
Abstract
We report a case of successful intraocular foreign body/traumatic cataract removal and anterior segment reconstruction surgery of a patient’s eye that suffered penetrating injury 65 years earlier. Surgery was not recommended by ophthalmologists that she had earlier consulted. The patient opted for surgery to improve cosmesis due to leukocoria, but the level of regained vision exceeded expectations of both the patient and the surgeon. This case adds further evidence that the duration of occlusion time has no effect on visual potential in patients out of amblyogenic age. The ethical considerations of operating on such an eye with poor prognosis after traumatic injury are also discussed. To our knowledge, our patient has the longest reported duration (65 years) between the time of injury and successful surgery with good outcome.
Introduction
Ocular trauma is not uncommon and it is estimated that up to 55 million eye injuries occur annually worldwide. 1 A frequent consequence of ocular trauma is the formation of a traumatic cataract, 2 which is a significant cause of visual loss worldwide. 3
Cataract surgery in traumatic cataracts is usually more complex and associated with unpredictable visual outcomes. Zonular dehiscence, capsular tears, retinal breaks and detachment, choroidal rupture and optic nerve damage are just a few of potential pathologies that may accompany ocular trauma. Penetrating injury and retained intraocular foreign body may cause further severe damage and intraocular infection.
We report a case of complicated surgery performed on a patient with a complicated cataract following penetrating injury acquired 65 years prior to surgery.
Case description
A 79-year-old female presented with poor vision associated with the unsightly appearance of a white pupil in her left eye. She sustained ocular trauma to her left eye when she was 14 years old. While hiding from a friend in a small cabin, she was peeping through a keyhole when her friend had stuck a long wood stick with a sharp thorn through the keyhole and hit her eye. She was managed in a rural hospital but her vision gradually deteriorated over the course of 1 month. The vision in her left eye remained as counting fingers for the past 65 years. None of the ophthalmologists that she consulted with suggested surgery to treat the injured eye. She had no expectations for practical vision in this eye but was disturbed by the non-aesthetic appearance of the white pupil.
The visual acuity was 6/12 in her right eye and counting fingers with full light projection in her left eye. Upon examination, the right eye was normal except for a moderate cataract and dry age-related macular degeneration (AMD). She did not have a relative afferent pupillary defect. In her left eye, a focal scar was seen at the superior aspect of her cornea, with the corresponding peaking of the pupil in the same area. A dense fibrotic white cataract occupied most of the pupillary area with a small clear area at the centre of the lens. The anterior chamber was deep and quiet (Figure 1(a)), the intraocular pressure was normal and B-scan ultrasound of the posterior segment was unremarkable.
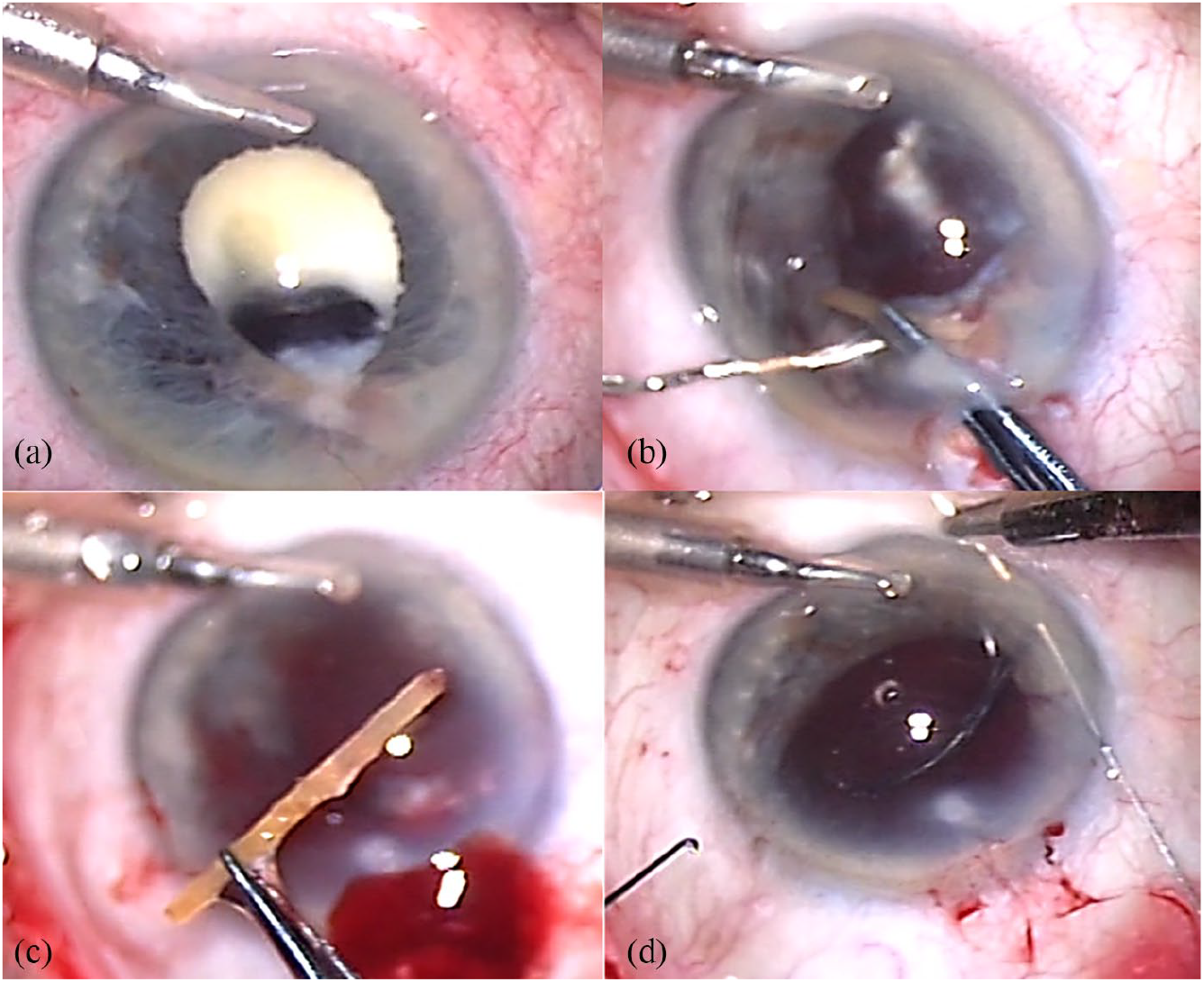
