
Abstract
Purpose
To compare rectangular three-snip punctoplasty and polyvinylpyrrolidone-coated perforated punctal plugs for treatment of acquired lacrimal punctal stenosis.
Patients and methods
In a prospective comparative non-randomized interventional study, 80 eyes with acquired lacrimal punctal stenosis were classified into two groups. Group A was treated by insertion of polyvinylpyrrolidone-coated perforated punctal plugs (FCI ophthalmics)™ and Group B was treated by rectangular three-snip punctoplasty. The study was done in Minia University Hospital between January 2018 and April 2019. Exclusion criteria included allergic punctal stenosis, lid malposition, and lacrimal obstruction distal to the punctum. All patients were subjected to complete history taking, slit lamp examination of tear meniscus height, fluorescein dye disappearance test, punctal position, shape, size, grading of stenosis, and grading of epiphora.
Results
The mean age of the patients was 43.85 ± 14.93 years. They were 30 females and 10 males. Eepiphora Grade 3 or 4, improved postoperatively to Grade 0 or 1 in 97.5% of eyes in Group A versus 55% of eyes in Group B. All eyes (100%) in Group A versus 21 eyes (52.5%) in Group B improved regarding fluorescein dye disappearance test grade (p < 0.001). Restenosis did not occur after plug removal, while it occurred in 10% of eyes subjected to three-snip punctoplasty.
Conclusion
Perforated punctal plugs and three-snip punctoplasty are safe and effective in treatment of punctal stenosis. However, perforated plugs are less invasive, better tolerated, and have more stable results compared to three-snip punctoplasty.
Introduction
Lacrimal puncta are approximately 0.3-mm orifices positioned on the medial aspect of the eyelids. They are round or oval in youth and often collapse into fish mouth or slit configuration with age. 1 Each punctum lies on top of an elevated mound known as the papilla lacrimalis and is surrounded by a fibrous ring. 2 Punctal stenosis is a frequent cause of epiphora. It can be congenital or acquired. 3 Acquired punctal stenosis refers to a condition in which the punctum is either narrowed or occluded. 4 Caesar and McNab 5 defined it as a punctal diameter less than 0.3 mm or the inability to intubate the punctum with a 26-G cannula without dilation. Treatment options include repeated mechanical and balloon dilation, punctal snip operations, and different stenting procedures.6–8 Perforated punctal plugs were first introduced by Bernard et al., with a central hole of 0.6 mm made to permit drainage of tears. Due to the hydrophilic nature of the silicone material, accumulated secretions may block the lumen. 9 Coating the plugs with polyvinylpyrrolidone (PVP) makes them hydrophobic and allows tears and debris to flow smoothly through the perforation. 8 Different techniques of punctoplasty have been described for treatment of punctal stenosis. They include one-snip, two-snip, and three-snip procedures. 7 Three-snip punctoplasty can be further classified into a rectangular and triangular fashions. 10 In this study, PVP perforated punctal plugs and three-snip punctoplasty were compared as regard the anatomical and functional results in treatment of epiphora due to lacrimal punctal stenosis.
Patients and methods
In a prospective, comparative, non-randomized, interventional study, a total of 80 eyes of 40 patients with bilateral punctal stenosis and epiphora were included and allocated in two groups. Group A was treated by PVP-coated perforated punctal plug implants inserted in the lower punctum and Group B was treated by rectangular three-snip punctoplasty of the lower punctum. Every patient had one eye allocated in group A and the other eye was allocated in group B. Patients were recruited from the outpatient clinic of Minia University Hospital during the period from January 2018 to April 2019.
Exclusion criteria included congenital and allergic punctal stenosis, cases with canalicular, lacrimal sac or nasolacrimal duct obstruction, associated lid malposition, blepharitis, ocular surface disorders, and dry eye. In addition, patients with a history of radiotherapy, previous eyelid or lacrimal surgery were also excluded from the study. The study was approved by the local research ethical committee of the Faculty of Medicine, Minia University, and was adherent to the tenets of the Declaration of Helsinki. Detailed informed consent was taken from all patients for the surgical procedures and for inclusion in the study after thorough explanation of the procedures and all possible risks and benefits. All patients were subjected to careful history taking, including history of epiphora and its grading according to Munk scale 11 (Table 1). The patients were also asked about history of photophobia, itching, mucoid discharge, and topical medications to exclude inflammatory and allergic causes of epiphora. The position of the eyelids and puncta was examined together with the lacrimal sac region for swelling, fistula, or regurgitation.
