
Abstract
Purpose:
To describe a comprehensive OCT-based classification of myopic traction maculopathy (MTM).
Methods:
Two hundred eighty-one eyes with MTM (visited from 2006 to 2018), were retrospectively reviewed for age, best-corrected-visual-acuity (BCVA), axial length (AL), optical coherence tomography (OCT), and wide-field color fundus-photographs. The study was divided in two Phases. Phase 1: MTM types were categorized with OCT and correlated with age and BCVA. The type of staphyloma was described. Phase 2: the evolution of MTM was studied evaluating at least three OCT exams of each eye taken at different timings (interval between each exam: 1–10 years).
Results:
Phase 1: We identified, four MTM retinal stages (1. Inner/Outer Maculoschisis; 2. Predominantly outer Maculoschisis; 3. Maculoschisis-Macular Detachment; 4. Macular Detachment) and three foveal stages (a. Normal fovea; b. Inner Lamellar-Macular-Hole; c. Full-Thickness-Macular-Hole). Outer-Lamellar-Macular-Holes and epiretinal abnormalities were associated findings. Stages 1 to 2 were younger than stages 3 to 4 (p < 0.05). BCVA in stages 1, 2 was similar, and higher than stages 3, 4 (p < 0.02). About 14% of eyes had no staphyloma, 73% of eyes had staphyloma type 1 or 2. MTM stages were not correlated with AL. Phase 2: The retina could change in time from stage 1 to 4, or the fovea could change from stage a to c. Mean evolution time from stage 1 to 2, stage 2 to 3, and 3 to 4 were 20, 12, 3 months, respectively. BCVA decreased over time as stages increased (p = 0.47).
Conclusion:
The MSS Table displays a new classification, the natural evolution, and practical insights for the management of MTM.
Keywords
Introduction
Myopic maculopathy (MM) was recently classified by Ruiz-Moreno and colleagues. 1 They extensively analyzed the structural and functional changes of MM and proposed the ATN classification, based on three main pathological features: atrophy, traction, and neovascularization. Myopic traction maculopathy (MTM), as defined by Panozzo, 2 represents the tractional feature in the ATN triplet of MM, affecting 9–34% of eyes with MM.2 –4 MTM, however, is comprised of a wide spectrum of clinical pictures (maculoschisis, macular detachment (MD), inner, outer, or full-thickness macular holes) that potentially imply customized management decisions, and deserves a classification on its own. In the literature, descriptions of different and yet limited types of MTM may be found.2 –14 Shimada et al. 5 graded the retinoschisis (O-RS), which is one of the manifestations of MTM, based on the location and the size of the outer schisis.
A comprehensive classification of all MTM types with practical implications for the management of the disease has not yet been published. Additionally, detailed information regarding the evolution of MTM is not available. In early stages, MTM can be completely asymptomatic,6,7 and this is the main reason that limits the knowledge of the natural history and the pathogenesis of MTM. 8 Certainly, the availability of new OCT equipment allows a better detection of fine changes and early signs of MTM and might help not only in the definitions and classifications of the types, but also in the evaluation of the natural history.
Several authors have tried to delineate the signs of evolution from one type to another in small case series. It was shown that foveal detachment (FD) occurs after the formation of the maculoschisis and may precede the formation of a macular hole. 9 Shimada et al. 10 described different stages of the maculoschisis, leading to a FD, through the formation of an outer lamellar hole. Sun 9 described the formation of a macular hole from a schisis.
However, there is not yet a proposal of the evolution of each type of MTM as a whole, nor a clear indication of the timing of evolution.
The aims of the present study are:
To focus on the tractional changes of MM, and to list all the possible clinical pictures of MTM visible with commercially available OCT.
To analyze the evolution of the different types of MTM and to determine the time taken to evolve from one type to another. In other words, to determine whether we should consider each clinical picture not as a type but as a stage of evolution.
The final goal is to reach a comprehensive OCT-based classification of MTM with practical implication, that is able to offer information on the prognosis and management of the patients.
Methods
We retrospectively reviewed, from a clinical database, the available information of all of the patients affected by MM that were seen between January 2006 and February 2018, at the S. Anna Hospital in Brescia, Italy. The analysis of the data was performed in August 2018.
