the uveitis was defined as a one-step increase from baseline in anterior chamber cells levels or laser flare meter measurements >50 ph/ms.
Results:
A total of 22 out of 27 patients (81%) achieved inactivity at the end of the study. Five patients (19%) did not show a significant reduction in anterior chamber flare, remaining stable throughout the follow-up. Only three episodes of flare-ups in three different patients were recorded. Overall, the treatment was well tolerated by all patients and no ocular discomfort, ocular side effects, or allergic reactions were registered.
Conclusion:
Adjunctive therapy with curcumin in patients affected by juvenile idiopathic arthritis–associated uveitis improves mild chronic anterior chamber flare and presents a good safety profile. Despite being mild, anterior chamber inflammation should be minimized to avoid the development of sight-threatening complications in these patients.
Keywords
Introduction
Juvenile idiopathic arthritis (JIA) is a disease entity that includes a number of arthritides of unknown etiology that begins before 16 years of age and persists for at least 6 weeks. 1 Children with JIA are at risk for developing chronic ocular inflammation and JIA accounts for approximately 75% of all pediatric anterior uveitis cases. 2
Uveitis associated with JIA is typically insidious and presents with severe asymptomatic chronic anterior inflammation. About 50%–75% of children with severe JIA-associated uveitis develop visual impairment secondary to ocular complications, such as cataract, glaucoma, band keratopathy, and macular pathology.2,3
Prompt and aggressive treatment with systemic immunosuppressive agents is often required to improve the long-term visual prognosis and reduce the risk of ocular events. Local and systemic corticosteroids are the mainstay of therapy in the acute phase of inflammation; however, long-term corticosteroid-sparing agents should be considered in cases of chronic and severe disease. 4
Steroid-sparing agents in the treatment of JIA-associated uveitis include disease modifying anti-rheumatic drugs (DMARDs) such as methotrexate and azathioprine, and biologic agents in refractory cases. Tumor necrosis factor (TNF)-alpha blockers (adalimumab and infliximab) are the most commonly used biologic agents in JIA-associated uveitis, and these agents have markedly improved the visual prognosis of the disease.5,6 However, some patients fail to respond to different immunomodulators, including conventional agents and the more potent biologics, or they are intolerant to these therapies. In this subset of patients, signs of chronic low-grade inflammation and flare in the anterior chamber may persist despite aggressive systemic immunosuppressive therapy.
Curcumin is a natural pigment extracted from Curcuma longa rhizomes. In the last few years, several in vitro and in vivo studies have confirmed its anti-inflammatory, antioxidant, antimicrobial, and anti-tumorigenic properties. Indeed, curcumin acts with a pleiotropic mechanism to target cellular and molecular signaling pathways involved in the inflammatory response, including downregulation of apoptotic cascade, inhibition of free radical production, and blockage of the cyclooxygenase enzymatic activity.7 –10 Recently, the beneficial effects of curcumin-based products have been reported in different ocular inflammatory conditions, such as chronic anterior uveitis, glaucoma, dry eye disease, diabetic retinopathy, and age-related macular degeneration.11 –18
While the current literature refers to an adult population only, little-to-no data exist about pediatric patients. Based on the good systemic tolerability and safety reported in the current literature, there is reasonable support to the potential role of curcumin in the treatment of chronic uveitis in children. The aim of this study is to evaluate the efficacy and the safety of the adjunctive treatment with curcumin-phosphatidylcholine complex tablets in children affected by JIA-associated uveitis.
Patients and methods
This was a retrospective, longitudinal study of consecutive patients affected by JIA-associated uveitis followed at the Uveitis Service, Department of Ophthalmology, San Raffaele Scientific Institute in collaboration with the Pediatric Rheumatology Unit at the “Istituto Ortopedico G. Pini,” Milan, Italy, between January 2018 and January 2019. The study was conducted in agreement with the Declaration of Helsinki for research involving human subjects and was approved by the institutional review board (IRB) of both hospitals. The patients’ parents (if the child was younger than 18 years old) or the patient himself signed an informed consent to participate in the study.