Munk scale for epiphora grading (Munk et al. 11 ).
Slit lamp examination was done to exclude causes of increased lacrimation, to evaluate tear meniscus height (TMH) and to evaluate punctal orifices position, shape, and grading of stenosis according to Ozgur et al. 12 (Table 2). Fluorescein dye disappearance test (FDDT) was done using one drop of 2% fluorescein sodium instilled into the anesthetized lower fornix. The fluorescence of the tear meniscus was observed with the help of cobalt-blue filter. FDDT was graded according to Ozgur et al.; 12 scale consistent with the time of dye clearance with Grade 1 is <3 minutes, Grade 2 is 3–5 minutes, and Grade 3 is >5 minutes. Objective improvement was considered by postoperative decrease of the grade of FDDT. Diagnostic lacrimal probing and syringing was done to ensure patency of the lacrimal passages distal to the puncta. ENT consultation was done for all patients to exclude any nasal pathology that may induce epiphora as nasal polyps, tumors, or deviated septum.
Grading of punctal stenosis (Ozgur et al. 12 ).
Perforated punctal plugs
The plug (FCI Ophthalmics) is made of silicon and coated with a thin layer of PVP, which makes the surface slick to prevent debris from collecting on the surface and to enhance drainage with a central perforation of 0.6 mm (Figure 1). Plugs are preloaded on a disposable plug inserter to facilitate their insertion and are available in two sizes. The larger size was used in all cases.
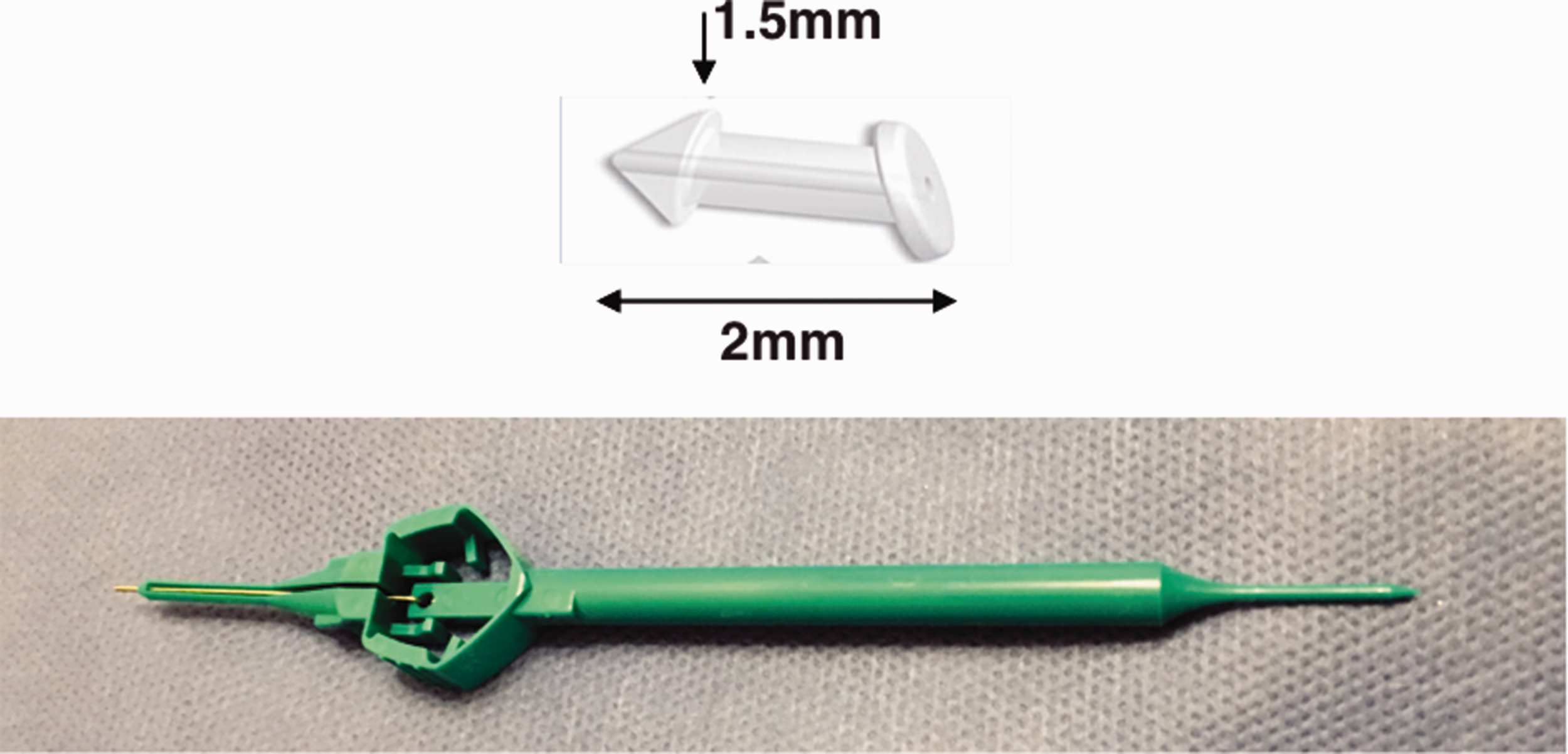
PVP perforated plugs (FCI Ophthalmics) and the inserter.
