
Abstract
Introduction
The Epstein–Barr virus is a rare causative pathogen identified in the posterior segment. The majority of cases were presented with a serious condition of acute retinal necrosis, and most of these eyes had poor outcomes. The clinical features and effective treatment options for this condition are still unclear.
Conclusion
Epstein–Barr virus is rarely identified as a sole pathogen in retinitis. Peripapillary predilection might be another type of presenting feature apart from the more-commonly reported peripheral acute retinal necrosis.
Introduction
The Epstein–Barr virus (EBV) is a double-stranded DNA virus from the Herpesviridae family and infects around 90% of the adults worldwide. 1 Acute infection is usually subclinical or presents as infectious mononucleosis. After the primary infection, the EBV resides in the memory B-cells and becomes latent. The carriers hold a lifelong risk of reactivation, which usually occurs when their immunity is compromised.
Although there is a high prevalence rate of EBV infection, eye conditions related to EBV infection are less commonly reported. 1 In the posterior segment, it is even rarer to be identified as the causative pathogen. The majority of cases were presented with a serious condition of acute retinal necrosis (ARN), and most of those eyes did not regain useful vision after treatment.2,3 We report a case of an immunocompromised child presenting with EBV-related retinitis, who had improved visual acuity after intravitreal and systemic antiviral administration.
Case description
Written informed consent from the patient and his parents was obtained for identifiable health information present in this case. A 10-year-old boy was diagnosed with acute myelomonocytic leukaemia 4 years ago and had received chemotherapy and hematopoietic stem cell transplantation. He achieved remission after the transplant, but a relapse was diagnosed 3 years later and 2 months ago he received a second haematopoietic stem cell transplantation. He was receiving an ongoing immunosuppressive regimen with cyclosporine and was targeted at a trough level of 200–400 ng/mL. No related ocular history was reported.