Inclusion criteria were: (1) age older than 3 years old, (2) diagnosis of JIA according to the International League of Associations of Rheumatology (ILAR) classification system, 19 (3) diagnosis of JIA-associated anterior uveitis according to standardized uveitis nomenclature (SUN) criteria, 20 (4) well-controlled arthritis with current immunosuppressive therapy for at least 6 months, and (5) low-grade inflammatory activity in the anterior chamber characterized by flare 1+ at slit-lamp examination and 10–50 ph/ms (photon counts per ms) with the FC500 laser flare meter (LFM) (Kowa Co. Ltd, Tokyo, Japan). 21
Exclusion criteria were: (1) poorly-controlled uveitis (flare ⩾2+) at baseline or in the previous 3 months; (2) ⩾1+ cells in the anterior chamber at baseline; (3) treatment with systemic, intraocular, periocular, or topical corticosteroids at the time of inclusion in the study; (4) significant corneal opacities hindering the anterior chamber examination; (5) extensive posterior synechia or mature cataract impeding the semi-automated measurement of flare; (6) allergy or intolerance to any of the pharmaceutical components; and (7) intraocular surgery (including cataract extraction, glaucoma surgery, or vitrectomy) within the 3 months prior to inclusion in the study.
At baseline, all the patients were prescribed with NORFLO® tablets (Eyepharma Co, Italy) 1 tablet/day, each containing a mixture of highly bioavailable curcuminoids, complexed as iphytoone®, with a minimum of 2% phosphatidylserine. The treatment was continued for 12 months, in addition to each patient’s systemic immunosuppressive therapy.
All the participants underwent a complete ophthalmological examination at baseline and at each follow-up visit, including best-corrected visual acuity (BCVA) assessment on standard ETDRS letters or “tumbling E” charts, slit-lamp biomicroscopy, measurement of intraocular pressure (IOP) with eye care tonometer, and dilated fundus evaluation. Anterior segment inflammation was graded clinically by means of slit-lamp cells and flare quantification according to the SUN criteria 20 and semi-automated flare measurement with the Kowa FC500 laser flare meter (LFM). Seven measurements were obtained before the pupil was subjected to pharmacological dilation: the highest and lowest values were automatically discarded and the mean of the remaining five readings was calculated. All the measurements were performed by an expert pediatric uveitis specialist (E.M.).
Rheumatologic assessment, including history collection and physical examination, was performed on the same day of each ophthalmologic visit (M.G.); patients were classified as affected from persistent-type or extended-type JIA according to the ILAR criteria 19 and systemic treatment with DMARDs and/or biologic drugs was registered. Clinical parameters evaluated were age, gender, age at the onset of arthritis and uveitis, characteristics and complications of the uveitis, and current systemic therapies. Patient data were reviewed at 1, 3, 6, 9, and 12 months. Inactivity of uveitis was defined as complete disappearance of flare at the slit-lamp examination and values were < 10 ph/ms at LFM.22 –24 Conversely, recurrence of the uveitis was defined as a one-step increase from baseline in SUN cell activity score (AC cells) or LFM flare measurements of > 50 ph/ms.
Primary outcome measure was the efficacy of the supplementation with NORFLO added to the current systemic therapy in reducing the anterior chamber flare level; the efficacy of treatment was defined by complete inactivity of the anterior uveitis and reduction of the flare to < 10 ph/ms using LFM at 12 months. Secondary outcomes were the safety and the tolerance of the therapy and patient’s compliance. To avoid measurement bias, in patients with bilateral condition, only one eye was used for the analysis and the other was used for baseline higher flare measurement using LFM.