Data were collected on age (years), sex (male\female), eye (right\left), and decimal best-corrected visual acuity (BCVA). Axial length (AL) measurement was reported when available. All the images of the same eyes were retrieved from the database of the OCT machines, (Cirrus 3000, software version B 3.0, Carl Zeiss Meditec, Dublin, CA, USA; Cirrus®, AngioPlex Carl Zeiss Meditec Inc., Dublin, CA, USA; Triton® by Topcon, Tokyo, Japan; Spectralis®, Heidelberg Engineering, Germany), and color fundus photographs (CX-1, Canon Inc., Japan; Daytona®, Optos Inc., USA; Clarus 500®, Carl Zeiss Meditec Inc., Dublin, CA, USA).
The study had 2 phases. The first phase consisted in the observation of the OCT of both eyes of the patients in the whole group. Only OCT exams with at list the six radial scans of the posterior pole centered on the fovea and well visible were selected. This OCT exam was defined as “the final OCT.” All the eyes that underwent previous vitreoretinal surgery were excluded from this analysis.
This phase allowed to list all the possible OCT types of tractional changes that were found in the retina and in the fovea, and to make a correlation between the OCT (anatomical finding), the BCVA (functional finding), and the age (demographic finding) of the patient. Analysis of variance one-way Anova was used to compare the mean age among the MTM types. This analysis was followed by post-hoc Tukey–Kramer test for multiple comparisons. Two factors Anova analysis was used to compare the mean age among subgroups of MTM types.
A correlation was also made between the tractional changes visible at OCT-scan and type of posterior staphyloma in the same eye, according to Hsiang classification, 11 classified by judging the preoperative wide-field color fundus photo.
The second phase was focused on the observation of a selected subgroup of eyes from the whole series. These were eyes of patients that could provide at least two OCT exams, taken at different timings, at least 3 months prior to the final OCT which was taken at the time of the visit. The minimum acceptable time interval between the final OCT and the OCT taken just prior to the final one was 3 months. The acceptable time interval between two prior consecutive OCT exams was 6 months. All the eyes that underwent previous vitreoretinal surgery were excluded from this analysis.
This second phase allowed us to study the evolution of the disease in the same eye.
Six observers judged the imaging, by observing the same images twice, in order to study both an interobserver agreement and an intraobserver agreement.
The definitions of maculoschisis suggested by Benhamou et al. 4 were followed. We hereby provide the choices of glossary and terminology that were made in this study, in order to avoid any possible misinterpretation.
Schisis
