
Abstract
Purpose:
Persistence represents the major reason for failure of primary macular hole repair. A variety of surgical approaches are available for treating persistent macular holes. To compare clinical outcome of re-pars plana vitrectomy combined with autologous platelet concentrate and sulfur hexafluoride 20% gas tamponade with heavy silicone oil in persistent macular hole.
Methods:
Records of 48 consecutive eyes with persistent macular holes which underwent re-pars plana vitrectomy with either heavy silicone oil (35 eyes, persistent macular–hole minimum linear diameter: 518.8 ± 171.1 µm) or autologous platelet concentrate and sulfur hexafluoride 20% (13 eyes, persistent macular hole–minimum linear diameter: 454.1 ± 211.3 µm) were reviewed retrospectively. All patients underwent measurements of anatomical persistent macular hole characteristics evaluated by optical coherence tomography and visual function. Cases in which anatomical success failed after first re-pars plana vitrectomy were treated with the other surgical techniques, comparable to a cross-over design.
Results:
Persistent macular hole closure rate was 57.1% with autologous platelet concentrate and sulfur hexafluoride 20% and 45.7% with heavy silicone oil (p = 0.102). Functional results were comparable when persistent macular hole closure was achieved (p ⩾ 0.741), but significantly better for the autologous platelet concentrate with sulfur hexafluoride 20% group when persistent macular hole closure failed (p = 0.019).
Conclusion:
Re-pars plana vitrectomy combined with autologous platelet concentrate and sulfur hexafluoride 20% seems to achieve at least non-inferior persistent macular hole closure rates and comparable functional results when compared to heavy silicone oil, suggesting autologous platelet concentrate and sulfur hexafluoride 20% as a safe surgical alternative in persistent macular hole. Especially when persistent macular hole closure failed, autologous platelet concentrate with sulfur hexafluoride 20% seems to be superior regarding visual outcome.
Keywords
Introduction
A macular hole (MH) is a full-thickness anatomic defect of the retinal tissue, involving all neural retinal layers in the fovea. The primary or so-called idiopathic macular hole (IMH) represents the most frequent entity with approximately 90%. 1 Pars plana vitrectomy (PPV) with internal limiting membrane (ILM) peeling and gas endotamponade is currently regarded as the gold standard in MH surgery,2,3 and closure rates are reported to be up to 85%‒90%.1,3–7
Despite improvement in surgical techniques, primary failure rates were described to be at 5%‒20%.1,8–13 Different factors were identified as predictive for successful outcome in IMH surgery including anatomical characteristics, such as smaller diameter of MH,1,14–16 earlier stage or better preoperative visual acuity, intraoperative parameters including the area of peeled ILM, or postoperative face-down positioning.1,7,8,17,18
The mechanism behind failure, including persistence or reopening of MHs, remains poorly understood. Some have attributed it to residual epiretinal membrane traction or poor patient compliance with face-down positioning.5,6 Various surgical strategies exist for the treatment of persistent macular holes (PMHs), including re-vitrectomy with heavy silicone oil (HSO) tamponade, enlargement of ILM peeling with autologous ILM transplantation, autologous platelet concentrate (APC) or whole blood, and gas endotamponade.5,19 These different surgical techniques incorporate distinct implications for the patient, as the need for reoperation in silicone oil tamponade to extract the silicone oil as well as the increased risk for the development of glaucoma. In gas tamponade, postoperative prone positioning is required to be maintained by the patient. 5 For both techniques, HSO, as well as APC with gas tamponade, satisfactory results with closure rates each up to 86% have been reported,5,19,20,21 but there is an ongoing interest in direct comparisons between both methods.
The purpose of this study was to investigate whether re-PPV with APC and sulfur hexafluoride 20% (SF620%) gas tamponade or HSO as primary intervention yields better functional and anatomical results after PMH surgery.
Materials and methods
Clinical records of 402 consecutive eyes with IMH and PMH that have been admitted to the Department of Ophthalmology in the University Hospital of Cologne, Germany, for PPV between October 2013 and July 2019 were reviewed retrospectively.
According to national medical regulations on retrospective single-center clinical studies, the Ethics Committee of the University of Cologne ruled that approval was not required for this study. All tenets of the Declaration of Helsinki have been regarded.
Patients’ electronic files were reviewed and the following parameters were extracted in an anonymized database, including epidemiological data, directly preoperative and postoperative best spectacle-corrected visual acuity (BSCVA) results, characterization of anatomical status, surgical technique (re-PPV with either APC and SF620% tamponade or with HSO), and surgical success rate (PMH closure (yes/no)). Complication rates and anatomical success rates after potentially necessary reoperation for PMH were additionally recorded.
