
Abstract
Objective
To evaluate and compare the objective and subjective outcomes after the bilateral implantation of a diffractive bifocal and trifocal intraocular lens.
Methods
This is a case–control, single-center observational study which included 27 patients; 16 patients were implanted bilaterally with the bifocal AcrySof IQ ReSTOR+3.0D and 11 patients with the trifocal AT LISA tri 839MP. Uncorrected visual acuity at distance, intermediate, and near under mesopic and photopic conditions using ETDRS charts with 10% and 100% contrast, corrected distance visual acuity, and binocular defocus curve in photopic conditions; binocular contrast sensitivity under mesopic and photopic conditions for far and near distances were assessed. The Visual Function Questionnaire-25 questionnaire was used to assess patients' satisfaction. All the measurements were performed 6–24 months after cataract surgery.
Results
The ReSTOR group had better binocular uncorrected near visual acuity in photopic conditions with low and high contrast charts (p = 0.040 and p = 0.033, respectively), as well as in far contrast sensitivity measurement under mesopic conditions with a spatial frequency of 3 cycles per degree (p = 0.034). There was not a significant difference between the two study groups in uncorrected near, intermediate or distance vision under mesopic conditions. The AT LISA tri study group had better subjective outcomes.
Conclusion
Both intraocular lenses restore visual acuity after cataract surgery. The ReSTOR intraocular lens provides better objective outcomes than the AT LISA tri, although the latter provides better subjective outcomes. The relevance of this study is the evaluation of both objective and subjective outcomes.
Introduction
Multifocal intraocular lenses (IOLs) have been designed to reduce spectacle dependence after cataract surgery and have been gaining acceptance as a refractive surgical procedure for presbyopic patients in selected cases. Thus, results can no longer be measured solely by visual acuity at different distances (depth of focus), but just as importantly by quality of vision, which can be assessed in terms of contrast sensitivity (CS), perception of photic phenomena, and patient satisfaction with the use of validated questionnaires. 1 These outcomes depend on retinal and cortical processing, known as neuroadaptation, and usually show improvement over time.2,3 Therefore, long-term follow-up of patients implanted with multifocal IOLs is critical to better assess quality of vision and patient satisfaction.
Depending on their design, current IOLs provide different depths of field and visual outcomes for far, intermediate, and near vision. 4 The diffractive design is intended to produce constant light to the retina, independently from the pupil size, and newer models have been aiming to improve intermediate vision and reduce visual side effects such as halos and glare. 5 The version of the diffractive bifocal lens AcrySof ReSTOR IQ (Alcon, Novartis, Fort Worth, TX, USA) that reduced near addition from +4.0 D to +3.0 D helped improve intermediate visual outcomes. 6 The AT LISA tri 839MP (Carl Zeiss AG, Jena, Germany) is a diffractive trifocal IOL that provides near, intermediate, and distance visual correction with fewer visual side effects due to a design that creates an asymmetrical distribution of light between distance and near vision. 7
The aim of this study was to compare the long-term clinical outcomes and personal satisfaction with two different models of diffractive multifocal IOLs: one bifocal and one trifocal. A 6- to 24-month follow-up was determined in order to allow for adequate assessment of not only objective parameters, such as visual acuity for variable distances, but also for more complex neuro-visual functions that develop and improve over time, such as CS (objective), and subjective parameters such as photic phenomena and overall patient satisfaction.
Methods
This is a case–control, single-center observational study that investigates the clinical outcomes and personal satisfaction of patients after minimum 6 months of uneventful microincisional cataract surgery (MICS) with bilateral multifocal IOL implantation at Vissum Alicante. This study was approved by the ethics committee of our institution and was performed in compliance with the principles of the Declaration of Helsinki, written informed consent was obtained from each patient.
In total, 27 patients were included in the study. They were divided into two cohorts based on the model of implanted diffractive multifocal IOL: (1) 32 eyes of 16 patients with bifocal IOL AcrySof IQ ReSTOR+3.0D and (2) 22 eyes of 11 patients with trifocal IOL AT LISA tri 839MP. All surgeries were performed by the same cataract surgeon (JLA) using the MICS technique, which is a bimanual technique that is performed through <2 mm clear corneal incision, enabling the separation of irrigation and aspiration. 8 All surgeries were performed with topical anesthesia (2% preservative-free lidocaine). Two 1-mm paracenteses were made at 10 and 2 o'clock, intracameral mydriatic was used to dilate the pupil and dispersive viscoelastic (Viscoat, Alcon) was injected to protect the corneal endothelium, phacoemulsification was performed, with implantation of a posterior chamber IOL (cohesive viscoelastic-Provisc, Alcon- was used to keep the capsular bag open for IOL insertion). After injecting intracameral antibiotic, the main incision and paracentesis were hydrated and sealed.