Increased thickness of the neurosensory retina in a column-like structure. Since, in most cases, the schisis affected the whole macula and not just the fovea, and since it could be found not only in the fovea but also (or only) in the extrafoveal area (Figure 1), we avoided the term foveomacular schisis or foveoschisis and selected to use maculoschisis.
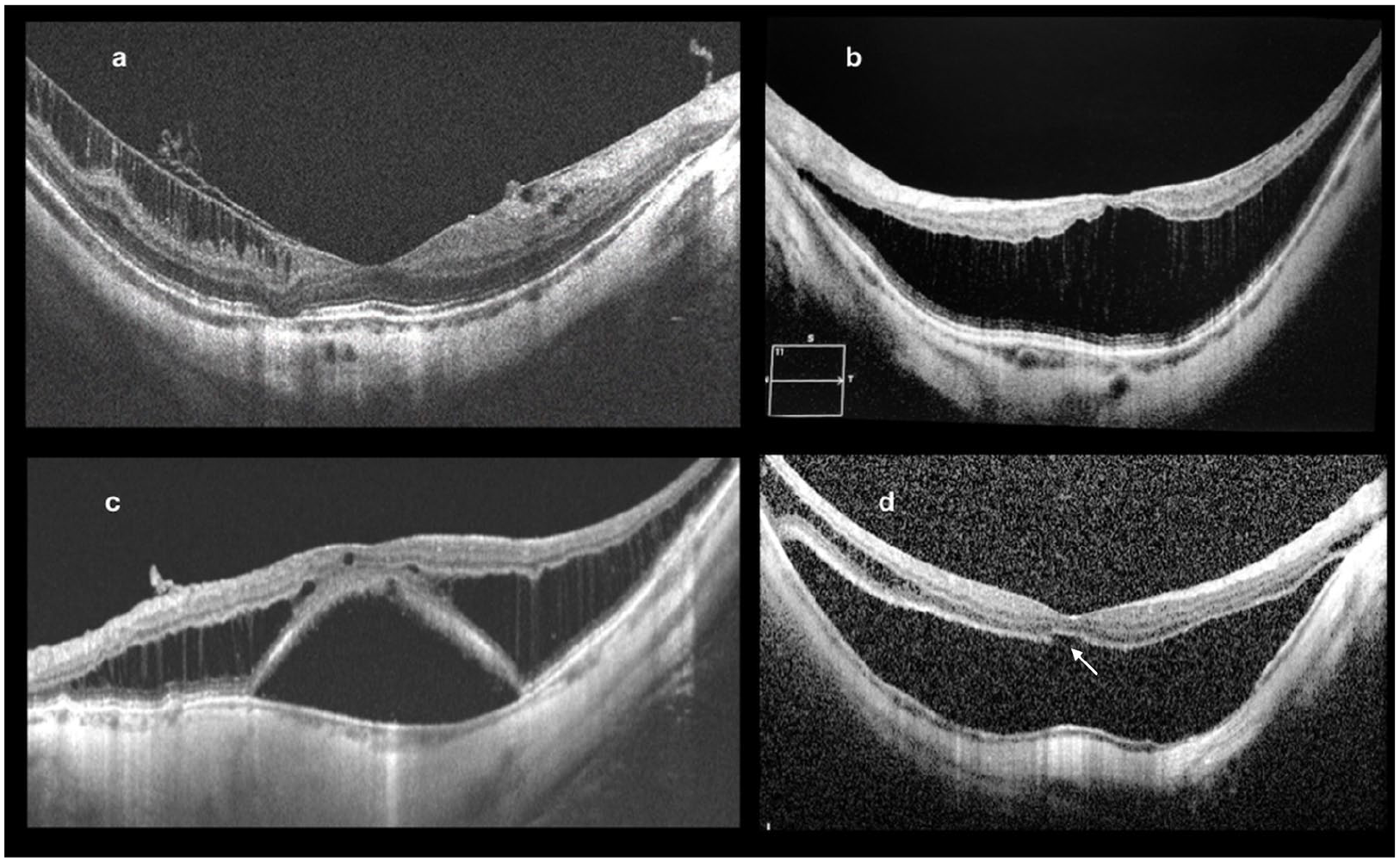
(a) Eye affected by MTM in the form of inner schisis (stage MSS 1a+) in a 44-year-old female. The OCT shows I-MS in the temporal extrafoveal area with epiretinal abnormalities and normal fovea. (b) Eye affected by MTM, in a 49-year-old female, in the form of predominantly O-MS involving the whole macula. Sign of inner schisis are not visible and the fovea is normal (Stage MSS 2a). (c) Eye affected by MTM in the form of maculoschisis and detachment (Stage MSS 3a). (d) Eye affected by MTM, in a 65-year-old female, in the form of MD involving the entire macula. Maculoschisis is no longer visible, except for the extreme temporal edge of the macula (Stage MSS 4a). An initial outer lamellar macular hole (O-LMH) is present (arrow).
Inner maculoschisis
Inner maculoschisis (I-MS) is a thickening of the inner retinal layers in a column-like structure, at different levels, from the inner nuclear layer to the ILM (Figure 1). The ILM can be detached from the nerve fibers layer and connected to it with a column-like structure.
Outer maculoschisis
Outer maculoschisis (O-MS) is a thickening of the outer retinal layers in a column-like structure (Figure 1), starting from the outer plexiform layer, that changes in a column-like structure, to the outer nuclear layer to the external limiting membrane.
Maculoschisis with MD
Association of maculoschisis and neurosensory detachment of the central macula (Figure 1) with separation of the photoreceptors from the retinal pigment epithelium (RPE).
Macular detachment
A neurosensory detachment of the macula with separation of the photoreceptors from the retinal pigment epithelium (RPE). The MD involves the whole macula with no areas of schisis visible (Figure 1). Occasionally the detachment may expand beyond the macula.
Inner lamellar macular hole
Inner lamellar macular hole (I-LMH) is a splitting of the inner foveal layers, developing from the internal limiting membrane (Figure 2) and not reaching the photoreceptors. The depth and width of the I-LMH may vary significantly but was not analyzed in the present study.
Evolution of MTM in a highly myopic eye of a female. (a) OCT scan, taken at the age of 53, shows O-MS in the macula with normal fovea (stage MSS 2a). (b) OCT scan, taken at the age of 55, shows O-MS in the macula with development of an I-LMH and visible epiretinal abnormalities (stage MSS 2b+). (c) OCT scan, taken 6 months after the previous one, shows O-MS with development of MD and FTMH (stage MSS 4c+).
Outer lamellar macular hole
Splitting and interruption of the photoreceptors (Figure 3). The width of the outer lamellar macular hole (O-LMH) may vary significantly but was not analyzed in the present study.