Insertion technique
Benoxinate hydrochloride 0.4% was used for surface anesthesia (Figure 2). Nettleship dilator was used to open any membrane covering the lower punctum, then was introduced vertically to dilate the punctum. Further punctal dilation was done using the dilator end of the insertor. The insertor was then held between the thumb and index finger, and the plug was orientated in the correct plane (the high end of the collar is directed toward the temporal side of the punctum). The plug was introduced gently in a vertical and progressive manner. Then it was released from the inserter by depressing the inserter handle until its end passed completely through the punctum. Topical moxifloxacin 0.5% eye drops and fluorometholone 0.1% eye drops were used four times daily for 1 week. The patients were followed up at the first postoperative day, 1 week, 1 month, and after 3 months when plugs were removed. Patients then were finally evaluated 6 months after the removal of the plugs. Removal of the plugs was done under topical anesthesia while the patient was sitting on slit lamp using fine-toothed forceps. Postoperative assessment included slit lamp examination for position of plug and TMH assessment, postoperative epiphora grading, FDDT, discomfort, or foreign body sensation, and late punctal narrowing after plug removal.

Insertion of the perforated punctal plugs (a and b) dilation of the punctum, (c–e) insertion of the plug, and (f) plug in place.
Rectangular three-snip punctoplasty
Operative procedure
After instillation of topical benoxinate hydrochloride 0.4%, subconjunctival injection of 2% lidocaine was done beneath the lower punctum, then Nettleship dilator was used to dilate the punctum (Figure 3). After grasping of the posterior wall of the punctum with fine-toothed forceps, vertical 2-mm incisions (medial and lateral side of the punctum) were done using Vannas scissors on either side of the forceps through the posterior wall of the punctum and vertical canaliculus. A horizontal incision was then made connecting the ends of the two vertical incisions to excise a rectangular portion of the posterior wall of the punctum and vertical canaliculus. Hemostasis was done by compression with a cotton tip for 1 min to stop any point of bleeding. Topical moxifloxacin 0.5% eye drops and fluorometholone 0.1% eye drops were used four times daily for 1 week. The patients were followed up at the first postoperative day, 1 week, 1 month, 3 months, and 9 months. Postoperative assessment included slit lamp examination of punctum and the wound (for healing and any signs of inflammation), TMH, postoperative epiphora grading, FDDT, discomfort or foreign body sensation, and late punctal narrowing.