Inclusion and exclusion criteria
Records of all consecutive eyes with PMHs that had undergone PPV with ILM peeling and gas tamponade for full-thickness IMH closure were reviewed and analyzed regarding inclusion and exclusion criteria. Only cases with sufficient data on (1) functional status (BSCVA), (2) anatomical characteristics based on preoperative optical coherence tomography (OCT) measurements, (3) completed re-PPV for PMH either with APC and SF620% gas tamponade or with HSO (Densiron® 68) and sufficient documentation of surgical technique and complication rates, and (4) available follow-up data, including BSCVA, and anatomical closure rate following surgery were included into this study. In cases with PMH after PMH surgery, success rates of second surgical approach were evaluated.
BSCVA results were measured in APC and gas tamponade group 6–8 weeks postoperatively, and in HSO group, prior to HSO extraction (2–3 months postoperatively) and, if available, 6–8 weeks following the HSO extraction.
Further exclusion criteria comprised complex pathologies of the anterior or posterior segment (active vascular or inflammatory vitreo-retinal diseases, high myopia > −6 D, aphakia, uncontrolled glaucoma, history of non-perforating or perforating trauma, any previous intraocular surgery despite uncomplicated cataract surgery with posterior chamber lens implantation, and history of retinal detachment).
A total of 64 cases with PMH could be identified. Thereof, in 53 cases, re-PPV with either APC and SF620% tamponade or with HSO was performed. In three cases, postoperative follow-up data were insufficient. Furthermore, two eyes had to be excluded for anatomical and functional outcome analysis because postoperative endophthalmitis (n = 1) or development of a retinal detachment (n = 1) did not allow a review of the closure rate due to missing or not evaluable OCT data.
Stand-alone standardized three-port re-PPV in phakic or pseudophakic eyes, as well as combined re-PPV with phacoemulsification and posterior chamber lens implantation for co-existent cataract were included.
For outcome analysis, two groups depending on the surgical technique were defined: (1) re-PPV with APC and SF620% tamponade, and (2) re-PPV with HSO (Densiron 68).
Surgical technique and postoperative treatment
All eyes underwent three-port re-PPV (20-gauge or transconjunctival, sutureless 23-gauge) in a standardized fashion as reported before. In case of co-existent cataract, cataract extraction was performed by standard 2.8-mm clear cornea bimanual phacoemulsification followed by the posterior chamber, in-the-bag lens implantation prior to PPV. Furthermore, the enlargement of ILM rhexis was performed at the operating surgeon’s discretion. At least a circle approximately reaching to the vascular arcades and centered on the MH was peeled off. Retinal breaks or degenerations have been identified and either laser retinopexy or cryotherapy has been performed. 1
Surgical groups
Re-PPV with APC and SF620%
The APC was prepared 1 day before the surgery in the Institute for Transfusion Medicine, University Hospital of Cologne, Germany. Venous blood (250 mL) was taken from the patient, and platelet-rich plasma was prepared by centrifugation. The platelet-rich plasma was stored until the next day at 22°C and again centrifuged at the day of surgery. The average resulting concentration was 10 × 109 platelets/mL.
For application, first fluid–air exchange was performed, and then two to three drops of the APC were applied over the PMH with a vitrectomy back-flush needle mounted on a 1-mL syringe. All patients received an SF620% gas tamponade. Patients were instructed to keep supine position at the day of surgery, and from the second day, patients were instructed to keep a strict face-down position at least for 1 week.
In cases of PMH following this procedure, re-re-PPV was performed with HSO tamponade as a third approach if a further attempt to close the PMH was made and desired by the patient.
Re-PPV with HSO group
HSO (Densiron 68; Geuder Fluoron GmbH, Neu-Ulm, Germany) was used as tamponade in all patients. The formation of Densiron 68 is a combination of the higher density F6H8 and polydimethylsiloxane. It has the density of 1.06 g/cm3 and the viscosity of 1400 mPa s at 25°C.
In cases of PMH under Densiron 68, re-re-PPV with silicone oil extraction and meanwhile APC and SF620% tamponade was performed as a third surgery if a further attempt to close the PMH was made and desired by the patient.
All patients received routine postoperative management in the form of topical antibiotic and anti-inflammatory agents in tapering doses over 2–3 weeks.