Patients who performed intermediate distance daily activities (like using a computer) were implanted with a trifocal IOL, otherwise they were implanted with a bifocal IOL.
Initially, we analyzed the electronic medical records of patients who had undergone bilateral implantation of the two studied IOLs in our practice. The retrospectively collected data were obtained from records of a preoperative (30 days to 1 h before treatment) and two postoperative visits—at 1 month (3–6 weeks) and 3 months (10–14 weeks) after IOL implantation—which took place before the subject was enrolled in the study. We assessed: preoperative axial length, anterior chamber depth (ACD) measured with IOL Master 500 (Carl Zeiss Meditec), pre- and postoperative manifest refraction, photopic uncorrected distance and near visual acuity (UDVA, UNVA), corrected distance visual acuity (CDVA), slit-lamp biomicroscopy and Goldmann tonometry.
Inclusion criteria were uneventful bilateral cataract surgery and IOL implantation; postoperative UDVA of 20/25 or better in one or both eyes; age between 45 and 75 years; and 3 months or less interval of IOL implantation between eyes. Patients who underwent Nd:YAG laser posterior capsulotomy after cataract surgery could still be included. Exclusion criteria were unresolved posterior capsule opacification (PCO); clinically significant glaucoma, macular, or retinal pathologies; keratoconus or keratectasia; pregnancy or nursing; and abnormal examination results from slit lamp biomicroscopy, fundus exam, IOL Master, or topography. Subjects who met all inclusion and exclusion criteria and were voluntarily willing to participate in this observational study were then scheduled for a visit (prospective phase) 6–24 months after the surgery.
The scheduled study visit consisted on the completion of a self-administered patient satisfaction and spectacle independence questionnaire (30 days to 1 day before examination visit) and a complete ophthalmic examination to assess clinical, refractive, and visual outcomes.
The questionnaire contained questions from a standard validated questionnaire, the National Eye Institute 25-item Visual Function Questionnaire (VFQ-25) 9 with additional questions targeting the overall satisfaction, spectacle independence, IOL recommendation, visual comfort in dim light conditions, and patient's individual lifestyle and vision requirements. The examination included uncorrected distance (4 m), intermediate (80 cm), and near (40 cm) visual acuities (UDVA, UIVA, UNVA) under mesopic and photopic conditions using ETDRS charts with 10% and 100% contrast. Manifest refraction, corrected distance visual acuity (CDVA), binocular defocus curve in photopic conditions; binocular CS under mesopic and photopic conditions for far and near distances (Optec 6500 Visual Function Analyzer (VFA), Stereooptical, Chicago, USA), at spatial frequencies 1.5, 3, 6, 12, and 18 cycles per degree (cpd), and binocular CS under mesopic and photopic conditions with the Pelli-Robosn Chart. Binocular halo and glare testing with a computer-based simulator (Halo and Glare Simulator, Eyeland Design Network GmbH, Vreden, Germany). Slit lamp biomicroscopy, including fundus examination, assessment of IOL positioning, presence of capsular fibrosis, PCO, or any adverse events. In case an exclusion criteria (e.g. PCO) was observed during the examination visit (prospective phase), the patient could be replaced to complete the number of patients planned for the study, which was 10–20 patients in each group, based on sample size estimation for the primary end point: CS function.
The literature data comparing CS outcomes obtained under mesopic conditions with one of the studied IOL models (AcrySof IQ ReSTOR+3.0D) and with another model of diffractive trifocal IOL (FineVision Micro F, PhysIOL, Belgium) show a significant difference (p = 0.01) at a spatial frequency of 6 cpd. 10 Assuming similar CS outcomes for this study, a minimum number of 10 and a maximum of 20 patients per study cohort (group) was found to be the sample size needed to prove the primary study goal for one spatial frequency level of CS.
The primary study endpoint is to show a significant difference in mesopic CS outcomes between the two study cohorts.
