
Abstract
A number of systemic medications are known to cause macular toxicity, and bull’s eye maculopathy is caused by some of them like hydroxychloroquine and clofazimine. A 55-year-old female, known case of vitiligo with history of undergoing methoxsalen–ultraviolet A therapy, presented with painless defective vision in both eyes. Fundus examination and autofluorescence showed macular degeneration with bull’s eye configuration. Optical coherence tomography showed perifoveal loss of photoreceptors and outer retinal thinning with foveal sparing appearing as ‘flying saucer’. Multifocal electroretinogram showed pan-macular suppression of waveforms. Patient was diagnosed as case of methoxsalen-induced advanced macular toxicity. This is the first reported case of methoxsalen-induced advanced bull’s eye maculopathy.
Introduction
Psoralen–ultraviolet A (PUVA) therapy is a form of chemotherapy which uses UVA light exposure to activate psoralen chemicals administered orally or topically. PUVA therapy is used for the treatment of several dermatoses with psoriasis, vitiligo, atopic dermatitis and cutaneous T-cell lymphoma being common indications. 1 The treatment is usually given 2–3 times a week with at least 48 hours interval, over a period of several months. 1
A number of systemic medications like thioridazine, chlorpromazine and tamoxifen are known to cause macular toxicity in various forms. However, advanced macular toxicity caused by chloroquine, hydroxychloroquine and clofazimine is known to present as bull’s eye maculopathy.2,3 In addition, bull’s eye maculopathy can be seen in other unrelated retinal disorders like cone dystrophy, Stargardt’s disease and dry age-related macular degeneration. 2
Hereby, we are presenting a case of methoxsalen-induced advanced bull’s eye maculopathy.
Case history
A 55-year-old female presented with painless defective vision in both eyes of 2 years duration. She was a known case of vitiligo for 15 years, for which she underwent PUVA therapy (three episodes weekly for 1-year duration, total 156 sessions) with 10 mg of oral methoxsalen (8-MOP) twice daily about 3 years before. Though she used UVA protective glasses during the sessions of UVA exposure, she was not advised for the use of such glasses during sunlight exposure despite the sunlight being particularly strong in southern India. She had no history of taking anti-malarial medications (chloroquine/hydroxychloroquine), steroid intake, night blindness or trauma, and there was no significant family history.
On general examination, she had depigmented patches of vitiligo over her face involving the scalp, eyebrows, ear lobules and angle of mouth (Figure 1(a)), and over flexor aspect of both arms (Figure 1(b)) and legs. Her best-corrected visual acuity was 6/12 in both eyes. Anterior segment examination was within normal limits. Fundus examination showed perifoveal ring of retinal pigment epithelium (RPE) atrophy with sparing of central subfoveal area (more prominent in the left eye) appearing as bull’s eye maculopathy in both eyes (Figure 1(c) and (d)). Spectral-domain optical coherence tomography (OCT) showed perifoveal loss of the ellipsoid zone with outer retinal thinning, and the preservation of the outer retina-RPE complex in the central fovea in both eyes (Figure 2(a) and (b)). Corroborating to the fundus picture, a near-total washout of central fovea was noted in the right eye, while central foveal sparing of outer retinal structures was more prominent in the left eye, appearing as ‘flying saucer’ sign described for hydroxychloroquine-induced bull’s eye maculopathy. 4 Fundus autofluorescence of both eyes revealed typical bull’s eye pattern with central normal autofluorescence with a ring of hypoautofluorescence which was surrounded by a ring of hyperautofluorescence (Figure 2(c) and (d)). En-face OCT at the level of ellipsoid zone showed clearly delineated defect in outer retinal layers (Figure 2(e) and (f)). A standard full-field electroretinogram (ERG) of both eyes showed normal scotopic and photopic responses; however, multifocal ERG showed pan-macular suppression of responses with loss of central ‘hill of vision’ in both eyes suggestive of advanced stage of macular toxicity (Figure 3).

Photograph showing white depigmented patches of vitiligo over face involving scalp, eyebrows, ear lobules and angle of mouth (a), and over the flexor aspect of both arms (b). Fundus photo of both eyes showing annular perifoveal macular atrophy with sparing of central foveal island (appearing reddish, more prominent in left eye compared to right eye) (c and d).