Spectral domain-OCT examinations
All eyes underwent macular examination using spectral domain-OCT (SPECTRALIS® HRA-OCT; Heidelberg Engineering GmbH, Heidelberg, Germany) preoperatively as well as postoperatively. The specific scan protocol was a custom raster scan pattern with 37 sections (512 A-scans each) in a 30° × 20° field of view. Preoperative anatomical characteristics were measured using the following parameters: persistent macular hole–inner opening diameter (PMH-IOD), persistent macular hole–minimum linear diameter (PMH-MLD), persistent macular hole–base diameter (PMH-BD), and persistent macular hole–height (PMH-H; Figures 1 and 2).1,24 Furthermore, pre- and postoperatively macular volume (MV) was measured. Therefore, the Early Treatment Diabetic Retinopathy Study grid (6 mm × 6 mm square grid) was first manually replotted to the foveal center, and errors in device-provided segmentation lines were corrected manually. MV (mm3) was extracted from the topographic map of macular cube scan. 23
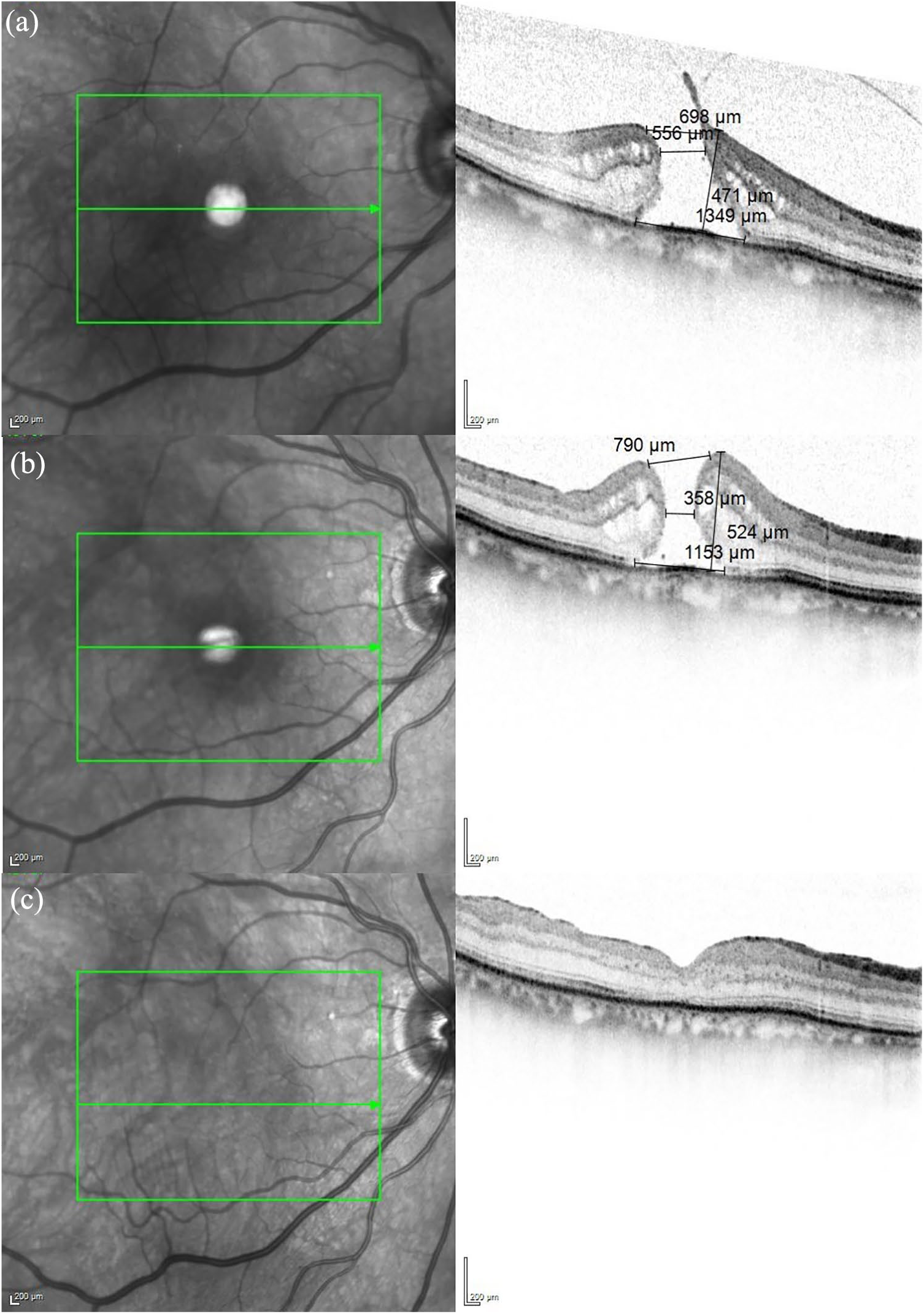
Anatomical closure of a persistent macular hole with autologous platelet concentrate and sulfur hexafluoride 20% gas tamponade. Optical coherence tomography (OCT) scans of the right eye of a 71-year-old female patient are shown: (a) the idiopathic macular hole (IMH) before pars plana vitrectomy with internal limiting membrane peeling and gas tamponade, in which best spectacle-corrected visual acuity (BSCVA) was 0.8 logMAR; (b) the persistent macular hole (PMH), in which BSCVA was 1.0 logMAR; and (c) the result after re-vitrectomy with autologous platelet concentrate and sulfur hexafluoride 20% gas tamponade, in which BSCVA was 0.2 logMAR.