Descriptive statistics for patients’ records and comparative analyses were performed through GraphPad Prism 6.0 (GraphPad Software, Inc., San Diego, CA). BCVA was converted to the logarithm of the minimum angle of resolution (LogMAR). All data were tested for normality using the D’Agostino-Pearson test. Means were presented with their standard deviation. Repeated measure analysis of variance (ANOVA) was used to highlight differences for continuous parametric variables, using Tukey’s correction for multiple comparisons; mean differences and 95% confidence intervals (CIs) for each comparison were provided. A p-value < 0.05 was considered statistically meaningful.
Results
Patients’ demographics
A total of 27 patients (21 females, 6 males) with a mean age of 17.4 ± 8.9 years (range 3–31) affected by JIA-associated uveitis were enrolled in the study. Nineteen patients had a diagnosis of oligo-extended JIA and eight of oligo-persistent JIA according to ILAR classification. Antigen nuclear antibodies (ANA) were positive in 15 patients, while rheumatoid factor and human leucocyte antigen-B27 were negative in all patients. The mean age at onset of JIA arthritis was 4.4 ± 3.4 years, while the mean age at onset of uveitis was 5.8 ± 4 years. The interval between JIA arthritis onset and first diagnosis of uveitis was 33.6 ± 50.1 months. In four patients (14.8%), the ocular inflammation preceded arthritis by a mean of 29.4 ± 28.8 months. In 22 patients, the chronic systemic treatment consisted of a non-biologic immunosuppressive drug (methotrexate) plus a biologic immunosuppressive drug. Demographic and clinical details are listed in Table 1.
Patients’ demographics, uveitis characteristics, and current systemic treatment for JIA.
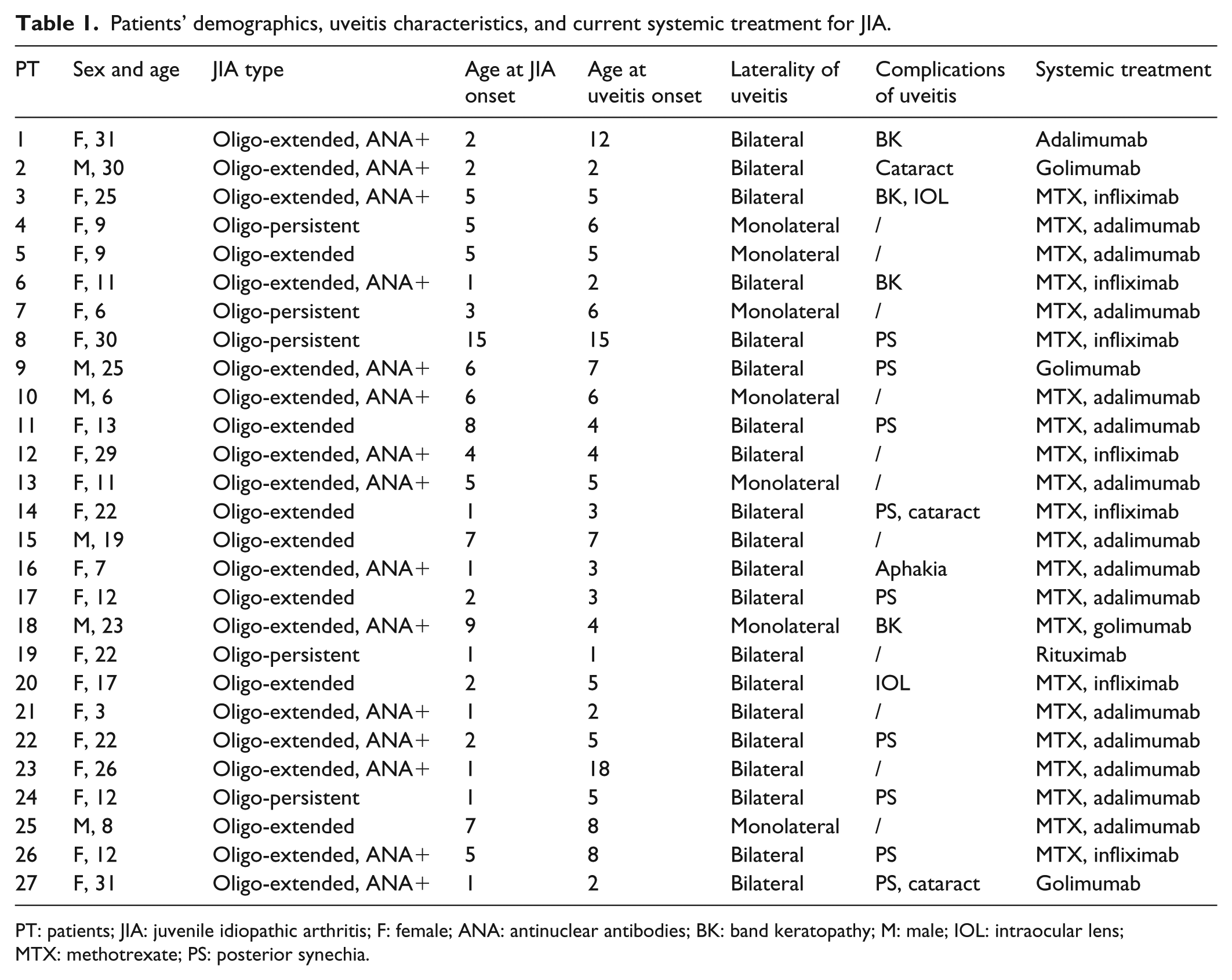
PT: patients; JIA: juvenile idiopathic arthritis; F: female; ANA: antinuclear antibodies; BK: band keratopathy; M: male; IOL: intraocular lens; MTX: methotrexate; PS: posterior synechia.
Uveitis characteristics