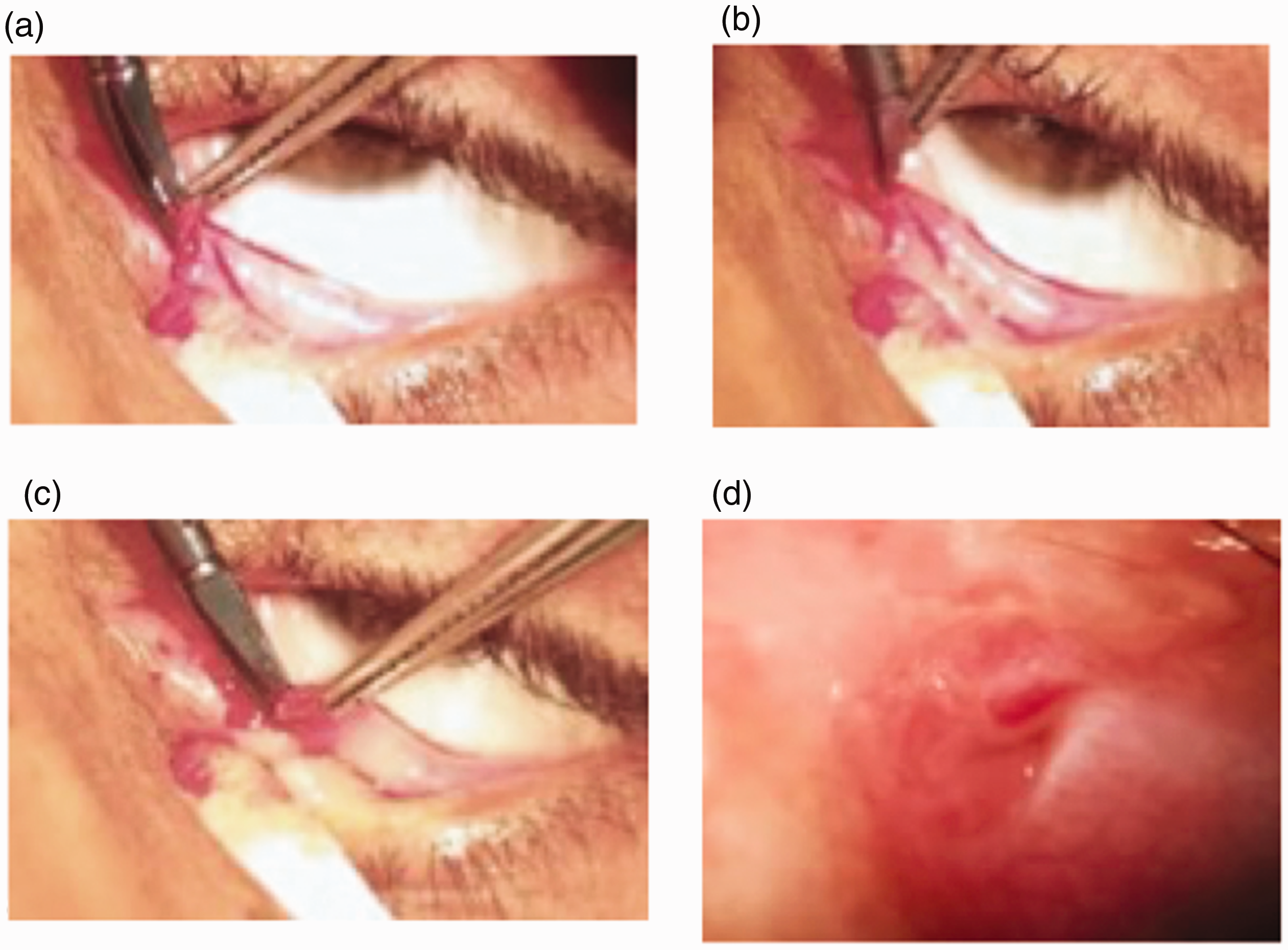
Three-snip punctoplasty: (a) first vertical snip, (b) second vertical snip, (c) third horizontal snip, and (d) at the end of punctoplasty.
Statistical analysis
Data were collected, coded, and entered in a PC for statistical analysis using the Statistical Package for the Social Sciences (SPSS: statistical package, version 20, IBM Corp, Armonk, NY, USA). For descriptive statistics, mean and standard deviation (SD) were used for quantitative data; number (n) and percentage (%) were used for qualitative data; and Kolmogorov–Smirnov normality test was used to differentiate between parametric data and non-parametric data. For analytical statistics, independent sample t-test was used for analysis of quantitative data, and paired sample t-test was used for analysis of paired quantitative data. For all tests, probability (p) was considered significant if <0.05, highly significant if <0.01, and very highly significant if <0.001. Bivariate correlation analysis was used for association analysis. Correlation (r) was considered weak or no correlation if 0.00–0.24, fair if 0.25–0.49, moderate if 0.50–0.74, and strong if 0.75 or more.
