
Abstract
Purpose:
To describe the clinical findings and outcomes in patients who presented with uveitis associated with multiple sclerosis.
Methods:
Retrospective review of 20 patients (38 eyes).
Results:
The most frequent ocular finding was multifocal elongated retinal perivenous “sheathing” with focal vascular leakage on fundus fluorescein angiography in 29 eyes followed by vitreous snowballs and debris in 26 eyes, anterior chamber inflammation in 15 eyes, mutton-fat keratic precipitates in 14 eyes, posterior synechiae in 13 eyes, cystoid macular edema in 9 eyes, iris nodules in 4 eyes, and optic neuritis in 3 eyes. Patients with cystoid macular edema were treated successfully with systemic corticosteroids combined with mycophenolate mofetil. Ocular complications were cataract in 6 eyes, glaucoma in 2 eyes and vitreous hemorrhage in 1 eye.
Conclusions:
Multifocal elongated retinal perivenous “sheathing” with focal vascular leakage on fundus fluorescein angiography is the most frequent finding in uveitis associated with multiple sclerosis.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease of the central nervous system (CNS) white matter and a common cause of neurological disability in young adults that has a wide variety of ophthalmic and neuro-ophthalmic manifestations. 1 The diagnosis of MS is defined by the presence of demyelinating lesions, separated by time and space, in the brain and spinal cord.1,2 It is predominantly affecting young and middle-aged females with estimated female to male ratio to be 3.5:1. 3 The disease is commonly behaving as relapsing-remitting (RRMS) type in around 65% of patients. In this condition, the disease is characterized by episodes of neurological manifestations followed by remission. In RRMS some patients may develop more progressive form known as secondary progressive MS. In minority of patients, the disease may present as primary progressive MS (PPMS) that affects both males and females equally and progresses slowly resulting in severe neurological disabilities in most of the patients.3,4
Various ocular involvements have been associated with MS including optic neuritis, ocular motor abnormalities, internuclear ophthalmoplegia, nystagmus, and uveitis.1,5–10 In large studies, the frequency of uveitis among patients with MS ranges from 0.65% to 1.1% with an average prevalence of 0.82%. 5 On the other hand, MS is reported among patients with uveitis, with a frequency of 0.9% to 1.7% with an average mean prevalence of 1.03%. 5 In a previous report, we demonstrated that the incidence of uveitis associated with MS was 1.5%. 11 In patients with uveitis associated with MS, intermediate uveitis is the most frequent anatomical diagnosis followed by panuveitis. 12 Several complications have been reported in uveitis associated with MS including cataract, cystoid macular edema (CME), band keratopathy, glaucoma, retinal detachment, retinoschisis, vitreous hemorrhage and occlusive vasculitis.13,14 The most common cause of mild visual impairment in uveitis associated with MS is CME associated with intermediate uveitis. 15
The aim of this study is to investigate the clinical features at presentation and long-term outcomes in patients with uveitis associated with MS.
Patients and methods
We retrospectively reviewed the medical records of 1000 patients with uveitis referred to the uveitis clinic of King Abdulaziz University Hospital, Riyadh, Saudi Arabia, between January 2000 and November 2018. We identified 20 patients (38 eyes) that were diagnosed to have MS. Demographics and clinical data that were collected included age, gender, laterality, best-corrected visual acuity (BCVA), intraocular pressure (IOP), presence of keratic precipitates, severity of anterior chamber inflammation, presence of posterior synechiae, cataract, vitreous debris and snow balls, optic nerve head assessment, vascular sheathing, macular edema, and treatment modalities.
Optic coherence tomography (OCT) to asses macular edema and fundus fluorescein angiography (FFA) were done for all patients. Basic uveitis workup was performed for all patients and included complete blood cell count, erythrocyte sedimentation rate, laboratory serum fluorescent treponemal antibody absorption detection and venereal disease research laboratory, serum angiotensin-converting enzyme, serum lysozyme, tuberculin skin testing, and chest radiography to exclude other uveitic entities.