Intraoperative photos – surgeon’s view. (a) A dense, fibrotic and calcified mature cataract with a central clear area. The superior pupil is deformed with posterior synechia under a localized corneal scar, at the area of the penetrating wound. (b) After cataract removal, a yellowish thin material embedded within the fibrotic tissue uveal is exposed. (c) A foreign material, 9.8 mm long, was removed from within the eye, most likely the wooden thorn which penetrated the eye 64 years earlier. (d) A three-piece IOL is positioned in the ciliary sulcus and sutured to the iris.
Since damage to the left eye appeared limited to the traumatic cataract and the patient was upset with the cosmetic appearance of the white pupil, we discussed the option of cataract surgery in this eye, mainly for cosmetic purpose. Details of the surgery, including guarded visual potential, and possible complications such as sympathetic ophthalmia, potential double vision and visual discomfort were highlighted during the informed consent process. Nevertheless, she was enthusiastic to have surgical intervention in her left eye to improve cosmesis.
During surgery, the anterior lens capsule was stained with trypan blue and a small, about 2-mm capsulectomy was performed. Soemerring’s ring–like material was chopped and the calcified pieces were dislocated into the anterior chamber and removed using phacoemulsification. A localized firm adhesion between the superior iris and the underlying lens material was evident. After dissection and peeling of the fibrotic membrane, a yellowish hard material was gradually exposed through a combination of bimanual dissection, iridectomy and anterior vitrectomy (Figure 1(b)). A yellow foreign body was found embedded within the iris–lens material complex. Finally, the hard material was released and removed from the eye. To our surprise, a thin and long (9.8-mm) foreign body was revealed, most probably the wooden thorn that penetrated her eye 65 years earlier (Figure 1(c)).
Even though achieving useful vision did not seem realistic, we decided to perform a complete restoration of the anterior chamber. Anterior vitrectomy was done leaving a partial anterior capsular rim and to remove bleeding from the ciliary body during removal of the foreign body.
With the following biometric readings: axial length of 24.57 mm (23.83 mm on the right eye), keratometry 42.0/46.9 (41.5/43.3 on the right eye) and intraocular lens (IOL) power calculation using both the SRK/T and Barrett Universal II formulae, a three-piece IOL (model: MA60AC; Alcon) of +17.0 dioptres was chosen, accounting for a slight anterior position of the IOL with iris fixation. Sulcus implantation with iris fixation using a 10-0 polypropylene suture (W1713; Ethicon) (Figure 1(d)) was chosen as iris repair and pupilloplasty had to be performed. We felt that although the remnant lens capsule would provide sufficient support for the IOL, iris fixation would prevent rotation of the IOL in addition to further supporting the IOL. A significant improvement in vision was noted within hours. At 1 month, her corrected visual acuity was 6/15 and at 1 year 6/7.5 (refraction: +2.00 –2.75 × 5). She subsequently underwent cataract surgery of her right eye, but because of underlying AMD that was more advanced in the right eye the vision in this eye did not exceed 6/12. The eye that was blind for 65 years ended up as her better eye (Figure 2).