The secondary study end points included overall patient satisfaction rate based on a specific self-administered questionnaire; spectacle independence (percentage of patients wearing glasses “some of the time” or “never”); and intermediate uncorrected visual acuity under mesopic and photopic conditions. For all the before-mentioned parameters, a significance level of p < 0.05 was considered to be statistically significant.
Statistical analysis
Statistical analysis was performed using the program R for Windows software. The mean values and standard deviations (SDs) were calculated for every parameter for preoperative and postoperative data and the values of the questionnaire, in accordance with the instructions of the RAND organization which developed the VFQ-25 questionnaire.9 Using the Kolmogorov–Smirnov test, the samples were checked for normal distribution. If parametric analysis was possible, Student's t-test for paired data was used, otherwise the Wilcoxon rank-sum test was applied to calculate the significance of differences between the two cohorts under investigation. In all the cases the same level of significance (p < 0.05) was defined to be statistically significant.
Results
All patients were Caucasian and matched for demographics and preoperative refraction (Table 1).
Demographics and preoperative refraction.
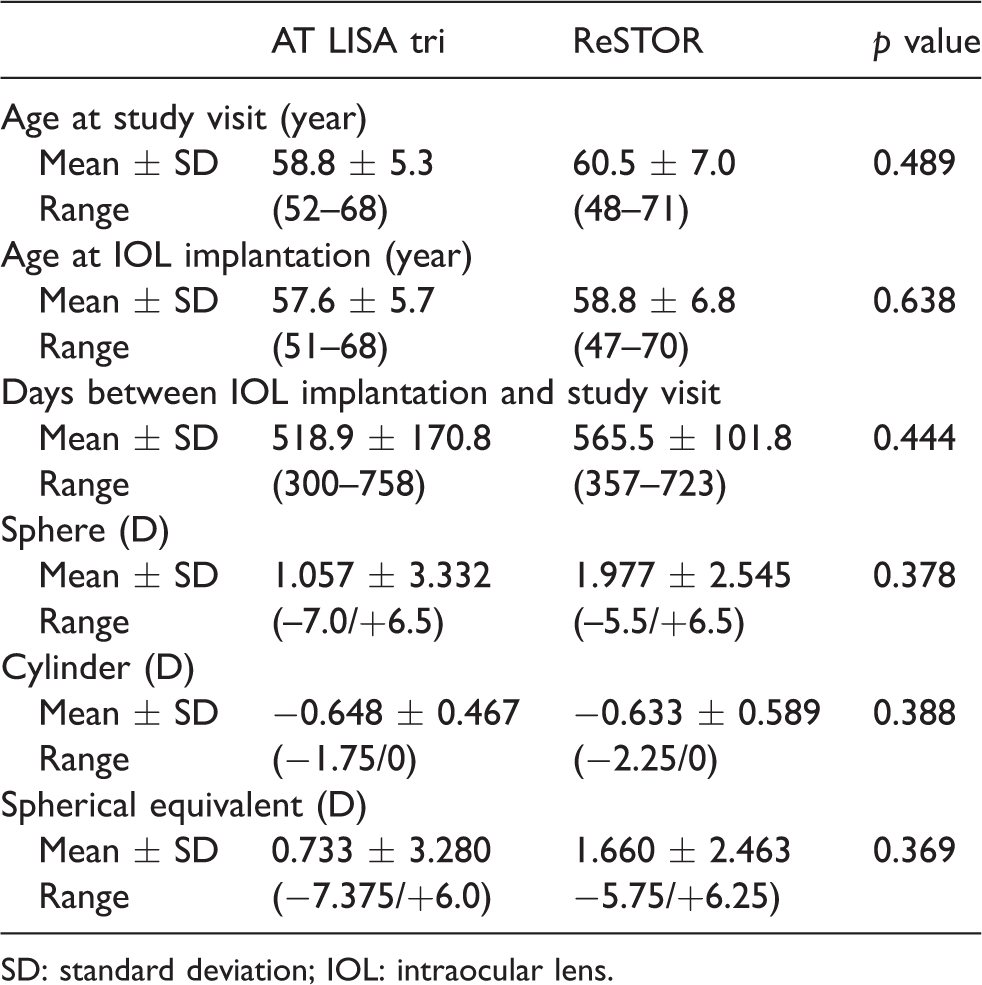
SD: standard deviation; IOL: intraocular lens.
