
Abstract
Purpose:
To evaluate the choroidal vascularity index of eyes for acute and chronic central serous chorioretinopathy patients using swept-source optical coherence tomography generated en-face scans.
Methods:
This was a retrospective study, in which slabs of en-face optical coherence tomography scans, at 5 μm intervals, spanning from the retina to choroid, were binarized using a validated algorithm to calculate choroidal vascularity index. The choroidal vascularity index was defined as the ratio between the choroidal vascular luminal area and the total choroidal area. Choroidal vascularity index was calculated for all the slabs of every subject in both the groups.
Results:
A total of 30 eyes for each acute and chronic central serous chorioretinopathy groups were recruited. The mean choroidal vascularity index of the acute group was 45.21% ± 2.25% at the choriocapillaris, which increased to the maximal value of 48.35% ± 2.06% at 75% depth of the choroidal thickness and 45.31% ± 3.27% at the choroidoscleral interface; whereas for the chronic group, the mean choroidal vascularity index was 44.76% ± 2.60% at the choriocapillaris, which maximized at 50% choroidal depth (48.70% ± 1.32%) and then returned to 45.41% ± 6.02% at the choroidoscleral interface.
Conclusion:
For both groups, the choroidal vascularity index increased from choriocapillaris to maximum values at mid-choroid and returned to almost the choriocapillaris value at the choroidoscleral interface.
Keywords
Introduction
Central serous chorioretinopathy (CSC) is a chorioretinal condition more prevalent in young to middle-aged males, in particular, those who are exposed to increased exogenous or endogenous corticosteroid.1–4 Patients with CSC present with serous neurosensory retinal detachment, pigment epithelial detachment (PED), and/or pigmentary change in the macula. This condition may resolve spontaneously, may recur, or may persist to become a chronic disease.
The culprit of CSC is the pathological changes in the choroidal vasculature. The large choroidal vessels are dilated in the affected patients, and its overlying choriocapillaris and medium-sized vessels are attenuated. These vessels are also hyperpermeable, manifesting as leakage on indocyanine green angiography (ICG). 5 Therefore, in order to gain a better understanding of the pathology of CSC, we would need to study the choroid of these patients.
ICG demonstrates hyperdynamic dilated choroidal vessels in CSC; however, the leakage of the dye to the interstitial space renders quantitative analysis of the vessels inaccurate. Enhanced depth imaging optical coherence tomography (EDI-OCT) is able to visualize the choroidal layers, making precise repeatable measurement feasible. We have shown in our previous study that both large and medium choroidal vessel layers were thickened subfoveally in acute CSC compared with healthy controls, whereas only the thickening of medium choroidal vessels was significant in chronic CSC subjects. 6 However, unlike ICG, the cross-sectional B-scans of EDI-OCT or swept-source optical coherence tomography (SS-OCT) are unable to provide ophthalmologists the overall picture of the choroid status of CSC patients, since information regarding the orientation and the direction of vessels are lacking. Furthermore, vessel size does change as they go from one location to another; therefore, cross-sectional analysis of the choroid may not be the best evaluation.
Due to advances in technology, OCT scanning time of newer machines is much shorter and with higher resolution. Reconstruction of multiple macular B-scans by powerful computer processors can, therefore, provide us with noninvasive en-face OCT scans of retinal and choroidal layers of various depths, which can help in the understanding of various retinal conditions.7–10
Choroidal vascularity index (CVI) is a new imagining biomarker and is defined as the ratio between the choroidal vascular luminal area and the total choroidal area on OCT scans. 11 This parameter quantitatively describes how much the choroidal vessels are dilated in different choroidal layers and has recently been studied in various retinal and choroidal conditions.12–16 It has been demonstrated that both EDI-OCT and swept-source OCT were able to reliably measure CVI noninvasively in healthy patients. 17 We have previously reported the CVI measurement of cross-sectional OCT B-scans of CSC patients. 18 We found that eyes with active CSC had significantly higher CVI compared to fellow eyes, eyes with resolved CSC, and healthy eyes. In addition, CVI of fellow eyes of CSC patients also had significantly higher CVI when compared to healthy eyes and eyes with resolved CSC.