After excluding other specific uveitic entities, magnetic resonance imaging (MRI) was ordered for patients who were suspected to have MS including those who have neurological manifestations at presentation and for those with clinical ocular findings suggestive for uveitis associated with MS such as multifocal elongated retinal perivenous “sheathing” with focal vascular leakage on FFA with or without granulomatous anterior segment inflammation (Figures 1–3). Uveitis classification was based on the International Uveitis Study Group classification system, where patients were categorized as having anterior uveitis, intermediate uveitis, posterior uveitis, or panuveitis. The diagnosis of intermediate uveitis was made when the vitreous is the major site of the inflammation. Uveitis was further classified as non-granulomatous if fine endothelial keratic precipitates were seen in the absence of iris nodules and/or choroidal granulomas, and granulomatous if larger keratic precipitates, including large mutton-fat keratic precipitates, Koeppe and/or Busacca iris nodules. 16
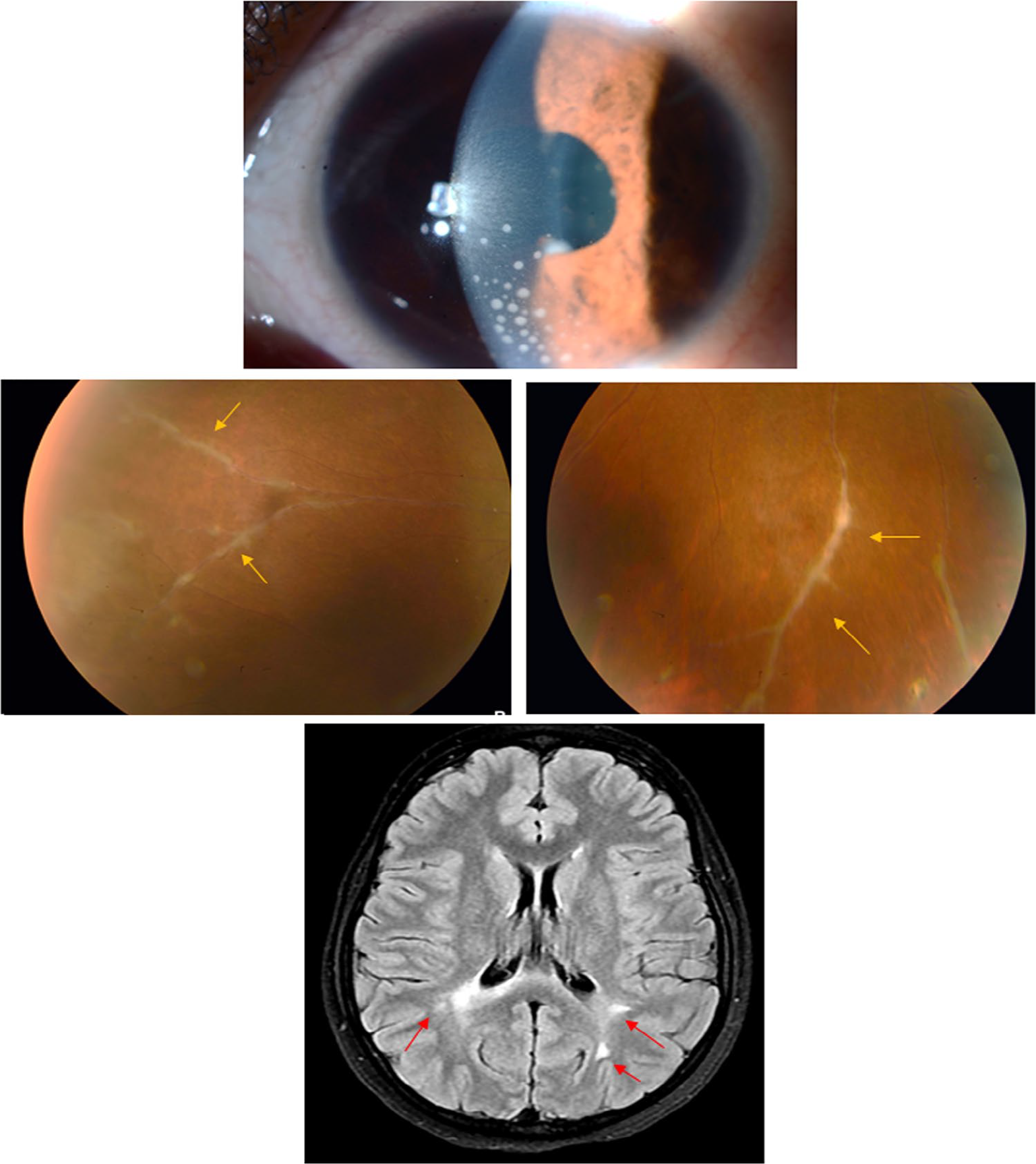
Slit-lamp biomicroscopy of a 24-year-old woman with uveitis associated with multiple sclerosis showing granulomatous keratic precipitates (upper row). Fundus photographs of the right eye showing elongated retinal perivenous sheathing (arrows) (middle row). Magnetic resonance imaging of the brain axial view showing multiple periventricular demyelinating lesions (arrows).
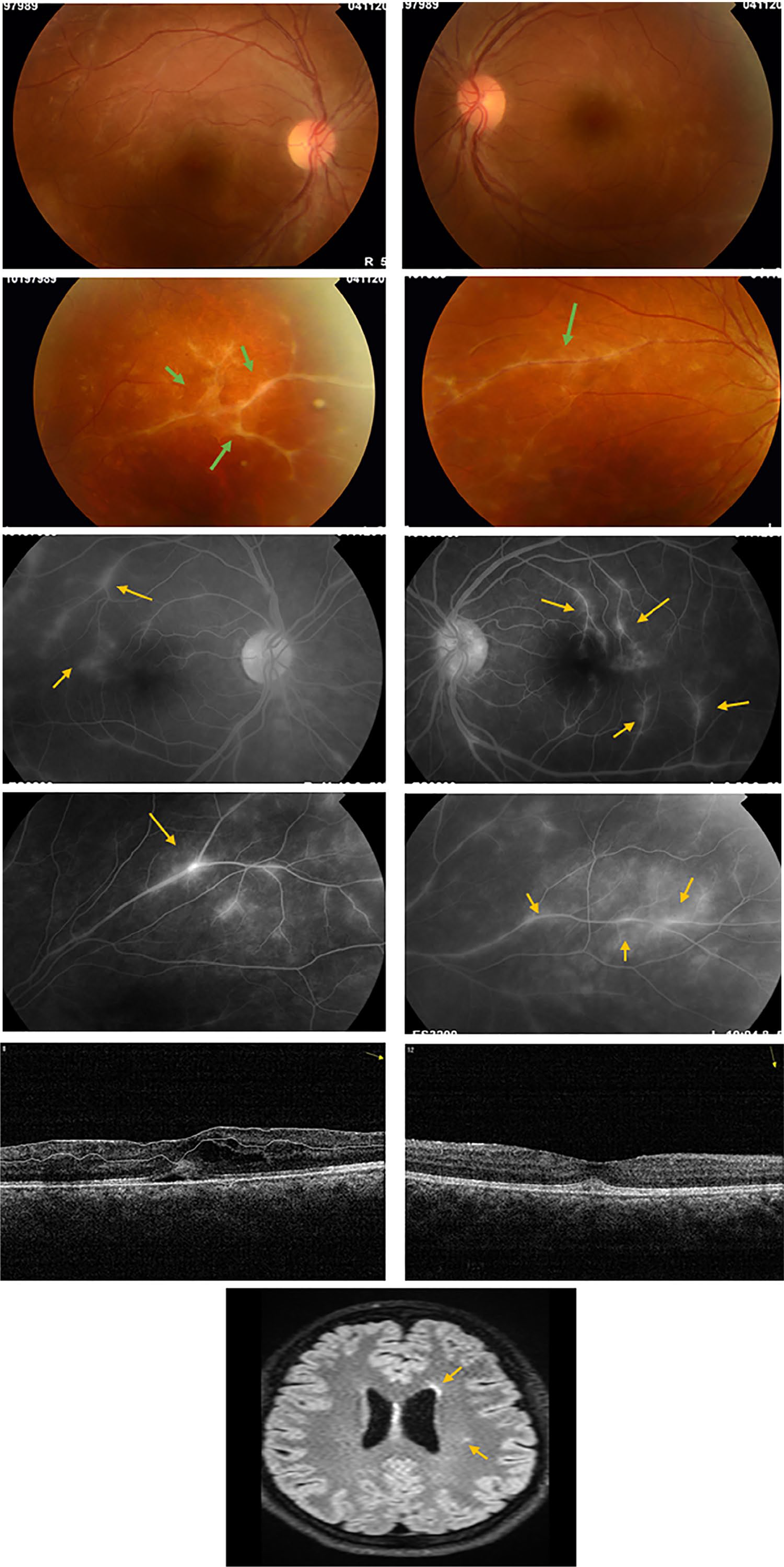
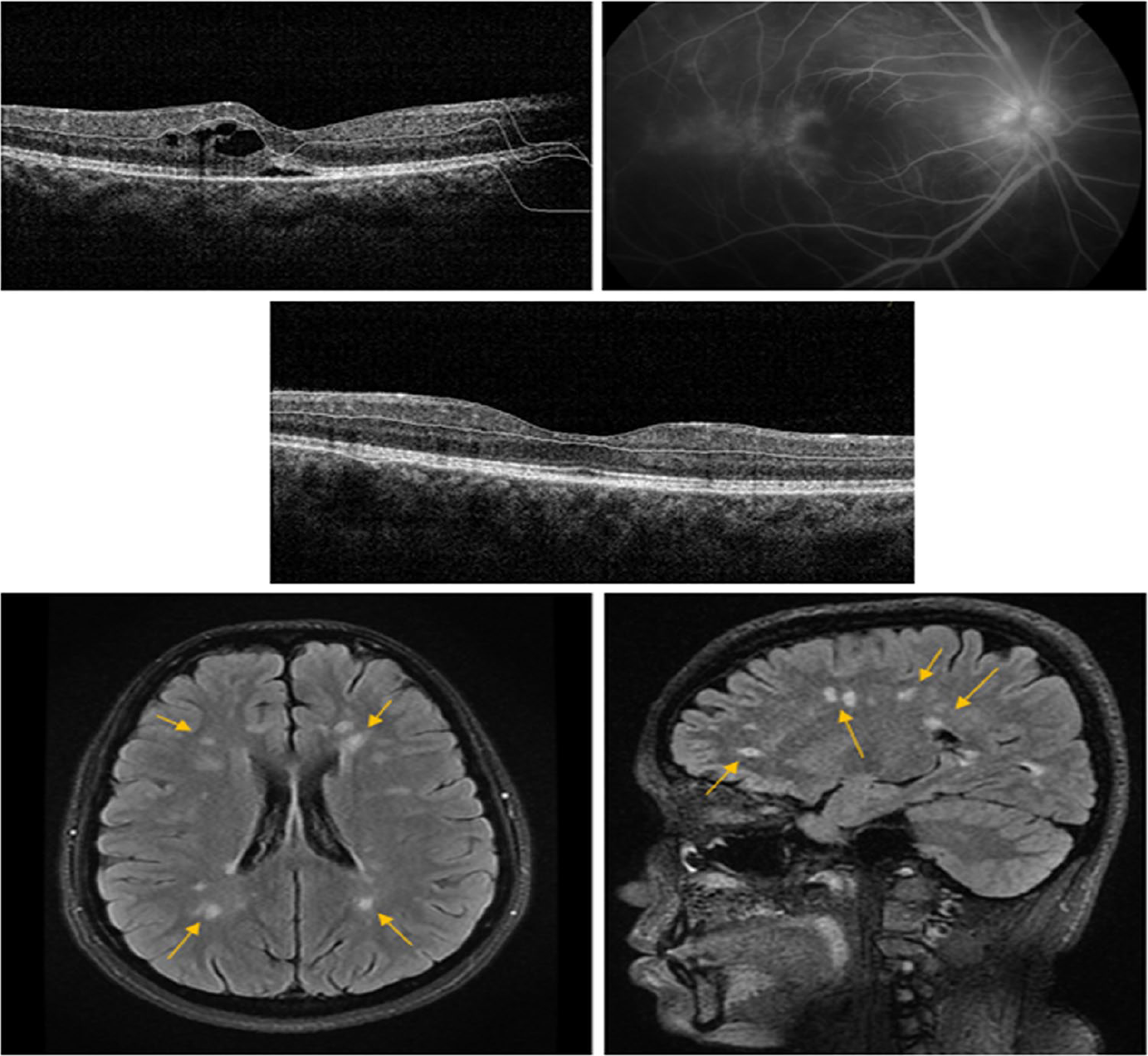
Fundus photographs of right and left eyes of a 23-year-old woman with uveitis associated with multiple sclerosis. Note the elongated retinal perivenous sheathing (second row). Fluorescein angiography shows focal leakage in the macular and peripheral retinal vessels (third and fourth rows). Optical coherence tomography showing cystoid macular edema of the left eye (fifth row left) and resolved edema 3 weeks after receiving systemic corticosteroids combined with mycophenolate mofetil (fifth row right). Magnetic resonance imaging of the brain axial view confirms the presence of demyelinating lesions.