There was no statistically difference between the two study cohorts in terms of biometric and demographic data, allowing an objective statistical comparison of the postoperative clinical results.
Preoperative monocular UDVA (LogMAR) was 0.677 ± 0.599 for AT LISA tri group and 0.585 ± 0.544 for ReSTOR group (p = 0.51). Preoperative monocular CDVA (LogMAR) was 0.023 ± 0.100 for AT LISA tri group and 0.009 ± 0.022 for ReSTOR group (p = 0.451). See Table 2 for the photopic binocular visual acuities at study visit.
Photopic Binocular Visual Acuities at study visit, ETDRS charts (LogMAR).
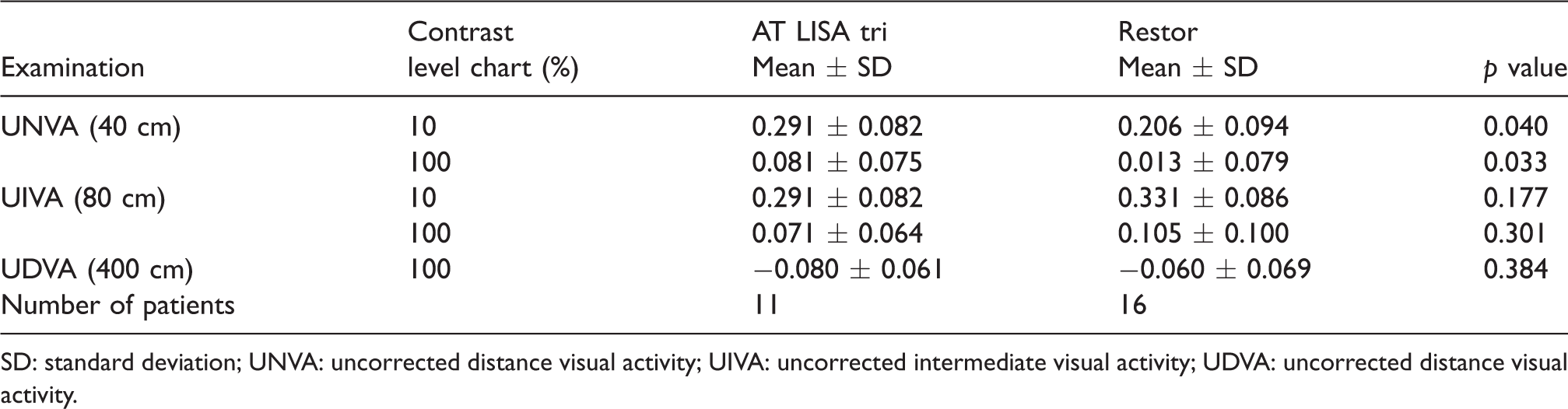
SD: standard deviation; UNVA: uncorrected distance visual activity; UIVA: uncorrected intermediate visual activity; UDVA: uncorrected distance visual activity.
Monocular UDVA improved significantly in both groups postoperatively (p < 0.01). At the study visit, objective measurements showed statistically significant differences between the two groups in UNVA in photopic condition with low (p = 0.04) and high (p = 0.033) contrast charts favoring the ReSTOR group, while no significant differences were found between groups in terms of UIVA or UDVA. Still regarding objective measurements, the ReSTOR group showed better far CS under mesopic conditions with a spatial frequency of 3 cpd (p = 0.034) measured with the Optec 6500. CS results with the Pelli–Robson chart show no significant differences between the two study groups (p = 0.356 under mesopic conditions, and p = 0.631 under photopic conditions).
Although the defocus curve did not show any statistically significant difference between the two groups (see Figure 1), a defocus of +1.5 D in photopic conditions at the study visit showed a marginally significant difference of binocular visual acuity (LogMAR) that was 0.378 ± 0.093 for AT LISA tri group and 0.485 ± 0.143 for ReSTOR group (p = 0.061).