Results
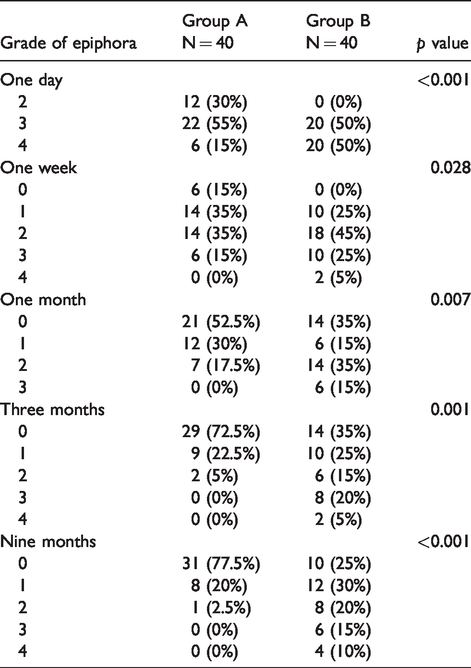
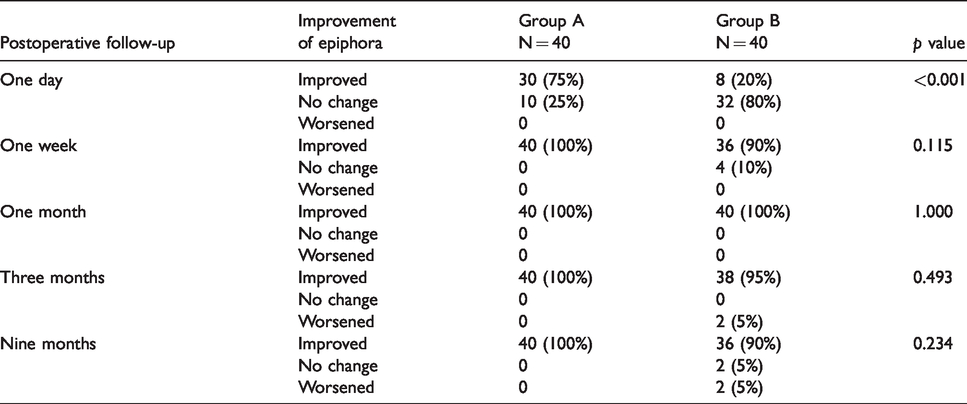
The mean age of the patients was 43.85 ± 14.93 (range: 17–67) years. Thirty patients (75%) were females, and 10 patients (25%) were males. Forty-six eyes (57.5%) had Grade 1 punctal stenosis, and 34 eyes (42.5%) eyes had Grade 2. Twenty-four eyes (30%) had epiphora Grade 3, and 56 eyes (70%) had epiphora Grade 4 with mean duration of 15.5 ± 13.4 months (range: 3–60 months). FDDT was Grade 3 in 72 eyes (90%) and Grade 2 in 8 eyes (10%). Postoperative grade of epiphora in both groups throughout the follow-up period is presented in Table 3. Improvement of epiphora grade at different points is presented in Table 4. There was a fair positive correlation between preoperative and final postoperative epiphora grade in Group A (p = 0.026 and r = 0.352). There was a negative fair correlation between the preoperative punctal stenosis grade and the epiphora grade postoperatively at the end of follow-up period in Groups A and B (p = 0.003, 0.044 and r = –0.462, –0.320), respectively. By the end of the follow-up period, in group A, FDDT was Grade 1 in 38 eyes (95%) and Grade 2 in only two eyes (5%). On the contrary, in Group B it was Grade 1 in 10 eyes (25%), Grade 2 in 24 eyes (60%), and Grade 3 in 6 eyes (15%). All eyes (100%) among Group A versus 21 eyes (52.5%) in Group B improved regarding FDDT grade (p < 0.001). FDDT and postoperative epiphora grade correlated positively after 9 months in both groups (p = 0.002 and r = 0.472) and (p < 0.001 and r = 0.887). In group A, foreign body sensation was felt in four eyes (10%) in the first postoperative day and this sensation disappeared after 1 week in all patients. In Group B, foreign body sensation and discomfort were described in 18 eyes (45%) in the first postoperative day, decreased to four eyes at 1 week and disappeared at 1 month. In Group A position, plug was found in place in 35 eyes (90%) in the first day postoperatively and rotated in four eyes (10%). Reposition was done on slit lamp. Early plug drop off occurred in only one eye within the first month. Restenosis after plug removal was not observed by the end of the follow-up period with normal size of the puncta (Figure 4(a)). In Group B, 36 eyes (90%) had dilated punctum (Figure 4(b)), while in four eyes (10%) with restenosis of the punctum with fibrosis at the surgical site was noticed by the end of the follow-up period (Figure 4(c)).