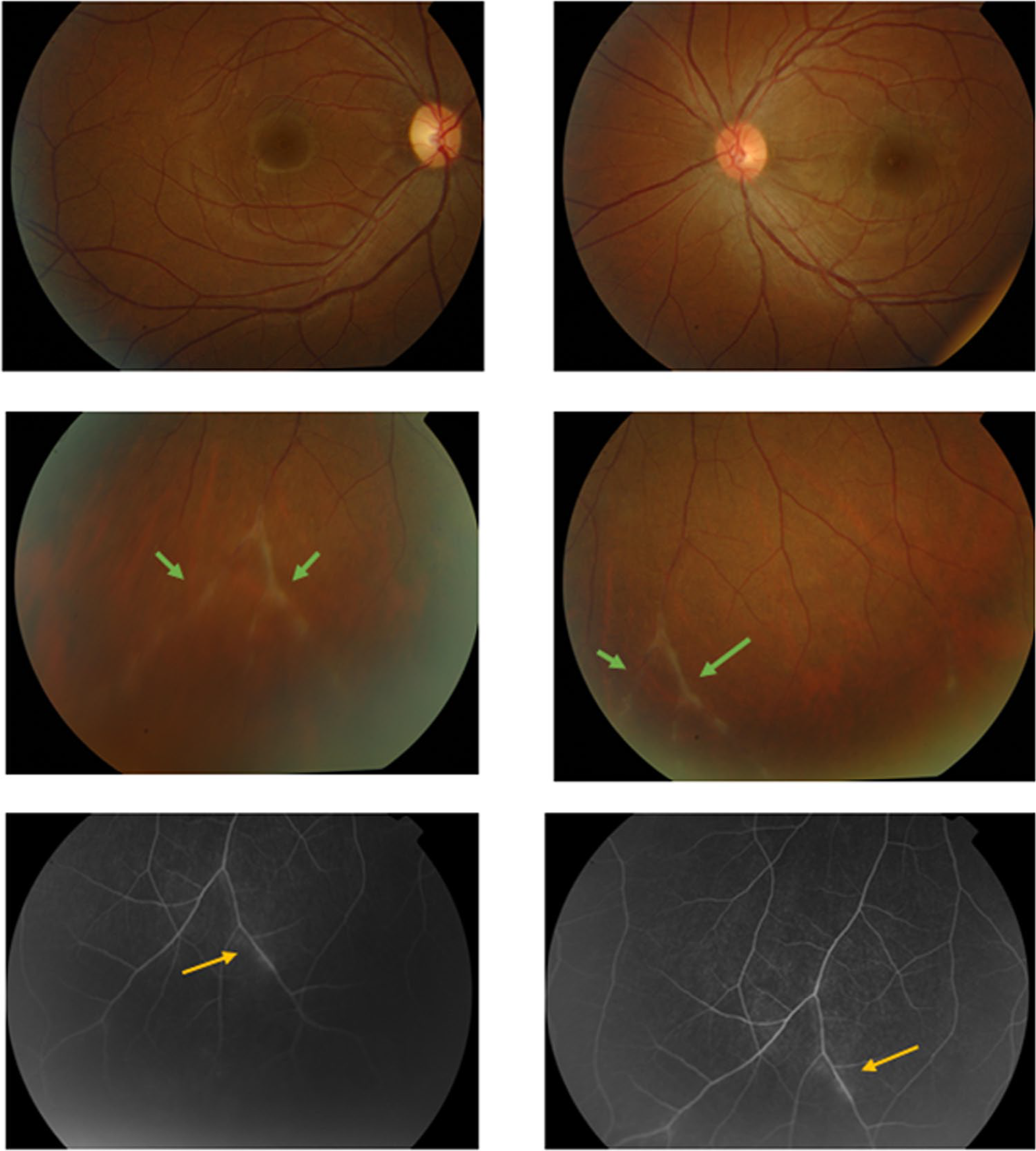
A 19-year-old woman with uveitis associated with multiple sclerosis. Fundus photographs of right and left eyes showing multifocal elongated peripheral retinal perivenous sheathing (arrows) (first and second rows). Fluorescein angiography showing focal vascular leakage (arrows) (third row).
All patients were seen and evaluated at MS clinic after the diagnosis of uveitis associated with demyelinating CNS lesions. Patients were classified as clinically isolated syndrome or clinical definite MS based on modified McDonald criteria. 17
Results
In this study, out of 1000 patients with uveitis, 36 (3.6%) patients had MRI of the CNS during the uveitis workup. Twenty of these 36 patients were found to have MS. Therefore, the prevalence of MS in our cohort of patients with uveitis was 2%. These patients were managed and followed-up by two of the authors, A.M.A. and A.-K.D. The patients were 19 (95%) females and 1 (5%) male. The age at presentation ranged from 12 to 52 years (mean: 29.5 ± 10.11 years). Uveitis was bilateral in 18 (90%) patients and unilateral in 2 (10%) patients (38 eyes). The follow-up period ranged from 12 to 120 months (mean: 42 ± 32.6 months).