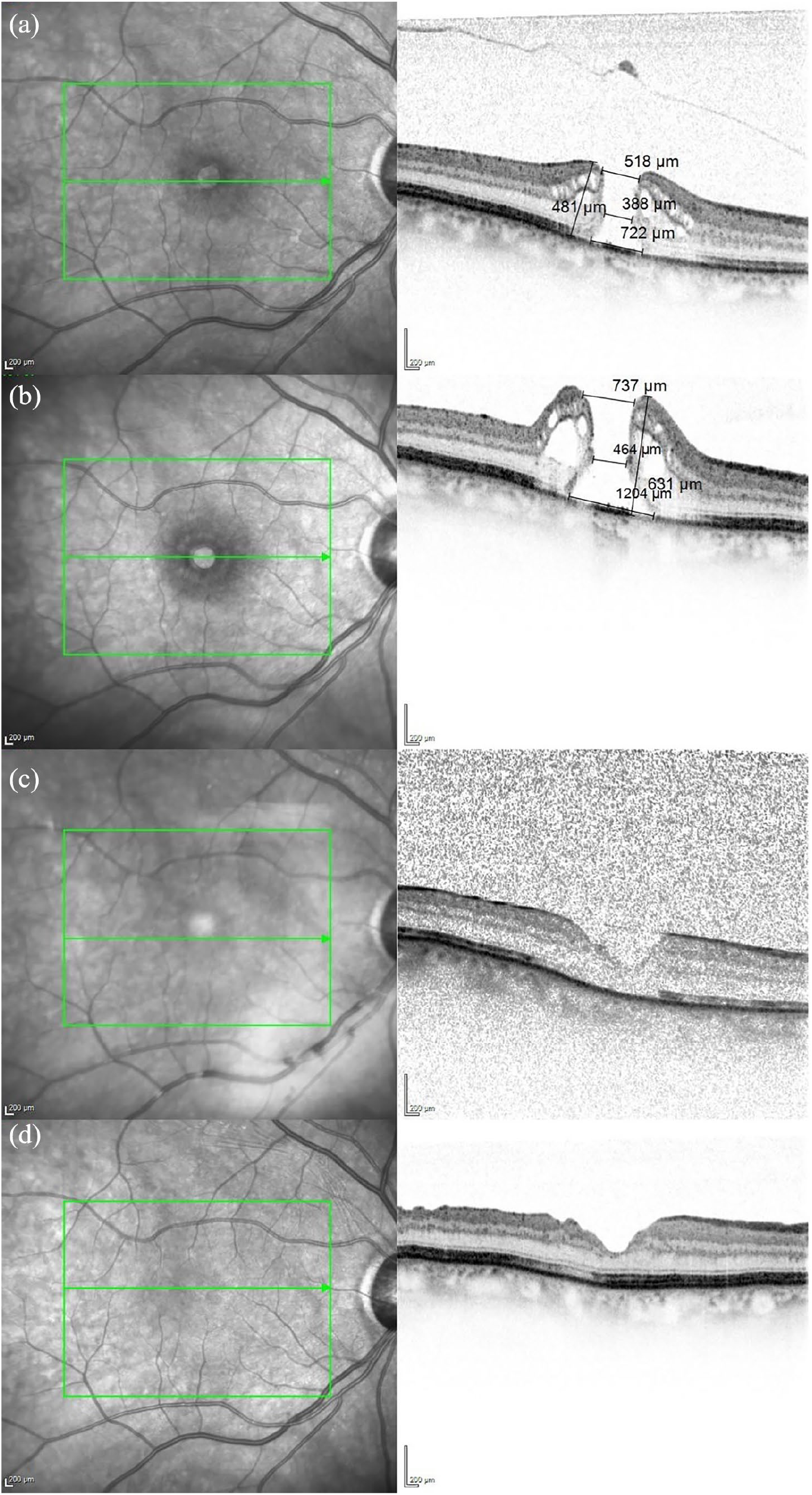
Anatomical closure of a persistent macular hole with heavy silicone oil tamponade. Optical coherence tomography scans of the right eye of a 74-year-old female patient are presented: (a) the idiopathic macular hole before pars plana vitrectomy with internal limiting membrane peeling and gas tamponade, in which best spectacle-corrected visual acuity (BSCVA) was 0.6 logMAR; (b) the persistent macular hole, in which BSCVA was 0.8 logMAR; (c) the result after re-vitrectomy with heavy silicone oil (Densiron 68) tamponade, in which BSCVA was 0.8 logMAR; (d) the final result after silicone oil removal, in which BSCVA was 0.4 logMAR.