Postoperative grade of epiphora in both groups.
Postoperative improvement of epiphora.
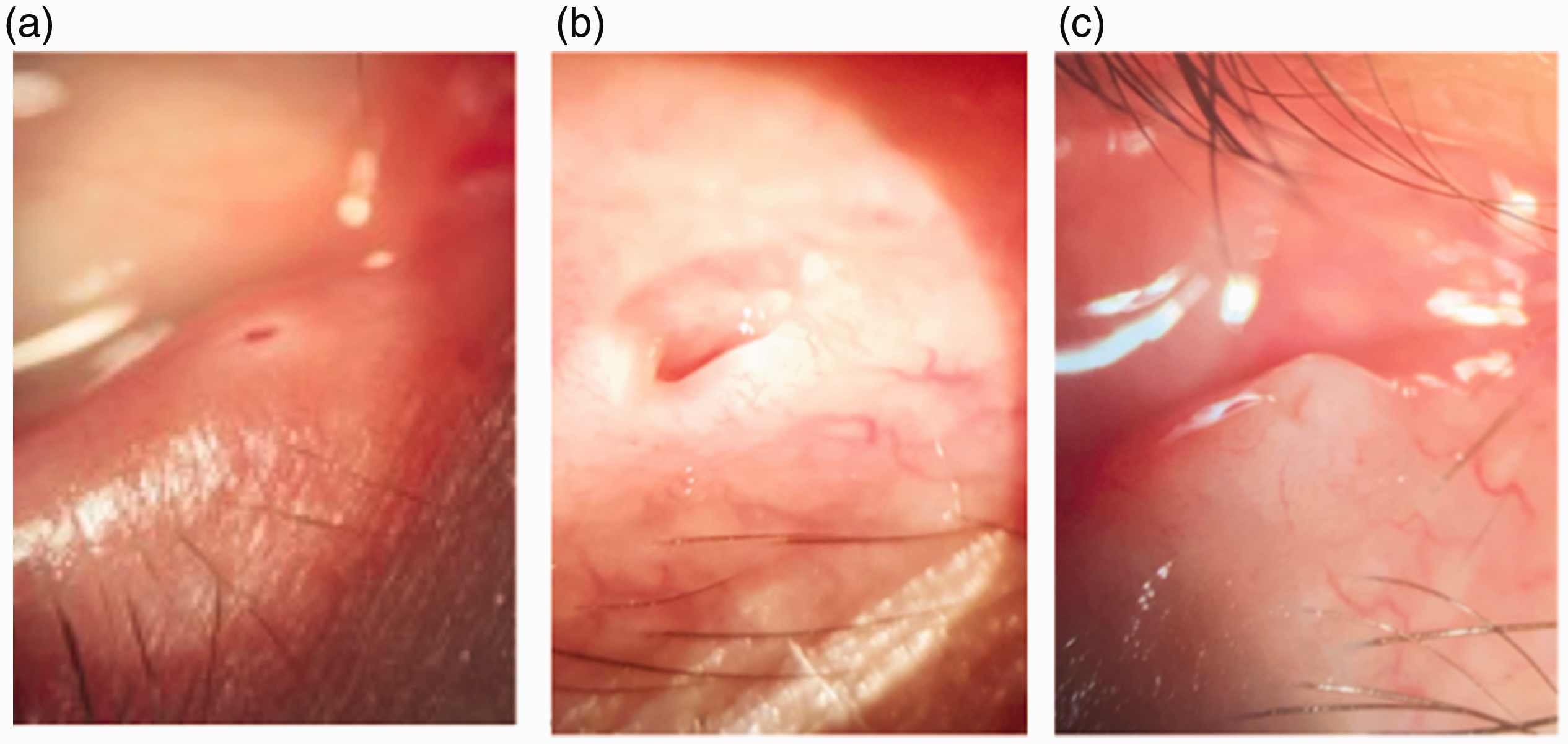
The punctum size at the end of the follow-up period: (a) normal size after plug removal, (b) dilated punctum after 3-snip operation, and (c) restenosis after three-snip operation.