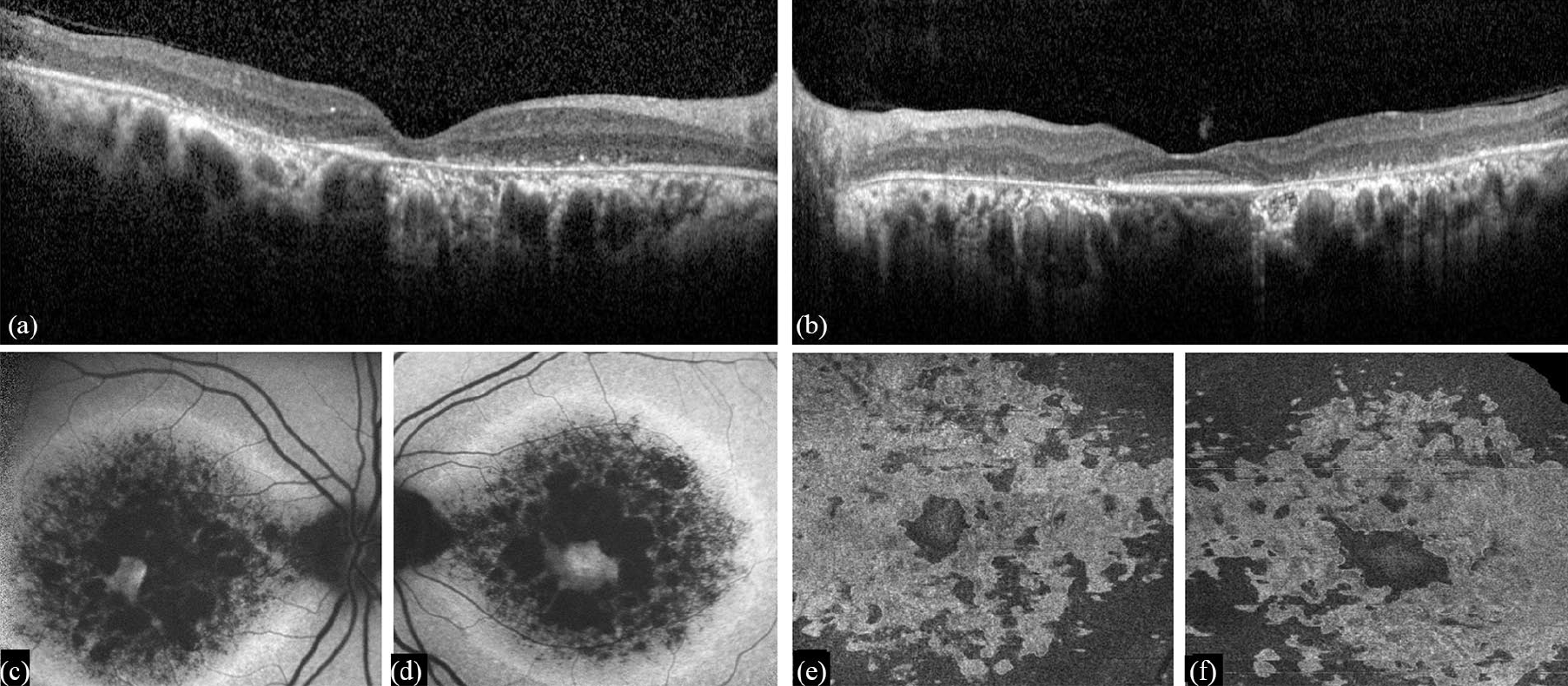
Spectral-domain OCT showing atrophic changes in macula of both eyes with perifoveal outer retinal thinning and loss of photoreceptors, and sparing of foveal photoreceptors (more prominent in left eye, and hence showing typical ‘flying saucer’ sign, while right eye having near-total washout) (a and b). Fundus autofluorescence of both eyes showing typical bull’s eye lesion with central normal autofluorescence with rings of hypoautofluorescence, patchy hypo- and hyper-autofluorescence, and hyperautofluorescence (c and d). En-face OCT at the level of ellipsoid zone showing clearly delineated areas of photoreceptor loss (e and f).
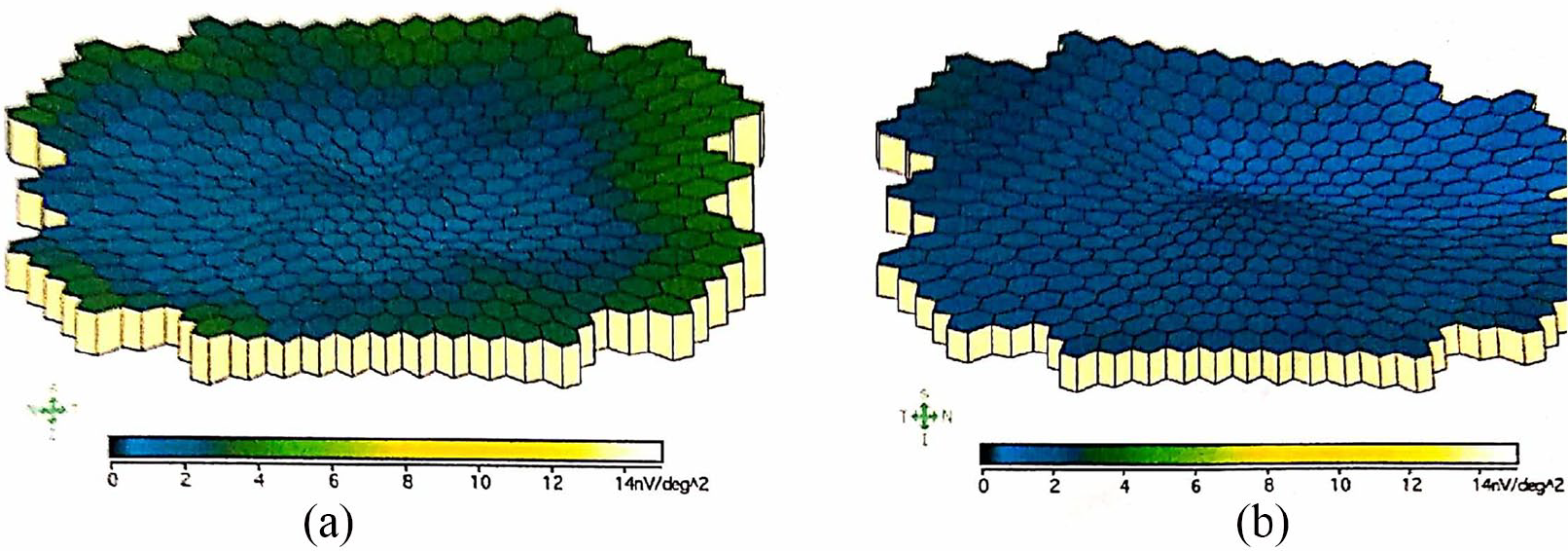
The 3-dimensional topographical display of multifocal electroretinogram of right and left eyes (a & b respectively) showing pan-macular suppression of waveforms more prominent in perifoveal region with loss of central ‘hill of vision’ suggestive of advanced macular toxicity.
Based on history, clinical examination and various investigations, a diagnosis of methoxsalen-induced advanced bull’s eye maculopathy was made, and the patient was explained about the visual prognosis. A written and informed consent was taken from the patient for using her details and images for publication.
Discussion
For various dermatoses, PUVA therapy acts by different mechanism of action altering intracellular signalling pathways. In vitiligo, PUVA induces re-pigmentation by stimulating melanogenesis. 1 The process involves the photoconjugation of psoralens to DNA in melanocytes, followed by mitosis and subsequent proliferation of melanocytes, activation of dormant melanocytes in the epidermis and appendages, increased formation and melanisation of melanosomes, and enhanced transfer of melanosomes to keratocytes. 1
In oral PUVA for vitiligo, methoxsalen is administered orally (0.6 to 0.8 mg per kg body weight) 1–3 h before exposure. 5 Following oral administration, methoxsalen is metabolized by the liver, and can be detected in plasma for 12–24 h before excretion in urine. Therefore, ocular protection with UVA blocking glasses is required from the time of oral administration of methoxsalen to next 18–24 h. 5 The ocular tissues can be exposed to its photosensitizing effect with subsequent UV radiation exposure through sunlight if protective glasses are not used, till the complete excretion potentially causing ocular toxicity.