He had fever 2 months ago when the cyclosporine trough level reached 1015 ng/mL. His white blood cell count dropped and absolute neutrophil count lowered to 1743/µL. The quantitative blood polymerase chain reaction (PCR) was positive for cytomegalovirus (CMV) DNA (57,854 copies/mL; Figure 1). Intravenous ganciclovir and intravenous CMV immunoglobulin were given and his fever subsided. One month later, blood PCR exam showed undetectable CMV viral load. However, fever recurred and the blood PCR became positive for EBV DNA (42,898 copies/mL), and negative for herpes simplex virus (HSV) DNA and varicella zoster virus (VZV) DNA. Intravenous acyclovir was therefore given and the fever subsided. At this time, he started having a complaint of blurred vision in the left eye for 2 weeks.
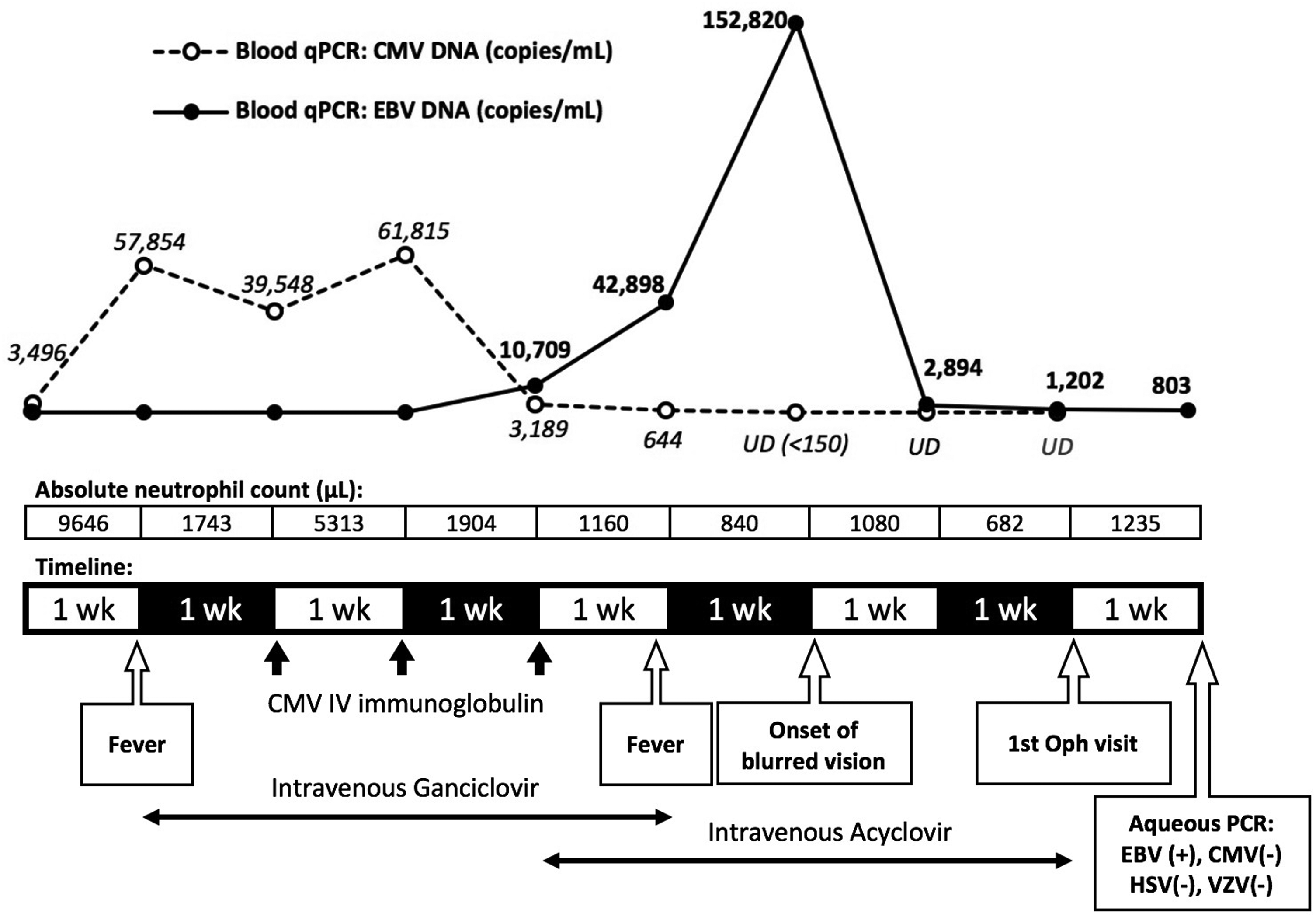
Clinical course and laboratory data. The patient was under immunocompromised state as shown by the absolute neutrophil count. He had fever 2 months before ophthalmic visit and was diagnosed of CMV reactivation based on elevated blood CMV DNA by PCR test. IV ganciclovir and CMV IV immunoglobulin were given and the blood CMV DNA count decreased to undetectable. However, fever recurred and the blood EBV DNA count became highly elevated and he started to have blurred vision. Aqueous PCR showed positive EBV DNA and negative for CMV, HSV and VZV DNA.
His best-corrected visual acuity was 20/20 in the right eye and counting fingers in the left eye. In the left eye, slit-lamp biomicroscopic examination showed 1+ cells in the anterior chamber without keratic precipitates or hypopyon. There was mild vitritis, and fundus examination revealed disc edema, diffuse retinal exudates, and retinal haemorrhages (Figure 2(a)). Spectral-domain optical coherence tomography (SD-OCT) showed subretinal and intraretinal hyperreflective materials and loss of the foveal external limiting membrane and ellipsoid zone/interdigitation zone (Figure 2(b)). The right eye was unremarkable except for a mild tortuous retinal vascularity.