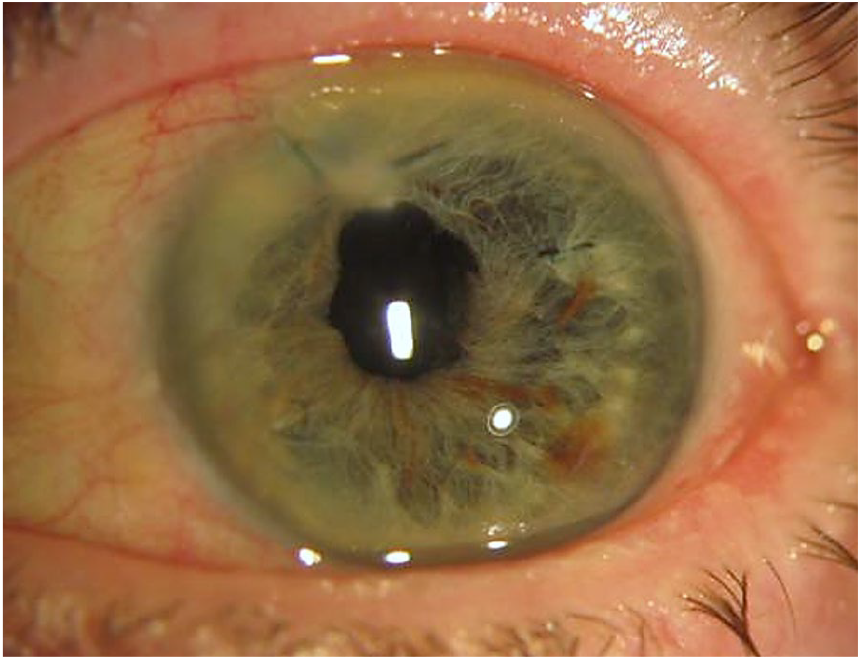
At 1 year postoperatively, the pupil is irregular but central and IOL is suture-fixated to the iris. Corrected visual acuity is 6/7.5.
Discussion
Meticulous pre-operative assessment and planning is required prior to surgery for traumatic cataracts. Nevertheless, oftentimes it is impossible to predict intraoperative surprises. Problems such as difficulty obtaining accurate biometry readings, pre-existing anterior and posterior capsular tears, compromised zonular support, vitreous in the anterior chamber and the lack of capsular support for IOL implantation should be anticipated and managed appropriately. Our patient had tears in both the anterior and the posterior capsule, vitreous in the anterior chamber, lack of proper support for IOL implantation and also an occult foreign body that was discovered intra-operatively. A computed tomography (CT) scan of the orbits would provide clues on the health of the posterior segment and help detect any occult foreign bodies. However, an orbital CT scan may still miss detection of our patient’s ocular foreign body given its non-metallic nature. Ultrasound biomicroscopy (UBM) is an alternative imaging method that has been shown to be helpful and even superior to CT scans in the detection of small, non-metallic foreign bodies in the anterior segment. 4 Some surgeons may opt to examine the fundus on-table via binocular indirect ophthalmoscopy prior to IOL implantation. Based on the patient-reported mechanism of injury and examination, we did not suspect any intraocular foreign body.
The predictors of visual prognosis in traumatic cataracts include presenting visual acuity, type of injury (open vs closed globe), wound location and method of cataract removal5,6 and IOL implantation. 6 Timing of cataract surgery and IOL implant did not affect visual outcome in adults, but was significantly associated with poorer visual outcomes for paediatric patients within the amblyogenic age group. 7 A final visual acuity of 6/18 or better after cataract surgery for traumatic cataracts was reported to be attained in between 38.5% and 55.7% of eyes.8,9 The Ocular Trauma Score (OTS) is an important prognosticating tool in ocular trauma and is useful as a guideline for informed treatment decisions. 10 Our patient was however unable to report her initial visual acuity post-injury which limited our ability to calculate her OTS.
Given that our patient had full light projection and no relative afferent pupil defect in this eye, there was potential for visual improvement despite the main objective of the surgery being to improve cosmesis. Nevertheless, the ethical considerations when operating on an eye with guarded visual prognosis due to traumatic injury need to be considered by the surgeon, 11 with proper informed consent being obtained. The surgeon should be guided by the principles of patient autonomy, beneficence and non-maleficence. The risk of sympathetic ophthalmia, with potential harm to the contralateral eye, needs to be highlighted to the patient. Less invasive options to correct leukocoria such as coloured contact lenses and corneal tattooing need to be put forward to the patient for consideration.
To our knowledge, our patient has the longest reported duration (65 years) between the time of injury and successful surgery with good outcome. The previously reported longest duration was 40 years for traumatic cataract surgery. 12 We reviewed our records and found two more cases of long-standing traumatic cataract that were operated at 35 and 55 years after the initial traumatic insult. In one case, after complicated retinal surgery, vision did not improve significantly and, in the second case, bullous keratopathy developed and limited visual recovery.
Our case adds further evidence that the duration of occlusion time has no effect on visual potential in patients out of amblyogenic age and full vision can be restored even after decades of blindness. Our patient had given up on good vision in her eye post-trauma, but, as informed physicians, we should not give up and ‘never say never’.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: E.I.A. is a consultant for Hanita Lenses, Biotechnology General, Vision Care Technologies, APX Ophthalmology, IOPtima, VisiDome and CorNeat. There are no conflict of interests related to the content of ths article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the information and images to be submitted.