Panuveitis was the most common anatomic diagnosis in 17 (44.7%) eyes followed by intermediate uveitis in 14 (36.8%) eyes, anterior uveitis in 6 (15.7%) eyes and posterior uveitis in 1 (2.6%) eye.
Clinical features
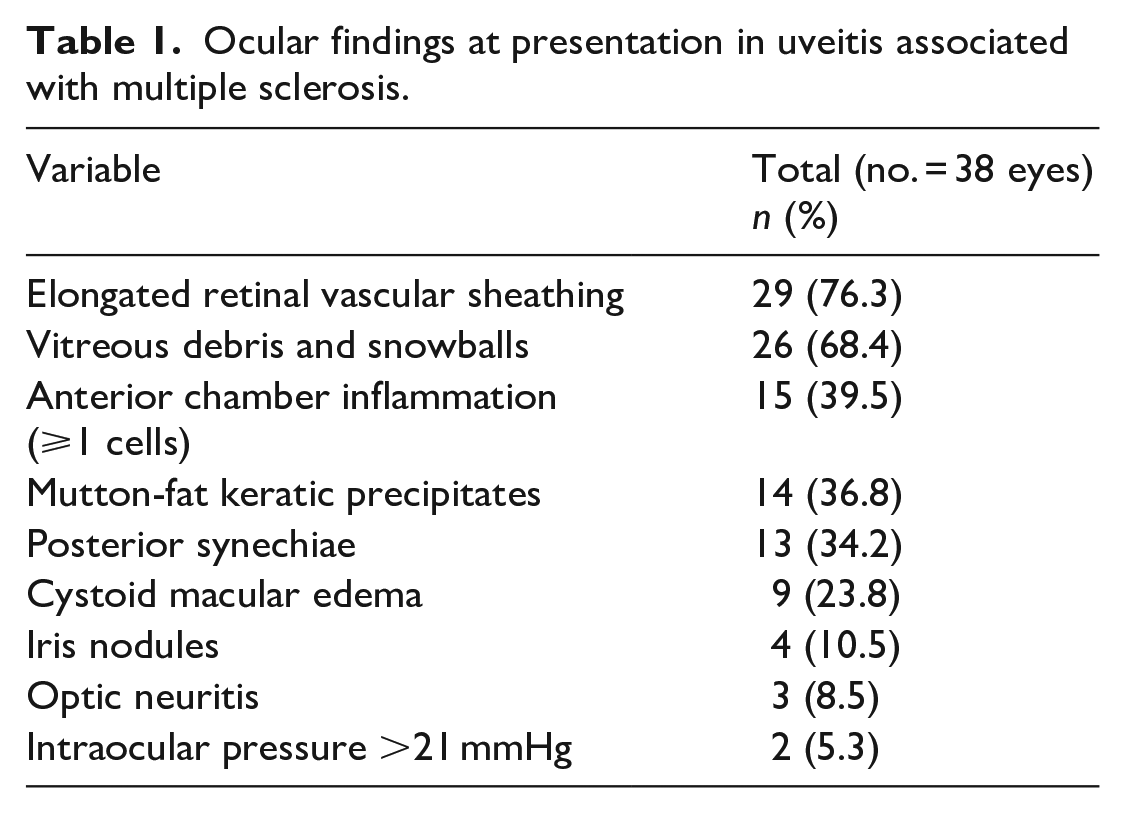
Multifocal elongated retinal perivenous “sheathing” was the most frequent clinical sign present in 29 (76.3%) eyes. All these eyes showed focal vascular leakage on FFA (Figures 1–3). This was followed by vitreous debris and snowballs in 26 (68.4%) eyes, anterior chamber cells in 15 (39.5%) eyes, mutton-fat keratic precipitates in 14 (36.8%) eyes (Figures 1 and 4), posterior synechiae in 13 (34.2%) eyes, CME in 9 (23.7%) eyes (Figures 2 and 5), iris nodules in 4 (10.5%) eyes, and high IOP in 2 (5.3%) eyes. At presentation, optic neuritis was diagnosed in 3 (15%) patients (3 eyes). All these patients presented with decreased vision, color vision defect, relative afferent pupillary defect, and visual field effect upon neuro-ophthalmic evaluation (Table 1).