Methoxsalen has been demonstrated in various ocular tissues like aqueous humour, crystalline lens, vitreous and retina at 3 h following oral intake in animal studies. 6 However, a number of clinical studies have demonstrated PUVA therapy as a safe treatment modality with recommended use of protective eyewear resulting in normal ophthalmological assessment and unaffected retinal function. The only complication reported following methoxsalen-UVA therapy is premature cataract formation, probably due to intra-lenticular deposits of methoxsalen forming adduct with lens protein on subsequent UVA exposure. 7
In literature, only one case of methoxsalen-induced bilateral macular toxicity is reported till now by Maitray and Rishi. 8 The toxicity was described as sub-RPE deposits with RPE elevation and thickening at the macula in both eyes. 8 However, in our case perifoveal annular atrophy of photoreceptor-RPE-choriocapillaris complex was noted. Methoxsalen-UVA therapy induces hyperplasia and hypertrophy of not only melanocytes but all the pigment-bearing cells of body including RPE cells. Increasing melanisation of melanocytes eventually results in cellular disruption of these pigment-bearing cells. 9 The possible pathophysiological mechanism of RPE-photoreceptor degeneration in our case could also be the methoxsalen-induced melanisation of RPE followed by cellular rupture. The presentation in previously reported case could be an earlier stage of methoxsalen-induced RPE toxicity, representing the pre-disruptive stage.
The exact cause of foveal sparing in cases of annular maculopathy caused by photosensitizing drugs, as seen in our case, is not well known. Possible explanation for the foveal sparing could be the attenuation of oxidative damage to the photoreceptor-RPE complex by the presence of macular yellow pigments at fovea. 2 The presence of macular yellow pigment reduces the amount of blue light striking the fovea. Also, macular yellow pigment, like other carotenoids, provides a direct anti-oxidant effect and hence neutralizes the oxidative consequences of light of any wavelength. 2
To conclude, this is the first reported case of methoxsalen-induced advanced bull’s eye maculopathy. Patients undergoing PUVA therapy should be properly counselled for extended use of UV protective glasses during sunlight exposure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.