The uveitis was bilateral in 20 patients. Granulomatous uveitis was the most common type of inflammation being present in 18 patients, while non-granulomatous type was only seen in nine cases. All the patients presented with anterior uveitis and no signs of posterior segment inflammation were detected in our population.
Regarding ocular complications at baseline, peripheral band keratopathy was present in four patients and posterior synechia in nine patients. Three patients presented with no clinically significant cataract, two patients with a posterior chamber intraocular lens, and one was aphakic (Table 1).
Mean IOP was 14.3 ± 2.1 mmHg and no changes were recorded during the 12-month study period. Three patients were on chronic topical IOP -lowering medications.
Visual acuity
Baseline BCVA was 0.17 ± 0.3 LogMAR (20/30 Snellen equivalent), while BCVA at the end of the study was 0.18 ± 0.12 (20/30 Snellen equivalent), with no statistically significant difference (p = 0.5).
Treatment efficacy
Disease inactivity was achieved in 22 patients at the end of follow-up.
Mean baseline flare was 34.3 ± 8.8 ph/ms, which was converted to 25.7 ± 11.3 ph/ms at 1 month, 16.4 ± 12.5 ph/ms at 3 months, 15.4 ± 16.1 ph/ms at 6 months, 14.0 ± 14.7 ph/ms at 9 months, and 11.8 ± 13.1 ph/ms at the end of the treatment (p < 0.0001). The flare measures reduced rapidly in the first 3 months of treatment, then the values stabilized and continued to reduce steadily until 12 months. Figure 1 showed that four patients (14.8%) reached inactivity of the uveitis (flare meter of <10 ph/ms) at 1 month, 10 patients (37%) at 3 months, and 8 patients (29.6%) at 6 months, while 5 patients (18.6%) did not show a significant reduction in flare during the study. Three patients (11.1%) experienced a flare-up (flare ⩾2+) by the ninth-month (flare was 2 at sixth-month and 1 at ninth-month). The flare-ups were successfully treated with topical corticosteroid (1% prednisolone acetate) and in all the cases the measurement of flare was <10 ph/ms after 2 weeks of therapy. Semi-automated flare measurements of study population during the follow-up are summarized in Table 2 and illustrated in Figure 1.