In this study, we would like to bring the choroidal analysis further by measuring the more representable CVI of CSC subjects based on en-face OCT images.
Methods
This was a retrospective cross-sectional study involving 30 consecutive acute CSC subjects and 30 consecutive chronic CSC subjects who attended the retina clinic of LV Prasad Eye Institute, Hyderabad, from January 2017 to December 2018. This study has been approved by the Institutional Review Board (IRB) and adhered to the tenets of the Declaration of Helsinki.
All the subjects were explained about the purpose of the study, the procedures, and study-related risks. Informed consent was obtained from every study participant. A thorough history and comprehensive ocular examination were performed to confirm the diagnosis of CSC and to rule out any other ocular and systemic pathologies. Acute CSC was defined as presenting symptoms or subretinal fluid of 6 months or less, whereas chronic CSC had similar condition lasting for more than 6 months. Distance best-corrected Snellen visual acuity (BCVA) later converted to logarithm of the minimum angle of resolution (logMAR), refractive error, and intraocular pressure (IOP) were measured, and anterior segment and fundus examination were performed with the slit lamp biomicroscopy and the indirect ophthalmoscopy, respectively. The exclusion criteria included refractive error ⩾ ±3 D, eyes with significant media opacities, macular pathologies other than CSC, any prior intraocular surgeries, or history of any systemic diseases such as diabetes mellitus or hypertension. One eye from each subject was recruited for analysis. If both eyes were affected by CSC, then the right eye was chosen for analysis.
SS-OCT imaging
Macular volumetric scans were obtained using the swept source-OCT DRI OCT Triton (Topcon Medical Systems, Japan), with a scanning speed of 100,000 A-scans/s. A total of 256 cross-sectional scans were obtained for each patient during 1–3 p.m. The data were extracted from the OCT machine with computer software program for analysis. Central macular thickness (CMT) was defined as the average subfield thickness of a 1-mm diameter circle centered on foveal center, measuring from internal limiting membrane to retinal pigment epithelium (RPE). Subretinal fluid (SRF) height was defined as the height of the hyporeflective space between the neurosensory retina and the RPE, which was measured at the center. Subfoveal choroidal thickness (SFCT) was defined as the distance between RPE–Bruch’s membrane complex and choroidoscleral interface. The transition point of the subfoveal medium-to-large choroidal vessels was identified on the OCT scans manually by two independent observers, and the average thickness of the subfoveal large choroidal vessel layer was measured.
The algorithm involved in obtaining en-face CVI measurement include (1) choroidal en-face OCT scan extraction and (2) binarization of en-face OCT scans.
Choroidal en-face OCT scan extraction
Choroid was identified from the OCT volume cube and then en-face scans separated by 5 µm were subsequently obtained for the CVI analysis. In particular, each B-scan of the volume was analyzed to segment choroid based on the previously validated algorithm, in which RPE–Bruch’s complex and choroid–scleral interface (CSI) were identified using the structural similarity index (SSIM), the Hessian analysis, and tensor voting. 19 Subsequently, segmented choroid sections were stacked to obtain the choroid volume, and multiple 5 µm spacing en-face sections were generated.
En-face CVI estimation
In order to increase the contrast between choroidal stroma and blood vessel lumen, adaptive histogram equalization was employed. Blood vessels were then separated using the block-based particle swarm optimization (PSO) thresholding. The binarized images were reviewed by two independent observers blinded to each other, to assess whether the images were correctly converted by comparing with the original en-face OCT images. This process was performed twice for each image by each observer.
CVI was calculated for every en-face image separated by 5 µm within the choroid volume. The layer of small choroidal vessel including choriocapillaris was defined as a dense network of small vessels just 10 µm beneath Bruch’s membrane. Six points of measurements were identified manually in each eye based on major anatomical locations (i.e. choriocapillaris and choroidoscleral interface) and various depths from RPE–Bruch’s membrane complex in terms of percentage of the maximum choroidal thickness across the volume cube (i.e. at 25%, 33%, 50%, and 75%, respectively).