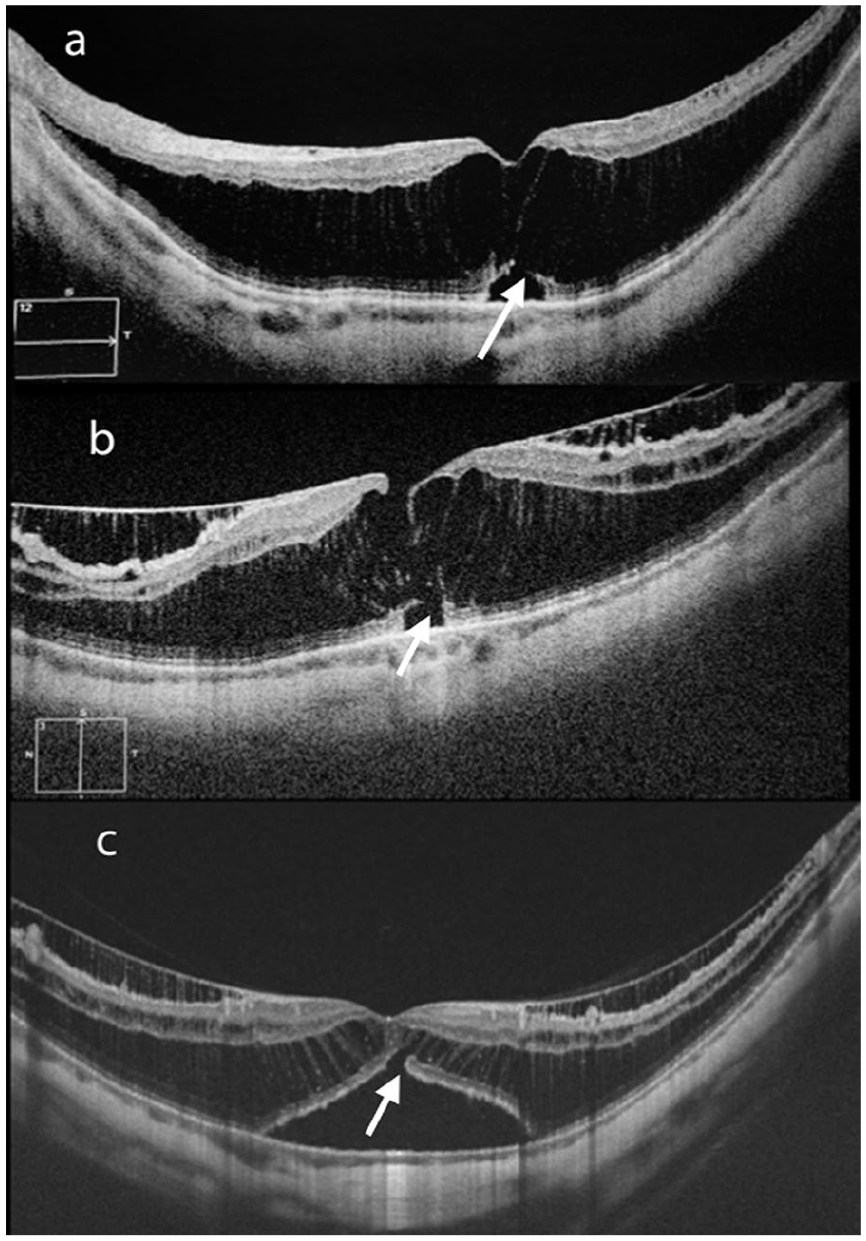
Eyes of three patients, affected by MTM, in the form of predominantly O-MS involving the whole macula (a) and (b) and in the form of schisis-detachment (c). In (a) and (c), the inner fovea is intact and there is an O-LMH (white arrow). In (b) there is an I-LMH and an O-LMH. There is not yet a full separation of the retina and a thin bridge of tissue is still visible between the I-LMH and the O-LMH. ((a) stage MSS 2aO; (b) stage 2bO+; (c) stage 3aO+).
Results
Phase 1
Three hundred and twenty-one eyes with MM were examined. Signs of MTM were found in 281 eyes of 157 patients. These eyes were divided according to types of MTM, based on the observation of the retinal pattern and of the foveal pattern, at the OCT scans.
From the original group of eyes with MTM, 52 eyes were excluded from the analysis because of the unacceptable quality of the imaging.
Table 1 shows the summary of data of the 229 eyes in phase 1 of the study.
Characteristics of patients studied in phase 1.