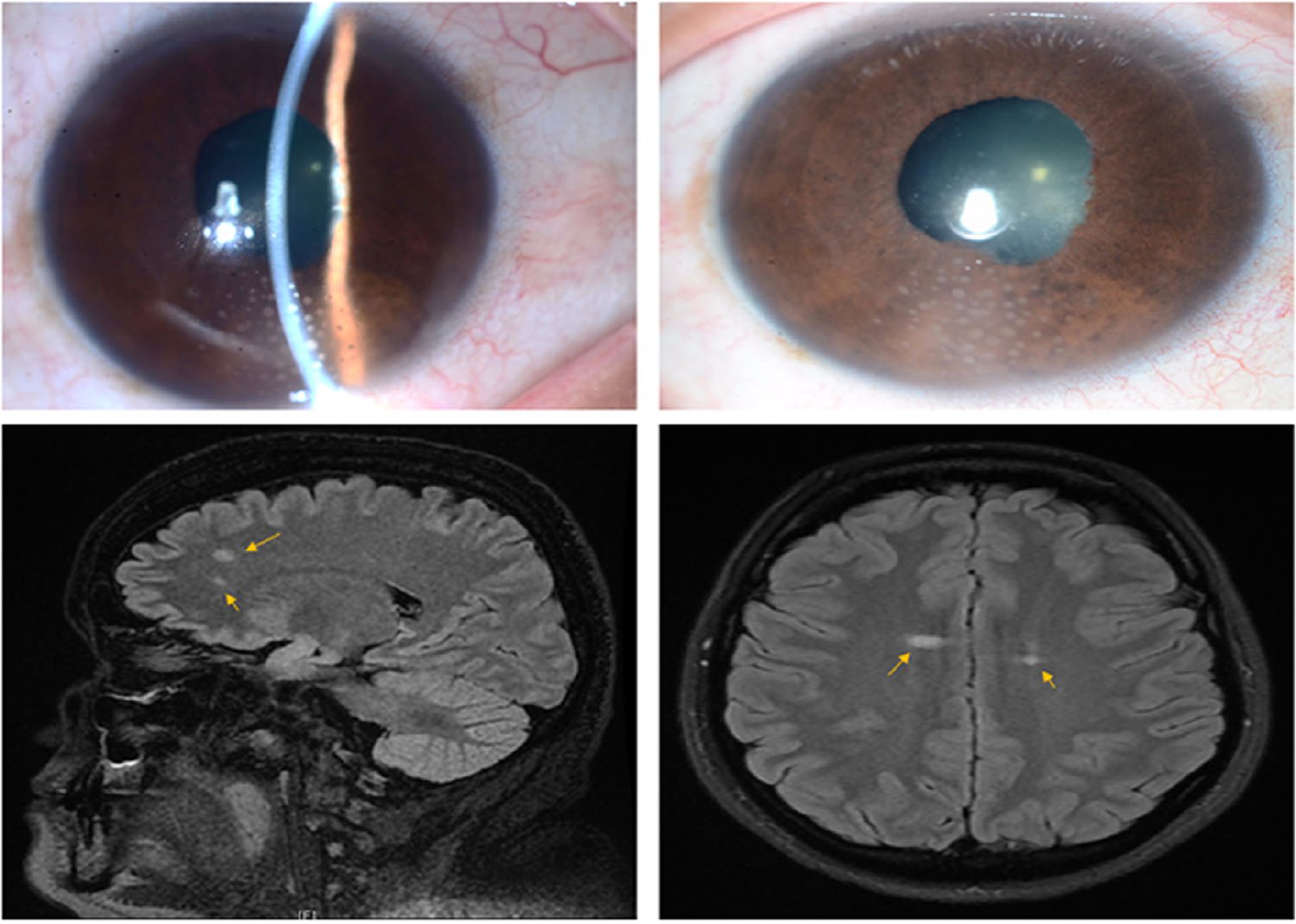
Slit-lamp biomicroscopy of the right eye of a 40-year-old woman who presented with uveitis associated with multiple sclerosis showing mutton-fat keratic precipitates and posterior synechiae (first row). Magnetic resonance imaging of the brain sagittal and axial view showing multiple periventricular demyelinating lesions (arrows) (second row).
A 27-year-old woman with uveitis associated with multiple sclerosis. Optical coherence tomography (OCT) of the right eye showing cystoid macular edema (CME) (first row left). Fluorescein angiography of the right eye showing optic disk leakage and cystoid macular edema (first row right). OCT right eye 1 month after treatment showing resolved CME (second row). Magnetic resonance imaging of the brain axial and sagittal view showing multiple periventricular demyelinating lesions (arrows) (third row).
Ocular findings at presentation in uveitis associated with multiple sclerosis.
The most frequent ocular complications detected during follow-up were cataract in 6 (15.8%) eyes, glaucoma in 2 (5.2%) eyes, epiretinal membrane in 2 (5.2%) eyes, and vitreous hemorrhage in 1 (2.6%) eye.