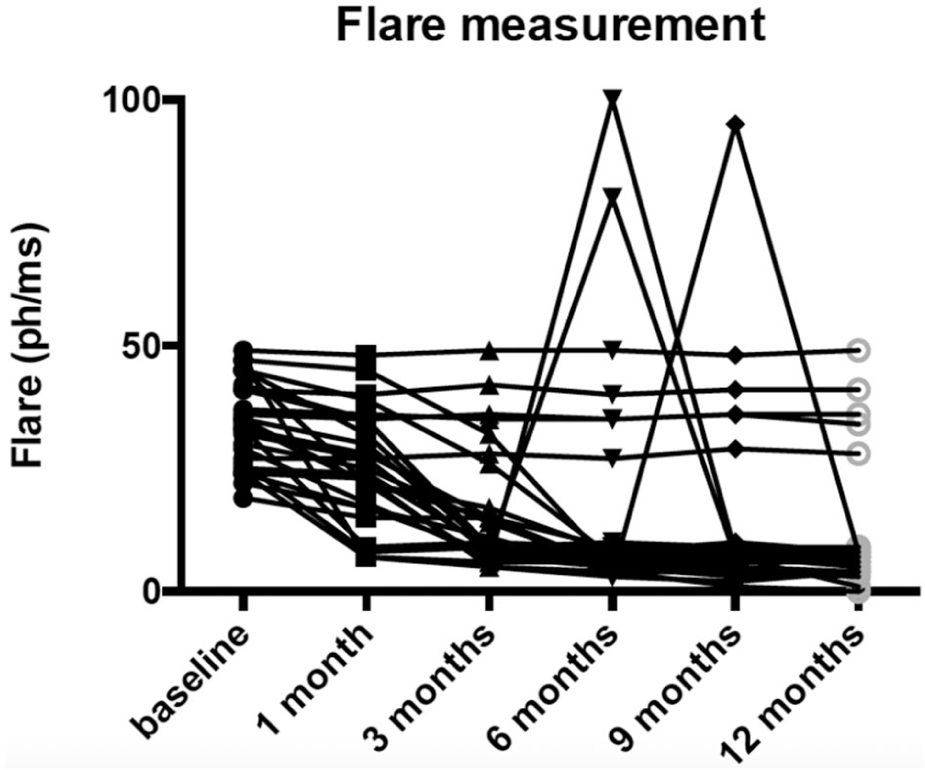
Semi-automated flare measurement of the study population throughout all the study.
Semi-automated flare measurement of the study population during the follow-up.
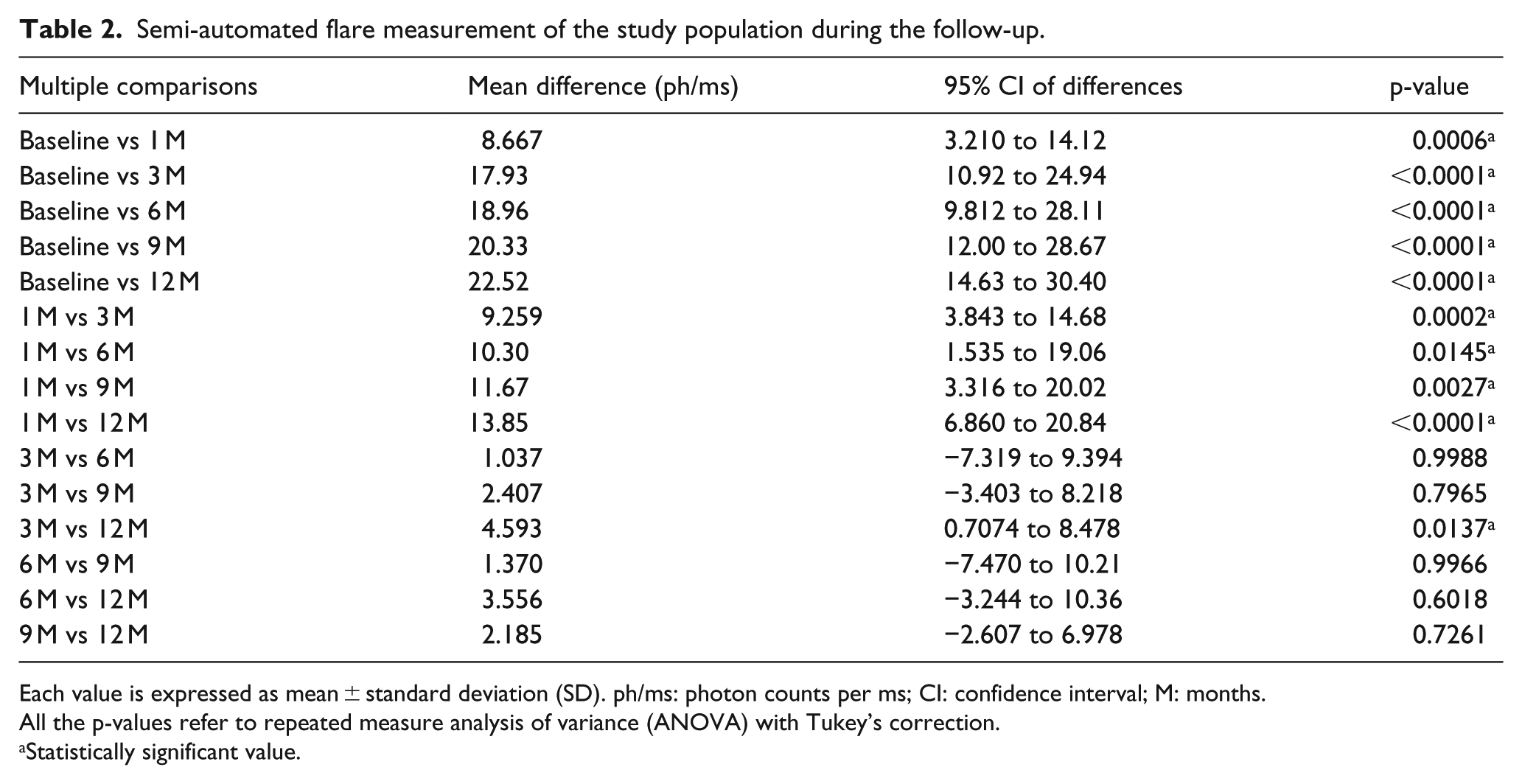
Each value is expressed as mean ± standard deviation (SD). ph/ms: photon counts per ms; CI: confidence interval; M: months.
All the p-values refer to repeated measure analysis of variance (ANOVA) with Tukey’s correction.
Statistically significant value.
The mean number of flare-up recurrence (2+ flare in anterior chamber) before starting with NORFLO treatment was three episodes per year and was reduced to one episode during the study period.
Treatment safety and tolerance
Overall the treatment was well tolerated by all patients enrolled. No ocular discomfort, ocular side effects, or allergic reactions were recorded during the study. Two patients reported mild gastrointestinal disturbances and one patient disliked the taste of the tablets. All patients were able to complete the study with NORFLO systemic treatment. None of the patients required intraocular surgery such as cataract extraction or glaucoma filtering surgery during the study.
Discussion
In this study, we evaluated the efficacy and the safety of the adjunctive treatment with NORFLO in patients affected by JIA-associated uveitis. NORFLO is a curcumin-phosphatidylcholine complex (iphytoone) with recently described anti-inflammatory properties.7 –10 Although the mechanism is yet to be fully elucidated, several studies reported the beneficial effects of curcumin in many relapsing ophthalmic diseases sustained by long-standing inflammation such as central serous chorioretinopathy, diabetic retinopathy, dry eye, and uveitis of different etiologies.11 –13,25 –29 In the present series, we reported an improvement of chronic 1+ anterior chamber flare after a 1 year course of oral therapy with NORFLO tablets. The majority of our patients (23 cases) showed reduction of flare in the anterior chamber with NORFLO treatment during the 12-months study period. Mean flare values decreased from 34.3 ± 8.8 ph/ms at baseline to 6.4 ± 12.5 ph/ms at 3 months, 15.4 ± 16.1 ph/ms at 6 months, and 11.8 ± 13.1 ph/ms at the end of the treatment (p < 0.0001).