Statistical analysis
Statistical analysis was carried out using SPSS v21 (SPSS Inc., Chicago, IL, USA). The choroidal parameters were recorded as mean ± standard deviation (SD). Normality of the data was determined. The unpaired t-test was used to compare the means of the acute group versus chronic group. Analysis of variance (ANOVA) was used to study the change in CVI at various depths of choroid within groups. Multiple regression analysis was performed on the two CSC groups to look for any correlations between CVI and age, gender, logMAR visual acuity, CMT, SFCT, and duration of disease. Linear relationships between variables were verified with scatter plots, and assumptions such as homoscedasticity, independence of observation, and lack of multicollinearity were verified by analysis with SPSS. Only p ⩽ 0.05 was considered statistically significant.
Results
Thirty consecutive patients each were recruited into acute CSC and chronic CSC groups, i.e. a total of 60 CSC patients.
The acute CSC group comprised 25 males (83.3%) and 5 females, with a mean (±SD) age of 37.3 ± 7.8 years (range = 22–54 years). All were treatment-naïve. The mean logMAR visual acuity was 0.16 ± 0.18, and the mean duration of symptoms was 46.9 ± 52.0 days. The mean CMT was 520.5 ± 216.8 μm, with the average height of SRF being 342.8 ± 248.9 μm. The mean SFCT was 439.5 ± 90.2 μm, and the large choroidal vessel thickness contributed 243.3 ± 89.6 μm. None of these 30 patients had intraretinal cyst or choroidal neovascularization, which is compatible with the usual presentation of acute CSC.
In the chronic CSC group, all 30 patients were male, with a mean age of 43.5 ± 7.1 years (range = 33–61 years). Before this episode of CSC, nine of these patients had previous micro-pulse laser treatment, six had focal thermal photocoagulation, one had verteporfin photodynamic therapy, and one had intravitreal injections of anti-vascular endothelial growth factor therapy. The mean logMAR visual acuity was 0.32 ± 0.37, and the mean duration of symptoms was 25.7 ± 26.7 months. The mean CMT was 300.3 ± 88.6 μm, with the average height of subretinal fluid being 118.7 ± 105.7 μm. The mean SFCT was 446.8 ± 70.0 μm, and the mean large choroidal vessel thickness was 249.8 ± 85.7 μm. Six patients (20%) had intraretinal cysts on OCT scans, but none had choroidal neovascularization.
En-face choroidal vascularity analysis
The overall mean CVI of the volume scan with multiple en-face sections separated by 5 μm is 47.97% ± 1.25% and 48.24% ± 1.94% for the acute and chronic CSC groups, respectively. No difference was found between the mean CVI of acute and chronic groups by the two-tailed independent t-test (p = 0.52).
The mean CVI of the acute group increased from the trough of 45.21% ±2.25% at the level of choriocapillaris (10 μm from RPE–Bruch’s complex) to the point of maximal vascularity 48.35% ± 2.06% at 75% depth of choroidal thickness and then returned to a lower level of 45.31% ± 3.27% just interior to the choroidoscleral interface. Data analysis with ANOVA with Greenhouse–Geisser correction demonstrated statistically significant differences between the mean CVI across various depths of the choroid (p < 0.0001). Post hoc tests using the Bonferroni correction showed that the mean CVI at 25%, 33%, 50%, and 75% depths of choroid was statistically significantly larger than the CVI at choriocapillaris and choroidoscleral interface (p < 0.001 in all pairwise comparisons). In addition, there was a significant change in CVI from 33% depth to 50% depth. Figure 1 shows the original en-face OCT images, shadow compensated images, and binarized images of an acute CSC patient at 20, 100, 250, and 350 μm from the RPE.