Postoperatively, holes were considered closed, indicating anatomical success, if there was a complete reattachment of the circumferential hole rim.
Statistical analyses
Data were collected and analyzed by SPSS (version 25.0 for Windows; SPSS, Inc., Chicago, IL, USA). The study cohort was grouped by surgical technique in the above-defined two endotamponade groups. Anatomical success rates were determined for each group (PMH closure (yes/no)). Pre- and postoperative BSCVA results were converted to the logarithm of minimum angle of resolution (logMAR). Descriptive analysis was performed. For statistical significance testing for interval scale parameters, Student’s t-test (PMH-MLD, PMH-IOD, PMH-H, PMH-BD, and MV) and Mann–Whitney U test (BSCVA) were applied depending on the normal distribution of parameters. Chi-squared test was used for ordinal scale parameters (closure rates). The level of significance was defined as p < 0.05. The Bonferroni procedure was performed to correct p values for multiple testing.
Results
A total of 402 consecutive eyes with the diagnosis of MH were identified, thereof 54 eyes with IMH developed PMH after PPV with ILM peeling and SF620% gas tamponade at our site and 10 eyes were admitted to our department with PMH following PPV with gas tamponade previously performed elsewhere in Germany. Of those 64 eyes with PMH, 16 had to be excluded from analysis: in 11 cases, patients rejected undergoing additional surgery, and in 3 cases, postoperative follow-up data were insufficient. Furthermore, two eyes had to be excluded for anatomical and functional outcome analysis because of postoperative endophthalmitis (n = 1) or development of a retinal detachment (n = 1). Overall, 48 eyes were eligible for the analysis. Thereof, in 24 eyes (50%), primary anatomical closure failed, whereas in 24 eyes (50%), anatomical closure could be achieved.
Subgroup analysis was performed along the primary surgical approach for PMH repair
Re-PPV with APC and SF620% gas tamponade (n = 13)
Mean age was 72.5 ± 9.7 years (range = 45–86 years) and female–male ratio was 8:5. Six right eyes (46.2%) and nine eyes were phakic (69.2%), whereas four eyes were pseudophakic (30.8%). Mean BSCVA before surgery was 0.90 ± 0.22 logMAR (range = 0.70–1.50 logMAR), and anatomical characteristics were as follows: PMH-MLD: 454.1 ± 211.3 µm (range = 405–838 µm), PMH-IOD: 772.5 ± 172.4 µm (range = 445–1003 µm), PMH-H: 564.9 ± 130.3 µm (range = 405–838 µm), PMH-BD: 1092.5 ± 294.7 µm (range = 625–1620 µm), and MV: 8.94 ± 0.70 mm3 (range = 7.78–10.08 mm3).
Anatomical closure was achieved in eight eyes (57.1%), whereas in five eyes, PMH could not be closed (35.7%). Visual acuity for successfully treated eyes was postoperatively 0.79 ± 0.63 logMAR (range = 0.2–1.9 logMAR).
Seven eyes (53.8%) showed increased BSCVA results, three eyes (23.1%) showed stable BSCVA results, and three eyes (23.1%) showed decreased visual acuity following first re-PPV with APC and SF620%. Visual acuity for failed closure was 0.78 ± 0.50 logMAR (range = 0–1.3 logMAR).
Out of the five eyes, only two were additionally operated with HSO—one was successful (50%) and one still failed (50%). There were no cases of endophthalmitis or retinal detachment postoperatively.
Re-PPV with HSO (n = 35 cases)
Mean age was 70.7 ± 8.3 years (range = 47–83 years) and female–male ratio was 28:7. Twenty-five right eyes (71.4%) and 28 eyes were phakic (80.0%), whereas 7 eyes were pseudophakic (20.0%). Mean BSCVA before surgery was 1.07 ± 0.26 logMAR (range = 0.7–1.7 logMAR) and anatomical characteristics were as follows: PMH-MLD: 518.8 ± 171.1 µm (range = 229–884 µm), PMH-IOD: 833.3 ± 181.0 µm (range = 477–1177 µm), PMH-H: 634.8 ± 207.7 µm (range = 318–1388 µm), PMH-BD: 1286.7 ± 463.2 µm (628–2644 µm), and MV: 9.54 ± 1.2 mm3 (range = 7.66–14.16 mm3).
Anatomical closure was achieved in 16 eyes (45.7%), whereas in 19 eyes, the PMH could not be closed (54.3%). All 35 cases underwent at least one more operation. Thereof, in 16 cases with anatomical success, HSO was removed without any additional tamponade.