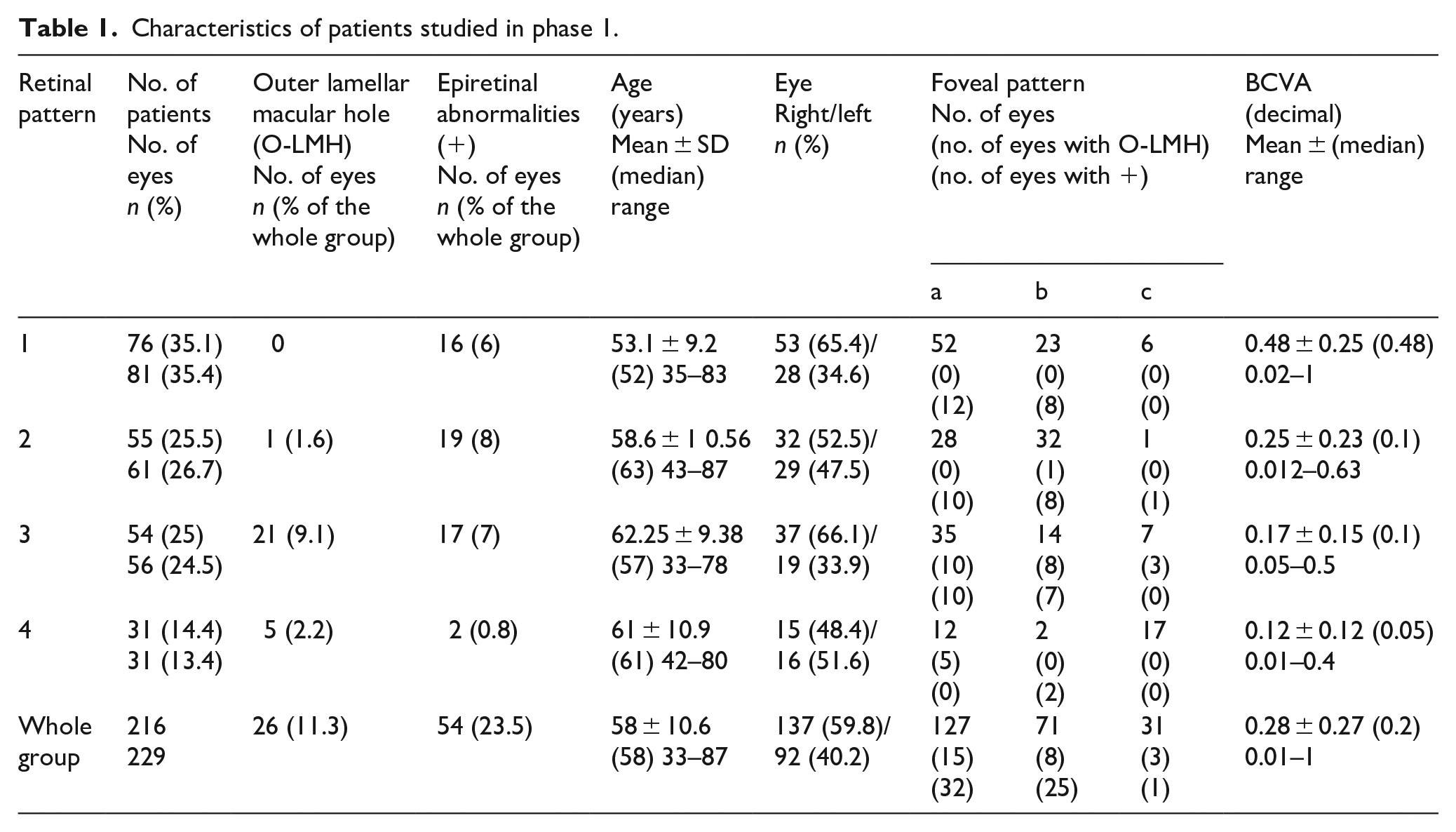
Four OCT retina patterns were identified, as follows: (1) inner macular schisis (I-MS) or inner and outer macular schisis (IO-MS); (2) predominantly outer macular schisis (O-MS); (3) macular schisis with MD; and (4) MD.
Three OCT fovea patterns were identified and could be associated with each retina pattern: (a) intact fovea; (b) inner lamellar macular hole (I-LMH); and (c) full-thickness macular hole (FTMH).
While epiretinal abnormalities, such as epiretinal membrane (ERM) or vitreoretinal traction (VRT) could be associated with each pattern, an O-LMH was present only in pattern 2, 3 (Figure 3), and 4 (Figure 1). Table 1 also shows the distribution of O-LMH and epiretinal abnormalities in different patterns.
The graph in Figure 4(a) represents the mean age of the patients for each type of retinal patterns. The difference between the age in retinal pattern 1, compared to retinal patterns 3, and 4, was statistically significant (p < 0.05). The graph in Figure 4(b) represents the mean age of the patients for each foveal pattern.