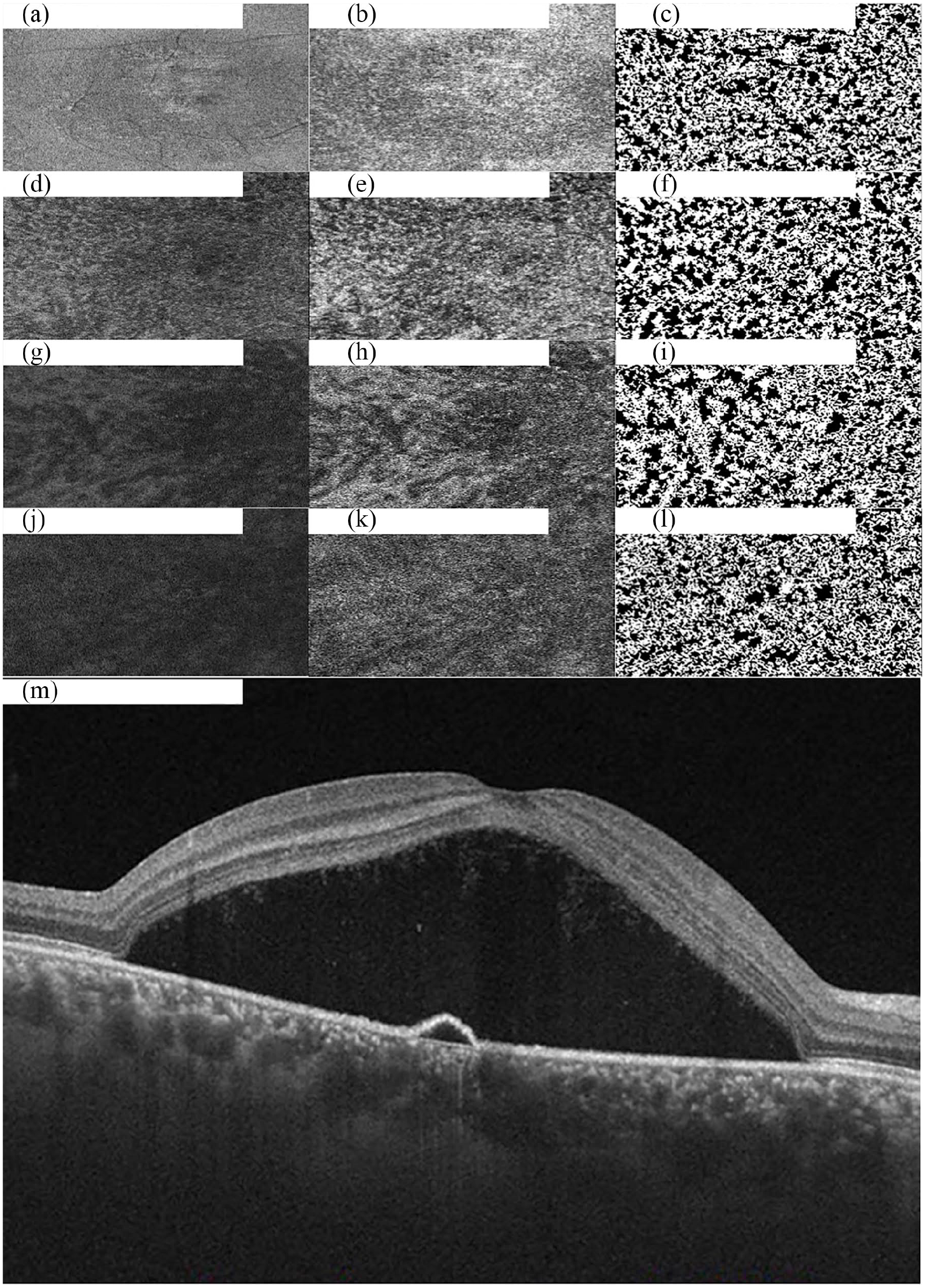
Original en-face optical coherence tomography (OCT) scans and the software-processed images of a patient with acute central serous chorioretinopathy. (a, d, g, and j) Original en-face OCT scan images at 20, 100, 250, and 350 μm; (b, e, h, and k) shadow compensated images at 20, 100, 250, and 350 μm; (c, f, i, and l) binarized images at 20, 100, 250, and 350 μm; and (m) OCT B-scan across the foveal center.