Visual acuity postoperatively and prior to HSO removal for successfully treated eyes was 0.79 ± 0.29 logMAR (range = 0.2–1.3 logMAR). Visual acuity after HSO removal in closed PMH cases was 0.49 ± 0.39 logMAR (range = 0.1–1.3 logMAR). Eleven eyes (31.4%) showed increased BSCVA results, nine eyes (25.7%) showed stable BSCVA results, and 15 eyes (42.5%) showed decreased visual acuity following first re-PPV with HSO tamponade.
Visual acuity for failed closure was 1.18 ± 0.45 logMAR (range = 0.3–1.9 logMAR). Of the 19 failed cases, in one eye, silicone oil was changed, and in two eyes, silicone oil was removed without any additional surgical approach for PMH closure, whereas in 16 eyes, re-re-PPV with APC and SF620% was performed. Of the 16 eyes that were reoperated with APC and SF620% to achieve anatomical closure, in 8 eyes (50%), re-surgery was successful, whereas in 6 eyes (37.5%), the PMH persisted. In two eyes, follow-up data were insufficient.
After re-re-PPV for extraction of HSO, two eyes developed purulent endophthalmitis postoperatively, and one eye had to be re-vitrectomized due to proliferative vitreoretinopathy retinal detachment.
Tables 1 and 2 display the detailed description of demographic, preoperative anatomical data, and pre- and postoperative functional data of study cohort, grouped by surgical technique and primary success (anatomical closure of PMH).
Demographic and clinical data of eyes with persistent macular hole grouped by surgical closure and surgical techniques: anatomical closure of persistent macular holes.
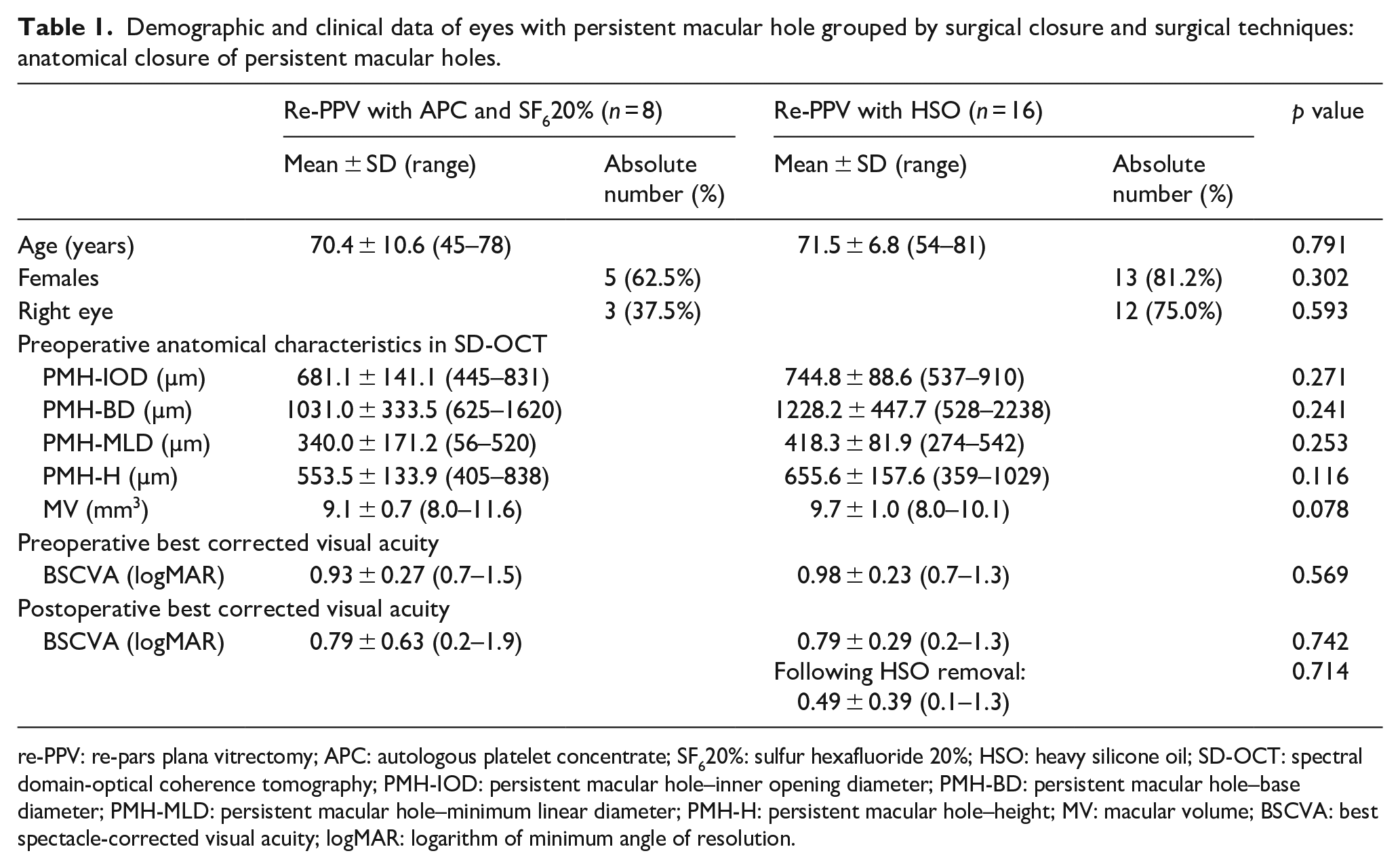
re-PPV: re-pars plana vitrectomy; APC: autologous platelet concentrate; SF620%: sulfur hexafluoride 20%; HSO: heavy silicone oil; SD-OCT: spectral domain-optical coherence tomography; PMH-IOD: persistent macular hole–inner opening diameter; PMH-BD: persistent macular hole–base diameter; PMH-MLD: persistent macular hole–minimum linear diameter; PMH-H: persistent macular hole–height; MV: macular volume; BSCVA: best spectacle-corrected visual acuity; logMAR: logarithm of minimum angle of resolution.