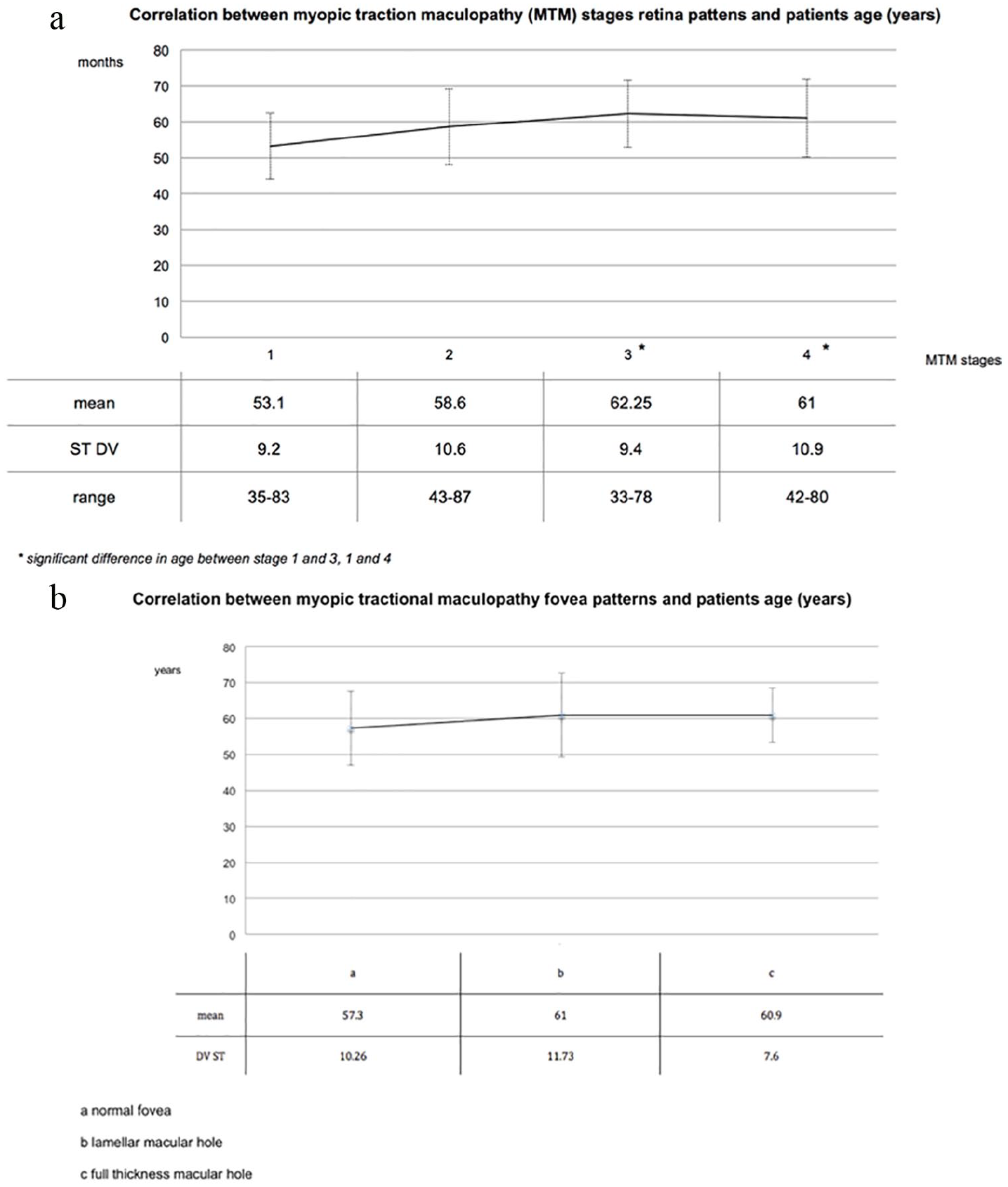
(a) The graph represents the mean age of the patients for each type of retina patterns 1, 2, 3, and 4. The difference between the age in pattern type 1 and 2 compared to pattern type 3 and 4 was statistically significant (p < 0.05). (b) The graph represents the mean age of the patients for each type of fovea patterns a, b, and c.
As displayed in Table 1, the mean BCVA in retinal patterns 1 and 2 were similar, while BCVA in patterns 3 and 4 were worse, although, in the statistical analysis (Tukey–Kramer test), the mean BCVA was significantly higher only in retinal pattern 1 compared to retinal pattern 3 and 4 (p < 0.05).