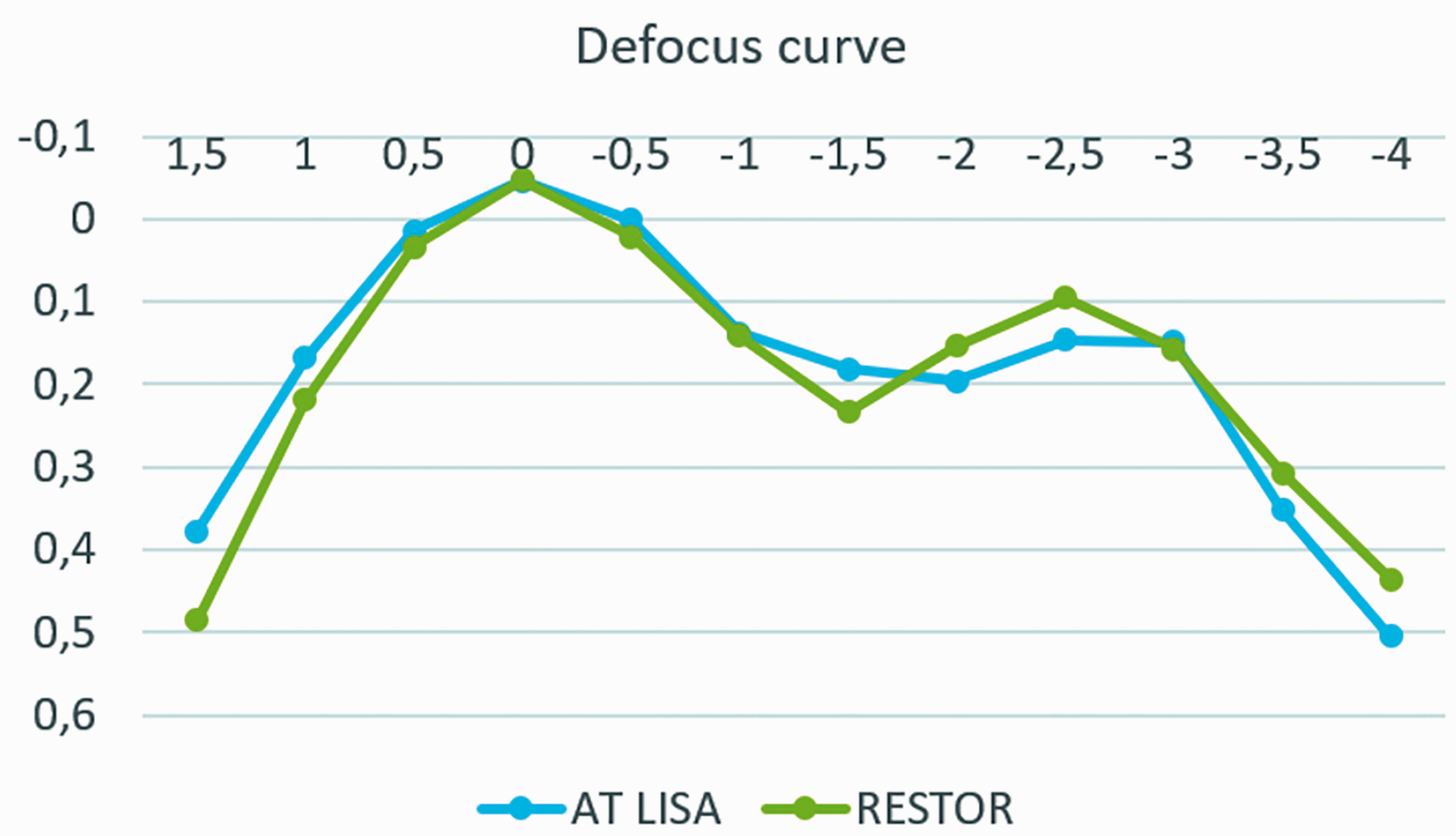
Binocular defocus curve of the AT LISA tri and Restor groups.
In contrast to the objective measurements, subjective outcomes measured by means of questionnaires showed better scores for the AT LISA tri study group (Tables 3 and 4), including overall patient satisfaction (p = 0.031), desire to choose the same IOL again (p = 0.015) (Table 3), and higher scores on all scales and subscales of the VFQ-25 questionnaire (Table 4).
Spectacle independence, IOL recommendation and overall satisfaction.