Demographic and clinical data of eyes with persistent macular hole grouped by surgical closure and surgical techniques: failed treatment of persistent macular holes.
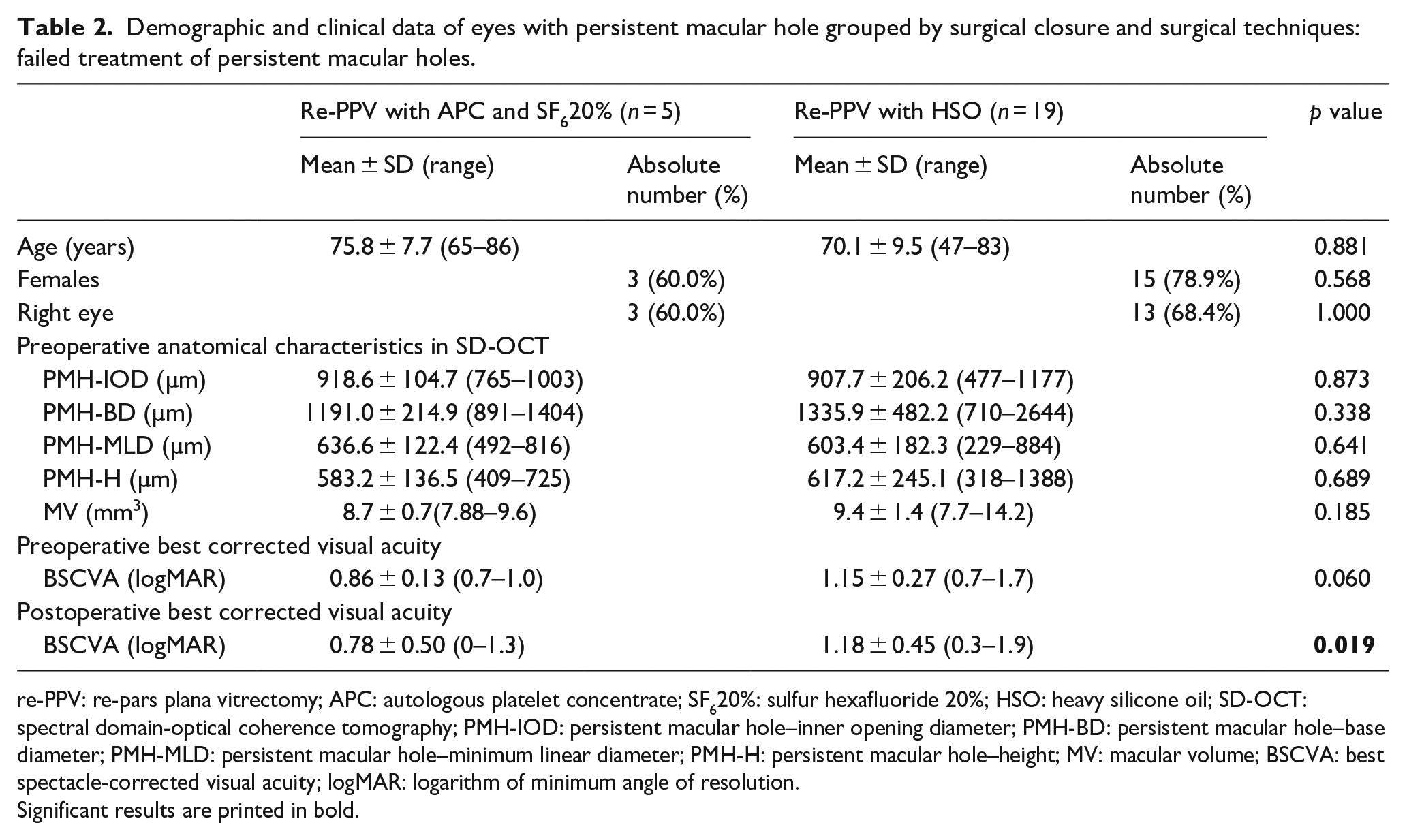
re-PPV: re-pars plana vitrectomy; APC: autologous platelet concentrate; SF620%: sulfur hexafluoride 20%; HSO: heavy silicone oil; SD-OCT: spectral domain-optical coherence tomography; PMH-IOD: persistent macular hole–inner opening diameter; PMH-BD: persistent macular hole–base diameter; PMH-MLD: persistent macular hole–minimum linear diameter; PMH-H: persistent macular hole–height; MV: macular volume; BSCVA: best spectacle-corrected visual acuity; logMAR: logarithm of minimum angle of resolution.