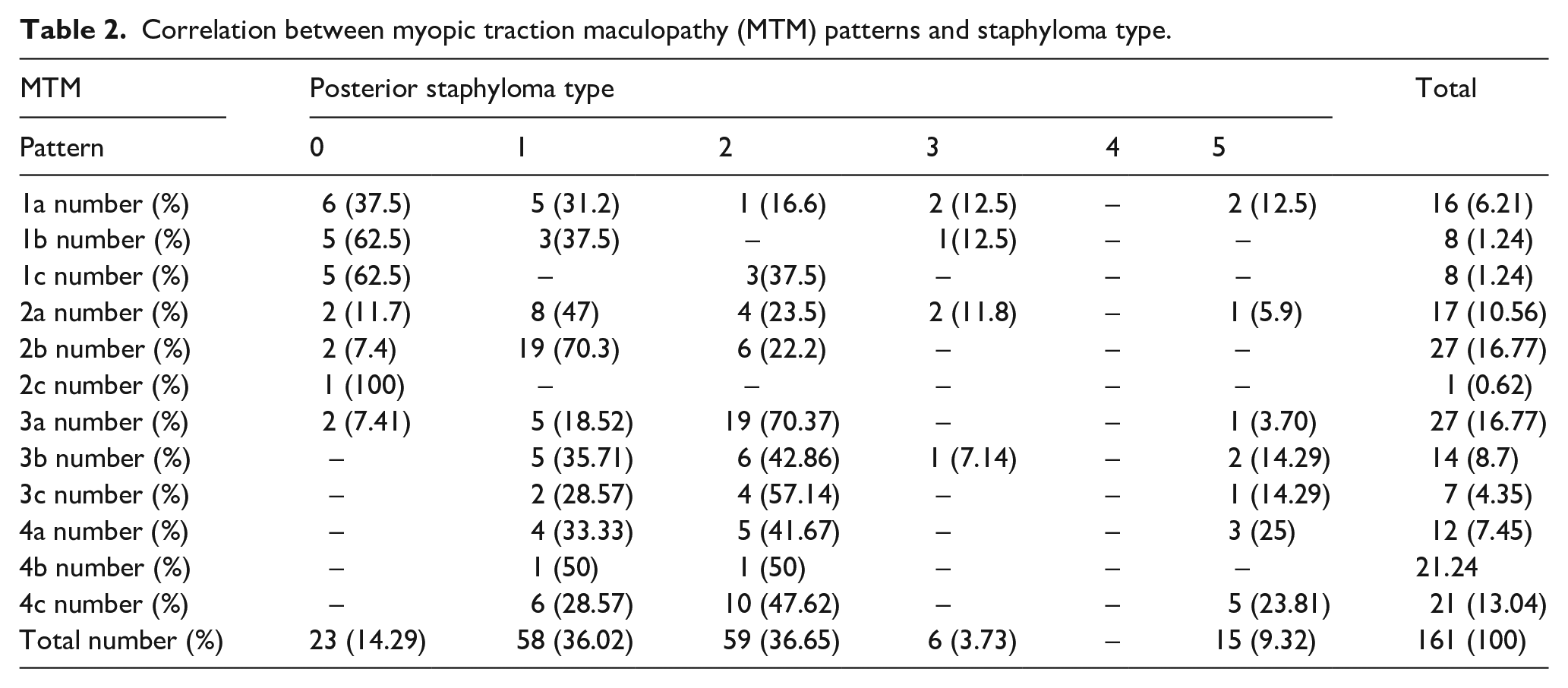
While the OCT was available for each eye, the wide-field color fundus photo to detect the presence of a staphyloma was available for a subgroup of 161 eyes. Among these, a staphyloma was not visible in 14% of the eyes. Eyes without a staphyloma showed OCT retinal patterns 1 and 2. In 138 cases (86%), MTM was associated with a posterior staphyloma (p < 0.05). The most represented staphyloma was type 1 (wide macula) in 36% and type 2 (narrow macula) in 37%. Staphyloma type 3 involving the peripapillary area was present only in 4% of eyes. Staphyloma type 5, involving the area inferior to the macula, was present only in 9% of eyes. The staphyloma type 4 (nasal) was not present in this series. Retinal patterns 3 and 4 were always associated with a staphyloma and mainly type 2.
The association between each type of OCT retinal and foveal patterns and the type of staphyloma is presented in Table 2.
Correlation between myopic traction maculopathy (MTM) patterns and staphyloma type.