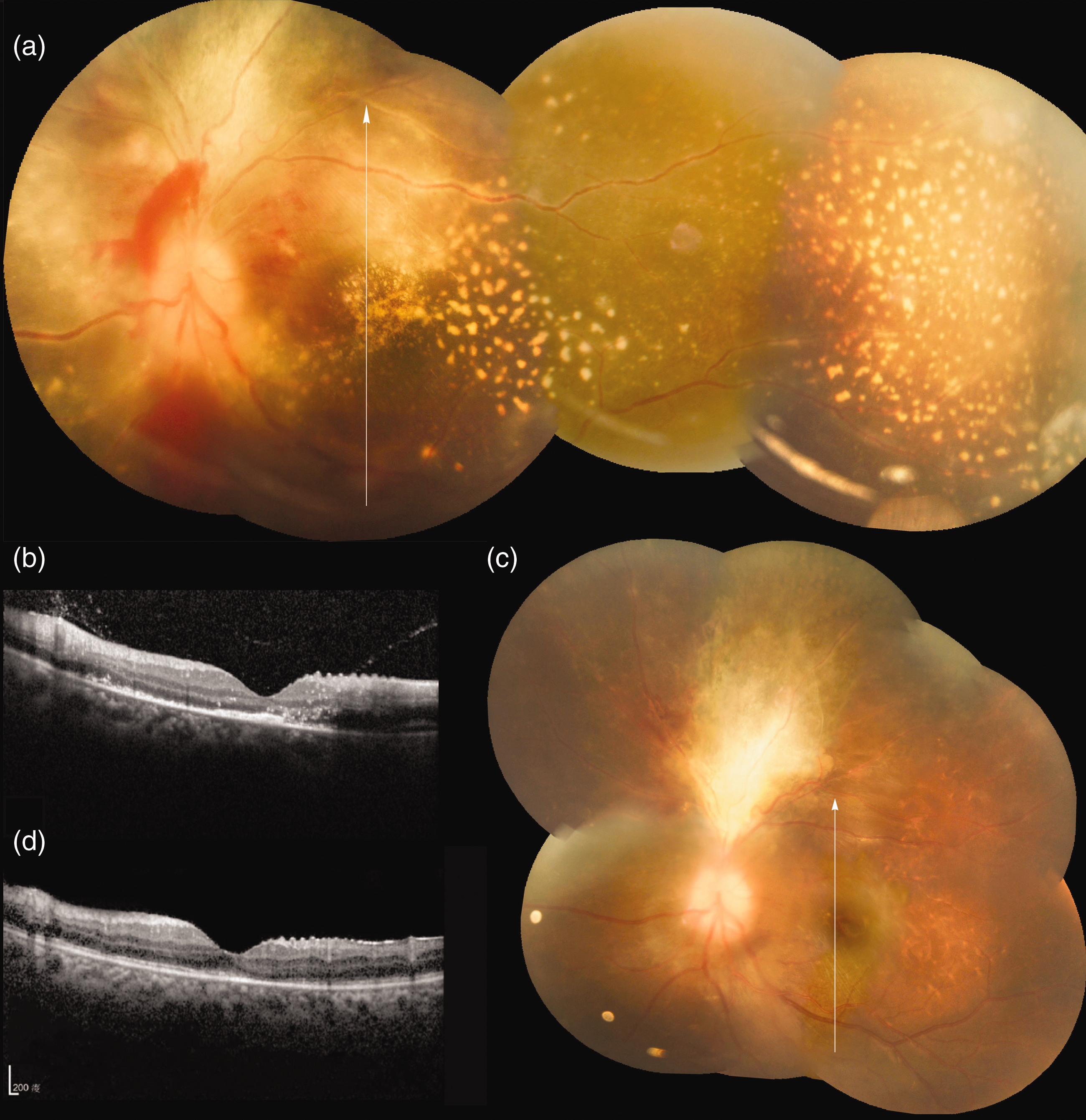
(a) Fundus photograph shows disc swelling, diffuse hard exudates, and retinal and preretinal haemorrhages. The arrow indicates the orientation of the spectral-domain optical coherence tomography (SD-OCT) image. (b) SD-OCT image shows subretinal and intraretinal hyperreflective materials and loss of the foveal external limiting membrane and ellipsoid zone/interdigitation zone (EZ/IZ). (c) Seven months after antiviral treatment, the fundus photograph shows some retinal fibrosis at the superior quadrant. The arrow indicates the orientation of the SD-OCT image. (d) SD-OCT image demonstrates partial restoration of the foveal external limiting membrane and EZ/IZ.
Due to the previous history, viral-related retinitis was suspected; therefore, intravitreal ganciclovir injection (2 mg/0.05 mL) and intravenous acyclovir were administered. Aqueous humour PCR showed positive for EBV DNA but negative for CMV, HSV and VZV DNA. After the antiviral treatments, disc swelling, diffuse exudates, and retinal haemorrhages gradually resolved. Seven months later, there was some retinal fibrosis (Figure 2(c)), and the SD-OCT scan showed partial restoration of the outer retinal layers (Figure 2(d)). His visual acuity improved to 20/500.