Significant results are printed in bold.
Figure 1 and 2 demonstrate exemplary cases with anatomical success following both surgical techniques.
Differences in outcome parameters between tamponade groups
There were no statistical significant differences between patient characteristics and pre-surgical anatomical or functional characteristics. Postoperative functional results were comparable without statistical significant differences if a PMH could be closed. In cases with still PMH following surgery, BSCVA results were significantly better following re-PPV with APC and SF620% tamponade (0.78 ± 0.50 logMAR vs 1.18 ± 0.45 logMAR; p = 0.019) when compared to re-PPV with HSO (Tables 1 and 2). The first closure attempt with re-PPV and APC and SF620% tamponade had a slightly higher success rate compared to HSO (APC and SF620% tamponade: 57.1%, whereas in HSO: 45.7%; p = 0.102). For the second closure attempt by re-re-PPV, success rates were 50% for both procedures.
Discussion
This study aims to compare two different approaches for PMH closure surgery using APC and gas tamponade or HSO tamponade. HSOs have been successfully proposed by several groups to treat PMH.20,21,22 Rizzo et al.21,22 showed that PMH closure could be achieved in 86% by HSO tamponade. Lappas et al. 20 reported the closure rate of 83% with mean BSCVA results of 0.84 ± 0.24 logMAR. Visual acuity improved in three quarters of treated patients. HSO tamponade does not require postoperative posturing, and a continuous therapeutical effect can be expected. In contrast to this advantage, patients are required to undergo additional surgery for silicone oil removal after 2–3 months. Furthermore, injecting silicone oil may cause inflammation and emulsion which potentially leads to the development of secondary glaucoma. 5 In consequence, the use of HSO in PMH always translates a two-step process for the patient with a time span of 2 months minimum.
In PMH surgery using APC with gas tamponade, closure rates of up to 85.2% with final BSCVA results of 0.5 ± 0.4 logMAR have been reported by Purtskhvanidze and colleagues. The major advantage of this approach is the absent need for re-surgery if PMH closure is achieved. 19 Valldeperas and Wong 25 reported a final PMH closure rate of 75% in a cohort of 51 eyes, and Dimopoulos et al. 26 reported a rate of 78% for the use of APC and gas.
These three studies do not incorporate suitable control group. Our study compares both approaches, HSO and APC with gas showing better closure rates for the APC group in the direct comparison. However, in both subgroups of our study, closure rates are lower than in cited studies.
Our study has major limitations. The major limitation of our study is the retrospective design and the relatively small sample size. In a larger cohort, it would be interesting to further differentiate eyes with small or lager PMHs, or to compare eyes depending on symptom duration or interval between onset of primary or PMHs and surgery.
Furthermore, we cannot report long-term visual acuity results due to a lack of follow-up data in clinical routine, especially in APC and SF620% group, which gives the impression whether BSCVA results seem to be unsatisfying in comparison. This may be due to the small sample size and the retrospective design of our study. However, it seems to be important to notice that in more than 50% of the APC group, an increase in BSCVA results could be achieved by one surgery, whereas in the HSO group, only about 30% showed increase in BSCVA following the first surgery for PMH. It would be desirable to address the question of which technique is of greater benefit to our patients in a prospective study, especially to gain long-term results.
To conclude, our study can show that re-PPV with APC and SF620% gas is at least non-inferior and as safe as HSO in PMH surgery. The closure rate seems to be slightly higher with the same or even lower complication rates. Fewer reoperations are required and the postoperative visual acuity seems to be more stable even if PMH surgery is unsuccessful. Especially when PMH closure failed, APC with SF620% seems to be superior regarding visual outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.