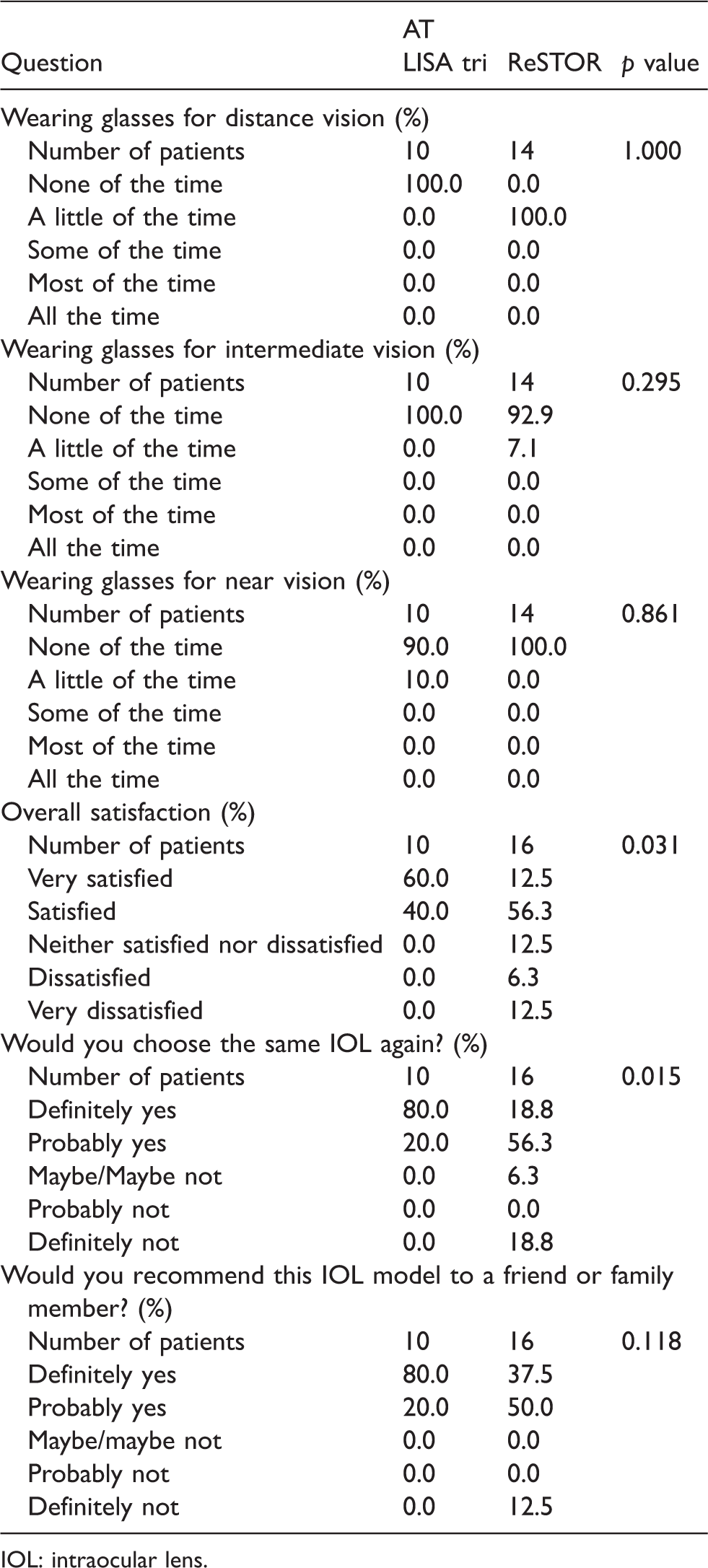
IOL: intraocular lens.
Outcomes VFQ-25.