Similarly, the mean CVI of the chronic CSC group also rose from the lowest point of 44.76% ± 2.60% at the choriocapillaris to the peak vascularity level at 50% choroidal depth with a CVI of 48.70% ± 1.32% and then returned to 45.41% ± 6.02% at the choroidoscleral interface. The change in CVI across the depth of choroid was significant (p < 0.0001). Post hoc pairwise comparisons determined that the CVI changes from choriocapillaris to 25%, 33%, 50%, and 75% depths of choroid were all significant (p < 0.0001). In addition, a significant increase in CVI was also observed from 33% depth of choroid to 50% depth of choroid. Figure 2 shows the original en-face OCT images, shadow compensated images, and binarized images of a chronic CSC patient at 20, 100, 250, and 350 μm from the RPE.
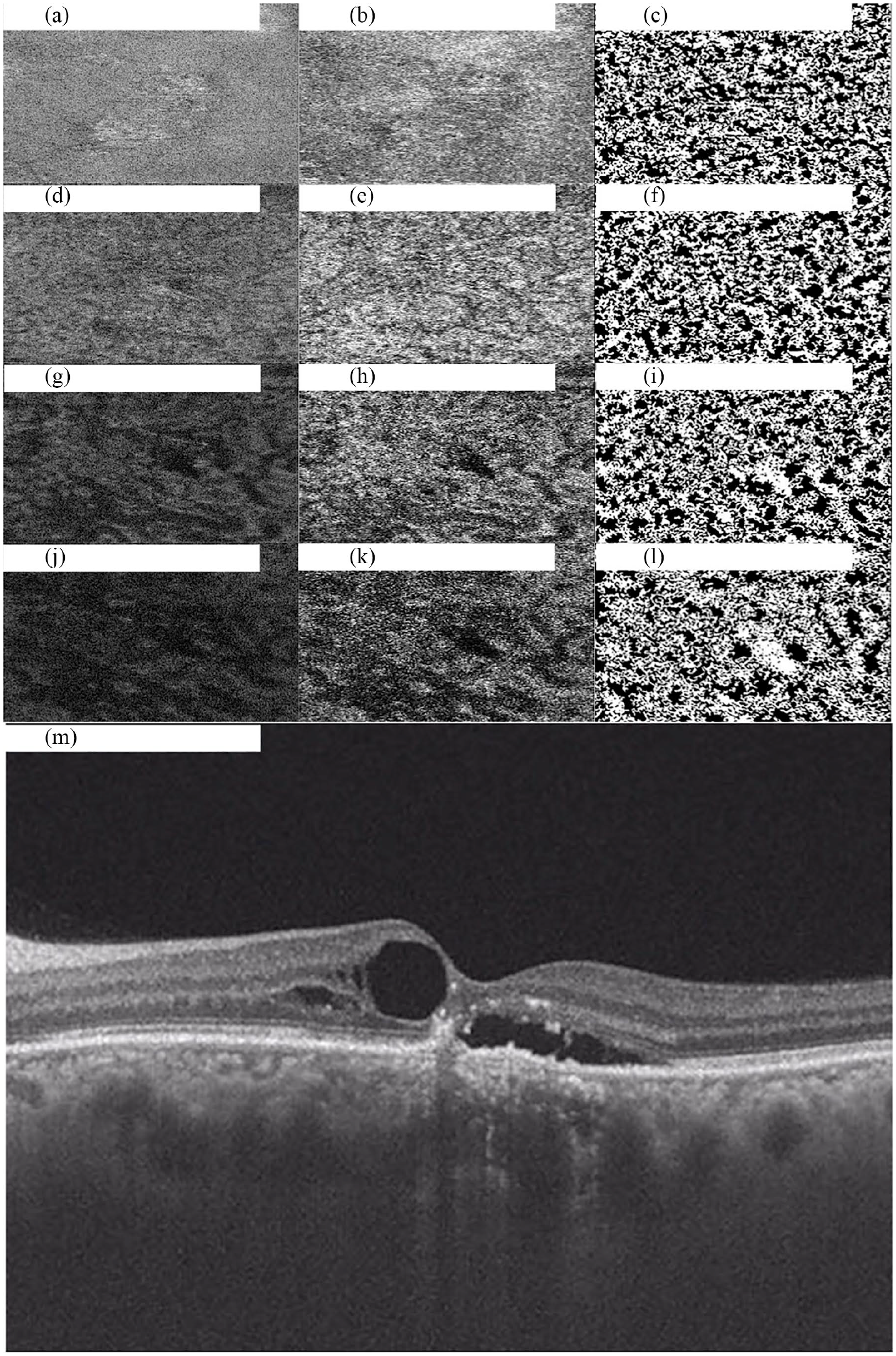
Original en-face optical coherence tomography (OCT) scans and the software-processed images of a patient with chronic central serous chorioretinopathy. (a, d, g, and j) Original en-face OCT scan images at 20, 100, 200, and 290 μm; (b, e, h, and k) shadow compensated images at 20, 100, 200, and 290 μm; (c, f, i, and l) binarized images at 20, 100, 200, and 290 μm; and (m) OCT B-scan across the foveal center.