Clinical features of patients with uveitis suspected to have MS with normal MRI of the CNS
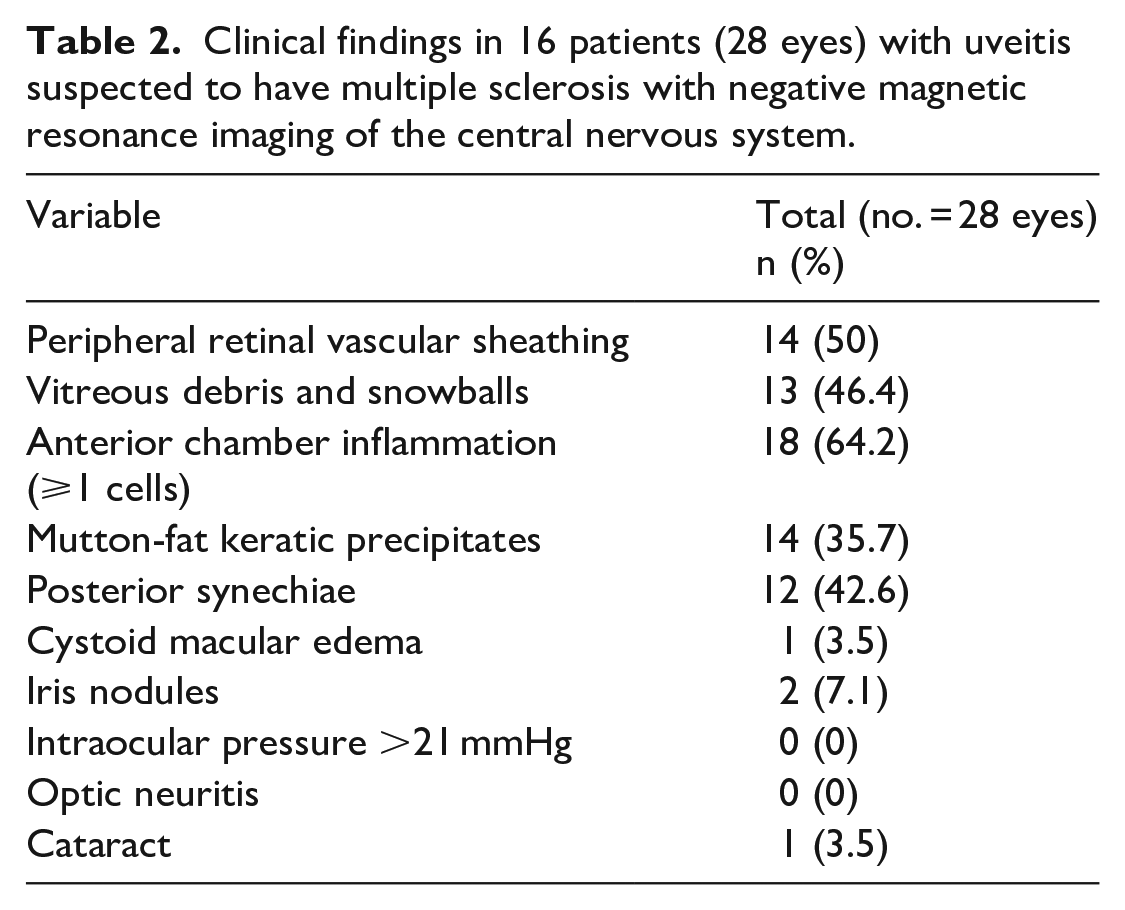
Of the 36 patients who underwent MRI for the CNS to rule out MS, 16 (44.4%) patients (28 eyes) had normal MRI. These patients were 13 (81.3%) females and 3 (18.8%) males. The age at presentation ranged from 15 to 33 years (mean: 22.7 ± 6.2 years). Uveitis was bilateral in 14 (87.5%) patients and unilateral in 2 (12.5%) patients. The follow-up period ranged from 8 to 84 months (mean: 42.9 ± 27.7 months). The clinical findings of these patients are summarized in Table 2. Of these 16 patients, 4 (25%) were diagnosed to have ocular sarcoidosis and the other 12 (75%) were labeled as idiopathic.
Clinical findings in 16 patients (28 eyes) with uveitis suspected to have multiple sclerosis with negative magnetic resonance imaging of the central nervous system.
Neurological findings
At presentation, 5 (25%) patients had clinical definite MS. In addition, 6 (30%) patients developed clinical definite MS during follow-up period. The interval between the diagnosis of uveitis and development of neurological symptoms in these patients ranged from 4 to 30 months (mean: 12.5 ± 9.4 months). The remaining 9 (45%) patients were labeled as clinically isolated syndrome after a follow-up period ranging from 12 to 98 months (mean: 47 ± 29.9 months). Of 11 patients with clinical definite MS, 10 (90.9%) patients were diagnosed to have RRMS and 1 (9.1%) patient was diagnosed to have PPMS.
Treatment of uveitis associated with demyelinating CNS lesions
Thirteen (65%) patients needed systemic treatment at one stage during follow-up. Oral prednisolone was the most common systemic medication used in 13 (65%) patients. Mycophenolate mofetil (MMF) was used in 9 (45%) patients who presented with CME, and intravenous methyl prednisolone was used in 3 (15%) patients who had associated optic neuritis. Seven (35%) patients were treated with topical prednisolone acetate 1% eye drops for the associated anterior segment inflammation.
Treatment of MS
Among the 20 patients who had uveitis associated with MS, 11 (55%) had clinical definite MS. Intravenous methylprednisolone 1 g daily for 5 days was used in these patients during the new relapses. Other immunomodulatory agents that were used included interferon-beta in 6 (54.5%) patients, natalizumab in 3 (15%) patients, and fingolimod in 2 (18.2%) patients.
Visual outcome for the whole study group
Table 3 displays the baseline and final BCVA of all eyes with uveitis associated with MS. Thirty (79%) eyes achieved BCVA of 20/40 or better at last follow-up. None of the eyes had BCVA of ⩽20/200 at last follow-up compared to 3 (7.9%) eyes at presentation. The prevalence of BCVA of 20/40 or better increased from 20 (52.6%) eyes at presentation to 30 (79%) eyes at final follow-up.
BCVA at presentation and at last follow-up.