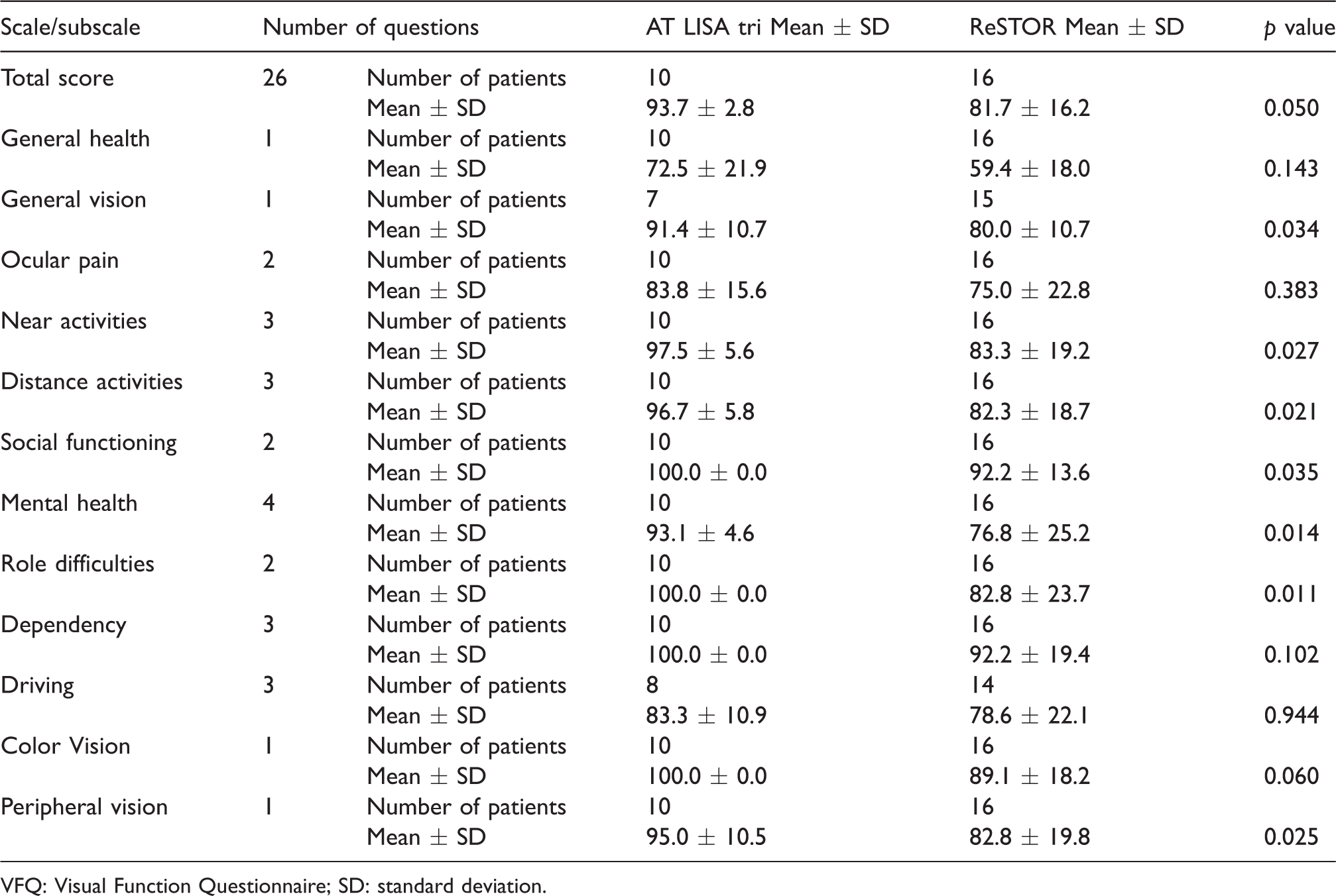
VFQ: Visual Function Questionnaire; SD: standard deviation.
The trifocal group had significant favorable outcomes in the following scales: peripheral vision, role difficulties, mental health, social functioning, general vision, total score, and near and distance activities.
Photic phenomena data measured with the halo and glare simulation software showed no significant differences between the two study cohorts.
Discussion
With this original study we decided to evaluate objective and subjective results after the implantation of a bifocal or trifocal diffractive IOL as there are many studies that focus either on the objective or subjective results alone,10–16 and we think that both results are equally important.
Regarding the objective measurements, we focused on CS as it is an important aspect in visual function. CS helps us in motion detection, dark adaptation, and visual acuity and it reflects visual perception in daily life better than standard acuity tests.16–18 We evaluated CS under photopic and mesopic conditions because after multifocal IOL implantation, patients complain more of visual symptoms under dim light conditions than under photopic conditions. 19 It has been reported with different multifocal IOLs that the visual acuity and CS is better under photopic conditions than under mesopic conditions.20,21
CS measured with the Pelli–Robson chart under mesopic and photopic light conditions showed no significant differences between the two groups, while the CS measured with the OPTEC 6500 showed significant differences under mesopic light conditions; this is because the tests measure CS differently; the Pelli–Robson measurement is in letters and the Optec 6500 is based on sine-wave charts, the latter has proved to be more sensitive than the systems providing letters. 22 The Pelli–Robson test has some drawbacks, such as fading of the print, unevenness of illumination, and reflections from the surface. 17 However, it is easy to use, quick, and repeatable. 23
Our CS results do not correlate with the ones we obtained in a previous study 16 in which we did not find any differences in low mesopic CS function measured with the same device (OPTEC 6500) between multifocal and monofocal IOLs (both IOLs that we studied in this article were included in the previous one). This might be due to the number of eyes that were greater in the previous study and the follow up time was longer in this study.