The flare measurements reduced rapidly in the first 3 months of follow-up, then the values stabilized, but continued to reduce steadily until 12 months. The majority of our treated patients reached inactivity of uveitis after 3 months (37%) and 6 months (29%) of therapy respectively. However, five patients (18.6%) did not show a significant reduction in flare during the study and the flare grading remained unchanged compared to baseline values. We also recorded a reduction in the mean number of uveitis relapses from three episodes per year to one episode per year after the use of NORFLO adjunctive treatment.
A residual flare that remains after maximal therapy in patients with JIA-associated uveitis indicates permanent breakdown of the blood-aqueous barrier. Laser flare photometry studies have shown that flare is the most important inflammatory parameter and is highly predictive of ocular complications and visual loss in children with JIA-associated uveitis, even in the absence of aqueous cells. 30
Therefore, we decided to include only patients with no cells in the anterior chamber but low-grade flare (<50) at semi-automated measurement. None on the patients was on topical therapy for active uveitis.
The flare measurement was conducted both clinically at slit lamp by an expert uveitis specialist and objectively by means of the Kowa LFM. Studies of laser flare photometry in uveitis have demonstrated that clinically meaningful changes in flare well correspond to the clinical activity score of the anterior uveitis. We considered a range of 10–50 ph/ms of flare at Kowa laser equal to clinical grading of 1+ of flare in the anterior chamber as described in previously published studies. 21 A value of <10 ph/ms was considered no clinically significant as it is normally present in the normal population.22,23 In JIA-associated uveitis a permanent breakdown of blood-aqueous barrier could be present. Nevertheless, as stated to expert consensus, aggressive treatment should be applied to reduce the amount of flare not due to permanent blood-aqueous barrier breakdown even in the absence of inflammatory cells in the anterior chamber. 24 We hypothesize that a permanent breakdown of blood-aqueous barrier was present in those five patients with unchanged flare from baseline to final visit. In the study, we recorded only three episodes of flare-up in three different patients, mainly at 6 months (two patients) and at 9 months (one patient). These episodes were recorded at the first follow-up visit from the achievement of inactivity. After 12 months the same patients presented a quiet anterior chamber. As previously described by Allegri et al., 11 in fact, we suppose that continuous and protracted treatment with curcumin-phosphatidylcholine complex maintains good control of anterior uveitis and prevents relapses.
In addition, data obtained so far showed that oral curcumin is well tolerated and safe in humans and that the phospholipid formulation (iphytoone) enhances its bioavailability.31 –33 In accordance with these studies, we did not record any drop out due to ocular or systemic secondary effects. Overall the treatment was well tolerated by our JIA pediatric population.
We acknowledge several limitations to our study including the small number of patients, the lack of a control group, and the limited period of follow-up. We cannot obviously state if the inactivity was accomplished by NORFLO therapy or was an independent factor during the chronic anterior uveitis course. However, the high number of patients in which inactivity was achieved after 1 year of curcumin therapy let reasonably think that there might be a causative effect. Regardless of these limitations, we identified a remarkable strength in our study that was the measurement of flare with Kowa laser that gave us an objective comparison between different visits.
In conclusion, adjunctive therapy with curcumin in patients affected by JIA-associated uveitis presents a good safety profile and may improve the mild chronic anterior chamber flare. Children affected by JIA-associated uveitis are at high risk of developing ocular complications and every effort should be done to control and minimize anterior chamber inflammation.
Footnotes
Authors’ Note
This work was completed at IRCCS Ospedale San Raffaele, Vita-Salute San Raffaele University, Milan, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.