Conclusion
EBV can cause conjunctivitis, keratitis, episcleritis, dacryoadenitis, uveitis, optic neuritis and retinitis. 1 However, due to the limited amount of cases, the nature of EBV ocular infection remains unclear. PCR techniques have become increasingly popular to identify previously undetectable pathogens from small sampling volumes of aqueous or vitreous. However, ocular infection solely attributable to EBV is rare; often, there is co-infection with other agents such as HSV or VZV. A recent report showed that among the 12 reported EBV-related ARN cases, only five of them were exclusively EBV positive either by PCR or fluorescence in-situ hybridization for the aqueous or vitreous samples. 2
While most of the EBV-related posterior segment infection presented as peripheral ARN, several cases showed early posterior involvement.3,4 The presenting features included disc involvement, macular retinitis, and vasculitis of the arcades. As EBV-related uveitis was also shown to be more severe in the peripapillary region, a peripapillary predilection of EBV intraocular infection was suggested as another presenting feature apart from the typical peripheral ARN. 3 This was evident in our patient, where the most prominent exudates and retinitis were located in the posterior pole, and the optic nerve head was also involved.
EBV-related ARN also tended to be more fulminant than VZV- or HSV-related ARN. 2 This feature, compounded with posterior pole involvement, was the likely reason that in most reported cases the vision did not improve after treatment. In contrast, there was improvement in visual acuity seen in our patient soon after intravitreal ganciclovir injection, despite the fact that there was posterior pole and optic disc involvement.
For an immunocompromised patient with retinal necrosis, exudations and haemorrhages, CMV is the commonly suspected aetiology. CMV retinitis was most commonly seen in acquired immune deficiency syndrome patients, but with the advances in highly active antiretroviral therapy (HAART), proportionally more CMV retinitis cases are now found in patients receiving chemotherapy or immune suppression therapy. Our patient was immunocompromised and had recent systemic CMV infection, which greatly raised the risk of CMV retinitis. However, it was demonstrated that the sensitivity and specificity of using aqueous PCR to detect active CMV retinitis in acquired immune deficiency syndrome patient was as high as 93.5% and 100%, respectively. 5 Also, an undetectable plasma CMV DNA in PCR likely excludes CMV end-organ diseases. 6 Our patient had undetectable CMV DNA in PCR in both blood and aqueous specimen at the time of ophthalmic presentation. This was also true of the HSV and VZV testing. The exclusive positive results for EBV DNA in both blood and aqueous strongly supported his concurrent systemic and ocular EBV infection. In addition, the onset of ocular symptoms coincided with the time of maximal plasma EBV viral load (152,820 copies/mL; Figure 1), and at that time, the CMV viremia was already resolved. Nevertheless, it is still possible that the fundus presentation and symptoms were partly caused by CMV intraocular infection, but the viral load had already become undetectable after initial treatment.
In terms of treatment, effective treatment for EBV retinitis is still unclear. In-vitro studies had shown that both acyclovir and ganciclovir inhibit EBV replication. 7 Clinically, acyclovir significantly decreases viral shedding in the oropharynx in infectious mononucleosis, but has no effect on disease duration.8,9 As for EBV retinitis, among the reported cases some were treated with systemic acyclovir/ganciclovir, often with additional intravitreal antiviral injection due to its more aggressive nature. 2 However, non-responder with subsequent vitrectomy was needed in many cases and the outcomes were poor. 2 When our patient presented with ocular symptoms, our initial clinical impression was CMV infection, and we proceeded to inject intravitreal ganciclovir on the day of aqueous tapping. We speculate that the timely intravitreal injection and the fact that the patient was already under systemic acyclovir treatment for EBV viremia were the reasons for the relatively successful treatment. Two other cases were recently reported to have vision improvement after therapy. One improved after vitrectomy without any antiviral agents, 4 and the other was initially non-responsive to systemic ganciclovir or acyclovir, but improved after intravitreal methotrexate. 10 While our case provided more insight into this condition, the characteristics and the appropriate treatment for EBV intraocular infection still await further investigation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.