There was no significant difference in the intermediate uncorrected visual acuity under mesopic and photopic conditions and spectacle independence between both the groups. This finding correlates with a previous study of our group 20 where the ReSTOR SN6AD1 and the AT LISA tri did not have differences in intermediate vision, which means that the bifocal IOL achieves good intermediate vision.20,24
We previously reported 25 that photic phenomena like glare and halos have a major impact on patient quality of life after the implantation of multifocal IOLs. Our results did not show a significant difference between the two groups; this result correlates to our previous findings. 20 Law et al. 26 reported an important reduction in photic phenomena 6 months after the implantation of the AT LISA tri IOL, which means that neuroadaptation plays a major role in the perception of photic phenomena.
Regarding patients' satisfaction, all significant outcomes showed favorable outcomes for patients implanted with the trifocal IOL. We think that these outcomes correlate with spectacle independence; 100% of the patients with the bifocal IOL reported wearing glasses a little of the time for distance vision, while none of the patients with the trifocal IOL reported wearing glasses for distance vision and they were significantly more satisfied with their distance vision than the bifocal group. For near vision, 10% of the trifocal IOL group had to wear glasses for a brief period of the day, while none of the patients in the bifocal group had to wear glasses. The bifocal IOL group reported having difficulty in performing daily activities like shaving, performing outdoor activities and seeing TV on the VFQ25 questionnaire. It seems that patients really value a good distance vision, and not being able to perform easily all these activities had a negative impact in their life.
Our subjective satisfaction results do not correlate to the ones we previously reported 20 in which we did not find significant differences in patients' satisfaction after the implantation of the AT LISA 809M, AT LISAtri 839MP and Restor SN6AD1. This could be explained by the different questionnaires that were used. In our previous study we evaluated the patients with an in-house questionnaire, and in this study we evaluated them with a validated questionnaire (VFQ25).
Other authors 27 reported similar subjective satisfaction results between bifocal and trifocal IOLs. This finding could be explained because the patients in the trifocal IOL group were younger and they might have had higher expectations than the patients in the bifocal IOL group.
Due to the increasing patient demand for spectacle independence, more multifocal IOL models have been developed in order to achieve higher patient satisfaction; these include trifocal IOLs, varifocal IOLs, and extended depth of focus IOLs. Although bifocal IOLs achieve good objective outcomes, trifocal IOLs achieve good objective and subjective outcomes, 5 and at least in our clinical practice are the ones that are most commonly implanted. Considering the subjective outcomes, it seems that the trifocal IOLs have surpassed the bifocal IOLs, considering that 12.5% of the patients on the bifocal group were very dissatisfied with their outcomes and they would not recommend the IOL to a family member.
Although there were no significant differences preoperatively between the two groups, the fact that the bifocal IOL group had more patients than the trifocal group could be a limitation to our study.
To the best of our knowledge, this is the first study with a long-term comparison of both subjective and objective outcomes between a bifocal and trifocal IOL.
In conclusion, both IOLs provide good and stable restoration of visual acuity after microincisional cataract surgery in the long term. The bifocal group had slightly better visual outcomes for near vision and CS, while the trifocal group had higher patient satisfaction, with better performance of distance activities. Evaluation of both objective and subjective outcomes is equally important because a good objective outcome does not guarantee a good subjective outcome as we showed with this study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication has been carried out in the framework of the Red Temática de Investigación Cooperativa en Salud (RETICS), reference no. RD12/0034/0007 and RD16/0008/0012, financed by the Instituto Carlos III—General Subdirection of Networks and Cooperative Investigation Centers (R+D+I National Plan 2008–2011) and the European Regional Development Fund (Fondo europeo de desarrollo regional FEDER).