Discussion
Punctal stenosis is a common cause of epiphora, and there are various methods to treat such codition. 13
This study is an interventional, prospective, comparative, and non-randomized study of 80 eyes with punctal stenosis distributed in two groups. Group A (40 eyes) was treated by insertion of PVP perforated punctal plugs in the lower punctum and Group B (40 eyes) was treated by rectangular three-snip punctoplasty of the lower punctum. The lower punctum is the main drainage site and responsible for 70% of tear drainage and all the procedures involving management of punctal stenosis usually performed through and confined to the lower punctum. Excluded patients were with allergic punctal occlusion as the condition is usually reversible and congenital punctal occlusion, as it may be associated with distal obstruction. In addition, patients with lid malposition, canalicular, nasolacrimal duct obstruction, those with previous eyelid or lacrimal drainage surgery, and untreated conjunctivitis or blepharitis were excluded, as these conditions could affect the surgical outcomes and may require special treatment.
Hur et al. 14 classified the grade of punctal stenosis, according to punctal morphology, into four types including membranous, slit, horseshoe, and pinpoint variants. In this study, the classification of Ozgur et al. 12 was used to grade punctal stenosis, as it relies on the size rather than the morphology of the punctum.
In Group A, plugs were retained in the lower punctum for 3 months with further 6 months follow-up period after plug removal. Konuk et al. 13 studied 44 eyes and removed the plugs after 2 months with mean follow-up period of 9 months. In addition, Chang et al. 15 and Malet et al. 16 removed the plugs after 2 months. On the contrary, removal of plugs was earlier in this study compared with that of El Ghafar et al., 17 who included 30 eyes with acquired punctal stenosis with adjuvant use of mitomycin-C, where the plugs were retained for 6 months with further follow-up period for 6 months after plug removal. In addition, Ozgur et al. 12 inserted perforated punctal plugs in 45 eyes and the plugs were explanted after 6 months with follow-up period ranging between 6 and 24 months. In Group B, the follow-up period was extended to 9 months postoperatively. Most of previous studies of three-snip rectangular punctoplasty, however, had 6 months follow-up period. 5 , 7 , 10 ,18–20 All eyes had epiphora Grade 3 or 4 according to Munk classification, 11 improved postoperatively to Grade 0 or 1 in 97.5% of eyes in Group A versus 55% of eyes in Group B by the end of the follow-up.
The results of Group A agree with those of Ozgur et al., 12 who had an improvement of epiphora score to 0% and 1 in 91.1% of the eyes 6 months after plug explantation. By contrast, they appeared better than those that of El Ghafar et al., 17 who reported disappearance of epiphora in 83.3% of eyes. This difference may be related to inclusion of cases with Grade 0 punctal stenosis (punctal atresia) in the study of El Ghafar et al. In addition, they defined postoperative success by epiphora Grade 0 versus epiphora grade 0 or 1 in this study and in that of Ozgur et al. 12 , 17 In addition, Chang et al. 15 had lower success rate of 85% which may be due to smaller sample size (20 eyes).
As regard to the anatomical results, in this study, plugs were found in proper position in 90% of eyes. Early rotation occurred 10% of eyes with simple reposition was done on slit lamp. Early plug drop off occurred in only one eye within the first month. Restenosis after plug removal was not observed during the follow-up period. This was in accordance with the study results of Ozgur et al., in which one plug dropped off spontaneously in 2 weeks. They had only two puncta (18.18%) and became stenotic again during the follow-up. However, the follow-up in their study extended to 2 years. 12 In Konuk et al.’s 13 study, three eyes demonstrated recurrent punctal stenosis. In Chang et al.’s 15 study, spontaneous plug loss was noted in four eyes between the first and second month follow-up examination. In El Ghafar et al.’s 17 study, two cases had extrusion of the plug. One case had granuloma formation that extruded from the lumen of the plug 2 months after surgery. Granuloma formation was not reported in this study.