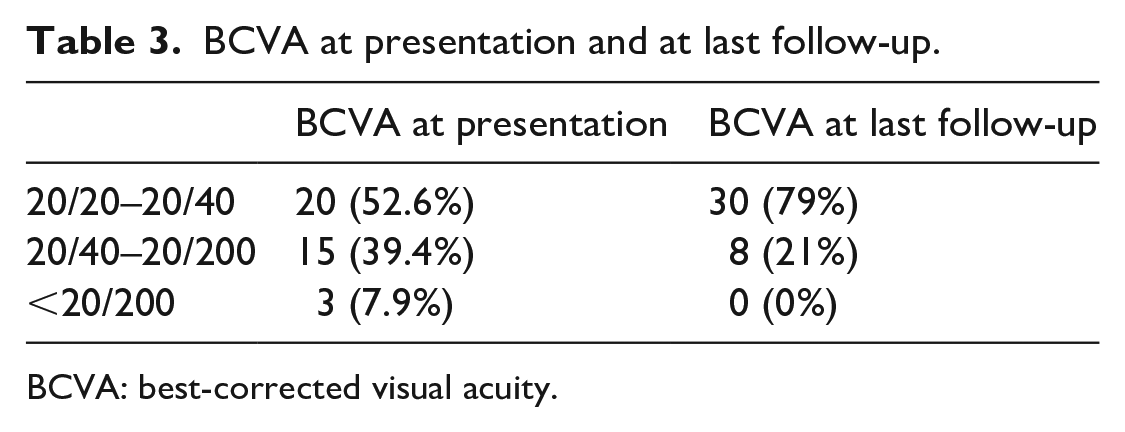
BCVA: best-corrected visual acuity.
Discussion
This study was conducted to investigate clinical features at presentation and long-term follow-up of 20 patients with uveitis associated with MS. The mean follow-up period in our study was 42 months (range: 12–120 months). Out of 1000 patients seen in our uveitis clinic between January 2000 and November 2018, 36 (3.6%) patients had MRI of the CNS during the uveitis workup. Among these patients, 20 (2%) patients (38 eyes) were found to have MS. It should be emphasized that in comparison with other series of patients, our series was among the largest. 5 In large studies of patients with uveitis, the prevalence of MS ranged from 0.9% to 1.7%5,18 with an average mean prevalence of 1.03%. 5
MRI of the CNS is not a routine investigational tool in uveitis workup and is mainly ordered for the highly suspected cases to have CNS demyelinating lesions. Recommendations about pertinent indications of MRI among uveitis patients are still lacking. 3 In a previous report, MRI of the CNS was only recommended for patients with medical history and/ or neurological findings suggestive of MS or if the patient is planned for treatment with anti-tumor necrosis factor-α to exclude signs suggestive of MS, since the condition can be made worse using these immunomodulatory agents. 4 In another report, MRI of the CNS was recommended for cases of intermediate uveitis if associated with neurological findings or presence of snow balls along with retinal vasculitis in asymptomatic patients. 19 Our indications for requesting MRI imaging of the CNS during the workup of uveitis include the presence of neurological symptoms suggestive of MS at presentation, presence of multifocal elongated retinal perivenous “sheathing” with focal leakage on FFA with or without granulomatous anterior segment inflammation and after excluding other specific uveitic entities.
In our study, multifocal elongated retinal perivenous “sheathing” along with focal vascular leakage on FFA was the most common and consistent finding in uveitis associated with MS. In previous studies, the frequency of retinal vascular sheathing in uveitis associated with MS ranges from 9% to 58.3% of patients.19–22 Retinal vascular sheathing in patients with MS was first described clinically by Rucker in 1944. 23 Histopathological study of the periphlebitis seen in patients with uveitis associated with MS revealed perivenous infiltrates of lympho-plasmocytic cells. 24
Uveitis can be the first presenting sign of MS. 5 Similarly, in the present study, uveitis was the first presenting sign of clinical definite MS in 6 (54.5%) patients. In a large series of 6042 patients with MS, it was reported that 41 (0.7%) patients had uveitis and that uveitis was the presenting sign of MS in 15 (36%) patients. 20
In the current study, panuveitis was the most common anatomic diagnosis in 17 (44.7%) eyes followed by intermediate uveitis in 14 (36.8%) eyes which is in agreement with previous studies.20,21 In contrast, intermediate uveitis was the most common anatomic diagnosis of MS associated uveitis in other reports.17,21,25,26 In this study, granulomatous anterior segment inflammation was detected in 14 (36.8%) eyes which is consistent with previous reports.27–31
The course of uveitis associated with MS is usually favorable. Mild visual impairment is commonly seen in association with CME. In this series, unilateral CME was diagnosed in 9 (45%) patients at presentation. Of these 9 patients, 7 (35%) patients were diagnosed to have RRMS and 2 (10%) had clinically isolated syndrome. MMF combined with systemic corticosteroids was used in these patients. This treatment regimen was effective in inducing complete resolution of CME. Similarly, Hedayatfar et al. 21 reported the efficacy of MMF in patients with uveitis associated with MS. Previous studies reported the incidence of CME in patients with uveitis associated with MS to range between 26.3% and 50%.19,21,22
Poor visual outcome in patients with uveitis associated with MS is associated with posterior segment complications, such as recurrent macular edema, epiretinal membranes, and advanced glaucomatous optic disk damage. 32 In our study, 79% of the eyes achieved BCVA of 20/40 or better and none of the eyes had BCVA of ⩽20/200 at last follow-up. The visual outcome in our study was comparable with a previous study in which BCVA of 20/40 or better was achieved in 68.7% of the eyes. 32
In conclusion, multifocal elongated retinal perivenous “sheathing” with focal vascular leakage on FFA is the most common and consistent ocular finding in patients with uveitis associated with MS. These findings should prompt further diagnostic workup including MRI of the CNS to exclude the possibility of demyelinating lesions in these patients after excluding other specific uveitic entities.
Footnotes
Acknowledgements
The authors thank Ms. Connie Unisa-Marfil for secretarial work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by King Saud University through Vice Deanship of Research Chair (Dr. Nasser Al-Rashid Research Chair in Ophthalmology, AM Abu El-Asrar).
Informed consent
Patients gave their permission for photographs to be used for teaching purposes and publication.