Multiple regression analysis demonstrated that age (p = 0.195), gender (p = 0.295), logMAR visual acuity (p = 0.293), CMT (p = 0.883), and duration of disease (p = 0.399) were not significantly correlated with the mean CVI of patients, with SFCT being the closest to marginal significance (p = 0.053).
Similarly, multiple regression analysis of the chronic CSC group has been conducted on the same variables as above except for gender due to the lack of female patients in the chronic group. None of the independent factors were found to be significantly correlated with CVI, with p values for age, logMAR visual acuity, CMT, SFCT, and duration of disease being 0.482, 0.899, 0.469, 0.951, and 0.486, respectively.
Discussion
We reported the CVI of consecutive acute and chronic CSC patients, and to our knowledge, this is the first study in the literature evaluating en-face CVI of CSC patients at various levels of the choroid. The CVI of CSC patients was noted to increase as the distance from Bruch’s membrane increases, to the maximum at 75% depth of choroid in the acute CSC group and 50% depth of choroid in the chronic CSC group. This observation is compatible with our understanding of pachychoroid conditions since the pathology involves dilatation of Haller’s layer, which is the outer larger choroidal vessels, and attenuation of the choriocapillaris and Sattler’s layer, therefore the inner smaller choroidal vessels. The increase in vascularity and size of Haller’s vessels may compress on the inner choroidal vessels and result in leakage from choriocapillaris and accumulation of fluid underneath the retina.
The similar trends of increasing CVI toward maximum at mid-choroid and similar values at various depths of choroid among acute and chronic CSC groups demonstrated that choroidal status might be alike in acute and chronic CSC patients, and their differences in clinical presentation might be secondary to the loss of normal RPE functions in chronic CSC patients.
Surprisingly on multiple regression analysis, age, gender, SFCT, CMT, visual acuity, and duration of presenting symptoms were not found to be correlated with CVI. The result is counter-intuitive since one might expect higher choroidal vascularity in CSC patients with worse macular thickening or visual acuity. This interesting finding may indicate that disease manifestation may vary a lot despite similar pathology in the choroid.
The strength of our study is that this is the first en-face OCT study in the literature reporting CVI of acute and chronic CSC patients with fine cuts separated by 5 μm. This type of detailed scanning, although is time-consuming, gives us a better picture of how CVI actually varies with the depth of choroid. The binarization of images was also verified by two independent observers (intraclass correlation coefficient (ICC) = 0.97–0.98); therefore flaws, if any, in image conversion would be identified easily, making CVI calculation more accurate. There are also limitations to our study. Our study is a cross-sectional study measuring CVI at a single time point for each patient. However, choroidal thickness may vary with blood pressure and time of the day; therefore, evaluating patient’s CVI at multiple time points and obtaining the average values would be superior to the current method. Furthermore, in the chronic CSC group, some patients had undergone treatment, which may affect choroidal vasculature morphology, and therefore CVI. This is particularly important when verteporfin photodynamic therapy was performed. However, only one eye out of our 30 chronic CSC patients had photodynamic therapy done before enrollment to our study.
To conclude, we reported the CVI of acute and chronic CSC subjects and there was no difference in CVI among the two groups. The trend of changes in CVI across various depths of choroid was similar in both groups. Age, gender, visual acuity, CMT, and duration of disease were not found to be correlated with CVI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.