In Group B, the improvement of epiphora score was higher than that of Chalvatzis et al., who compared three-snip punctoplasty in 16 eyes versus 16 eyes treated by modified three-snip punctoplasty with bicanalicular self-retaining stents. Complete disappearance of epiphora was noted in only two eyes treated by three-snip punctoplasty versus eight eyes which underwent modified three-snip punctoplasty with bicanalicular self-retaining stents. 19
Kim et al. evaluated the outcomes of rectangular punctoplasty in 45 eyes with punctal stenosis by the measurement of TMH using optical coherence tomography. They had functional success rate of 88.9% using Munk score and anatomical success rate of 93.3% with significant reduction of tear height at 6 months after surgery. 10 In addition, Caesar and McNab made a retrospective study of 53 cases with punctal stenosis undergoing posterior ampullectomy via three-snips. They documented 92% success rate. However, they defined success by any subjective improvement in epiphora. 5
Generally, the large variations in the success rates of three-snip punctoplasty may be related to the difference in the follow-up period as the incidence of restenosis is more likely to increase with time. In addition, there may be minor modifications or variations in the surgical techniques among different surgeons.
In this study, restenosis after three-snip punctoplasty was observed in four eyes (10%) due to fibrosis of surgical edge after follow-up 9 months. These results agree with those of Singh et al., who compared three-snip punctoplasty and monocanalicular intubation in 60 eyes with acquired punctal stenosis. They had punctal restenosis in nine eyes treated with three-snip punctoplasty versus only three eyes treated by monocanalicular intubation. 18
In this study, anatomical improvement was better than functional improvement. Similar results were documented by Ali et al., who performed rectangular three-snip punctoplasty in 145 puncta of 87 eyes of 56 patients complaining of epiphora due to punctal stenosis with follow-up period for 6 months. Punctal restenosis occurred in 5.7% of treated eyes, whereas 10.3% of eyes had postoperative functional epiphora. 7 In addition, Chak and Irvine compared three-snip rectangular punctoplasty (49 eyes) and three-snip triangular punctoplasty (59 eyes) with follow-up period 8 days to 2.3 years. They observed that patients were symptomatic postoperatively despite patent punctum in 16.9% of eyes with triangular punctoplasty versus 10.2% of eyes, which underwent rectangular punctoplasty and the difference was not significant. 20 The less favorable functional results despite patent punctum may be explained by the invasive procedures of ampullectomy and canalicular incision disrupting mechanism. 18
The physiologic role of lacrimal punctum in tears drainage lies in maintaining positive pressure within horizontal canaliculus during eyelid closure and negative pressure during eyelid opening. Invasive procedures like three-snip punctoplasty leave the system open to atmospheric pressure, disrupting this normal physiological mechanism. 18 On the contrary, using the PVP-perforated plugs in this study keeps both the physiological mechanisms and the anatomical structures undisturbed.
On comparing perforated plugs with three-snip punctoplasty, plugs had better functional and anatomical results. Subjective improvement of epiphora using Munk score was better in Group A. In addition, FDDT indicated objective functional improvement. All eyes (100%) among Group A versus 21 eyes (52.5%) in Group B improved regarding FDDT grade with a very highly significant difference (p < 0.001).
The advantage of the perforated punctal plugs over the surgical procedure of three-snip punctoplasty is the preservation of the punctal fibrous ring during its insertion that causes minor trauma and decreases the process of fibrous wound healing. This could partly explain the widely reported reduced functional success with snip punctoplasty procedures compared with plugs implantation in spite of anatomically patent puncta. 13
As regard safety, both techniques were well tolerated with no intraoperative or postoperative complications apart from foreign body sensation that was felt in 10% of eyes in Group A and in 45% of eyes in Group B during the early postoperative period and disappeared after 1 week and 1 month, respectively. Plug insertion was done using topical anesthesia while infiltration anesthesia was used for punctoplasty which makes the procedure a little invasive. Finally, extra cost was needed for punctal plugs compared to punctoplasty.
Limitations of this study include the relatively small sample sizes and the relative short follow-up with lack of long-term evaluation.
Conclusion
Both perforated punctal plugs and three-snip punctoplasty are safe and effective in treatment of acquired punctal stenosis. However, perforated punctal plugs are less invasive, better tolerated, and have superior and more stable results compared to three-snip punctoplasty.
Footnotes
Authors' note
This work has been accepted and orally presented in the 38th annual meeting, ESOPRS 2019, Hamburg, Germany.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.