No statistically significant correlation between retinal patterns and AL was found. Considering all eyes in the groups, an AL comprised between 26.12 and 37.54 mm almost evenly distributed per each OCT pattern.
Phase 2
For 72 eyes, at least three OCT taken at different timings were available. Four OCT exams were available for 20 eyes. Five for 12 eyes. Six for five eyes.
The time interval between each OCT ranged from 3 months to 2 years. The range between the first and last available OCT ranged from 2 years to 9 years.
We observed that the retina could change from pattern 1 to 2 to 3 to 4 (Figures 2 and 5), and\or that the fovea could change from pattern a to b to c (Figures 2 and 6). The changes in the retinal and foveal patterns could manifest simultaneously or separately.
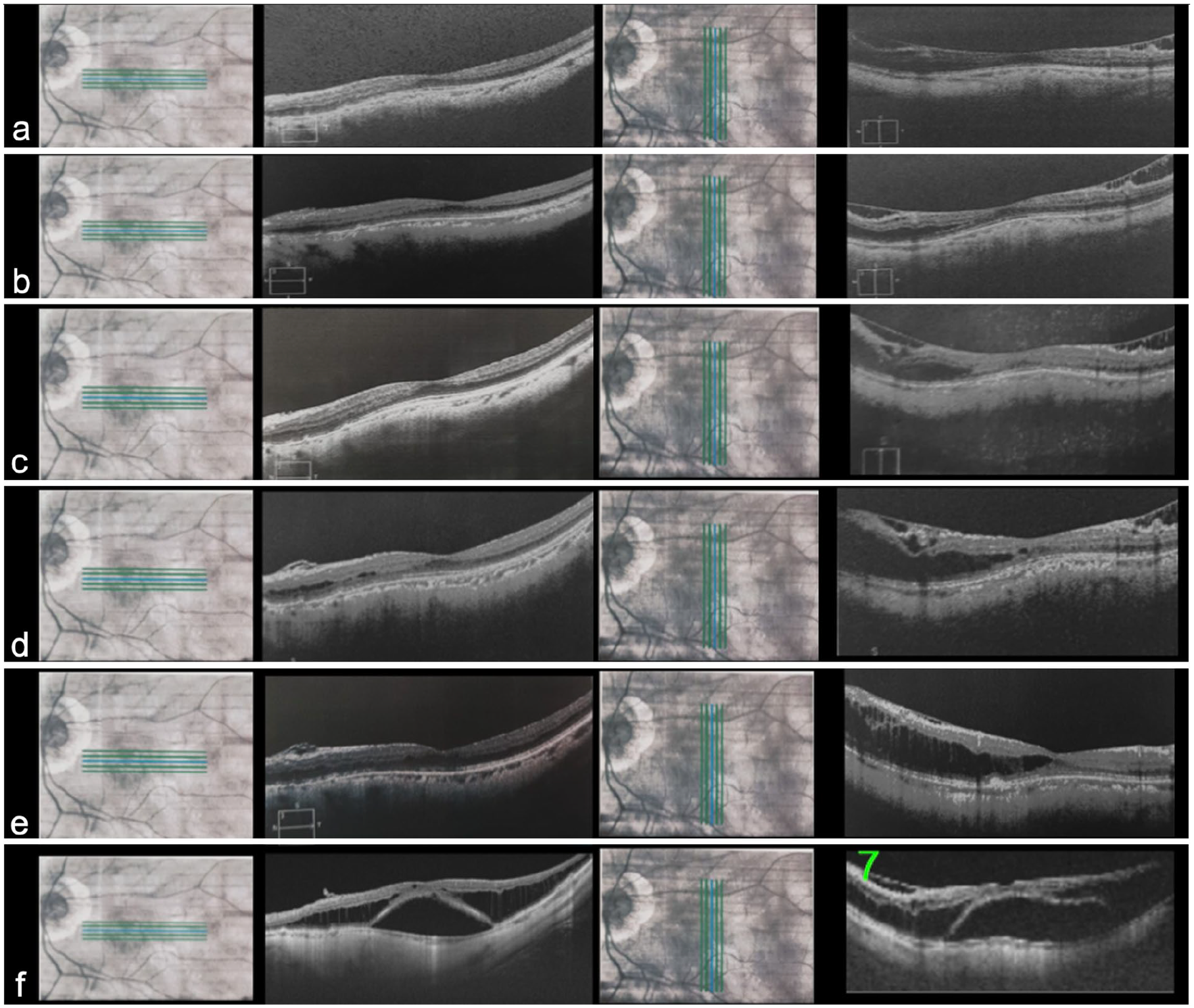
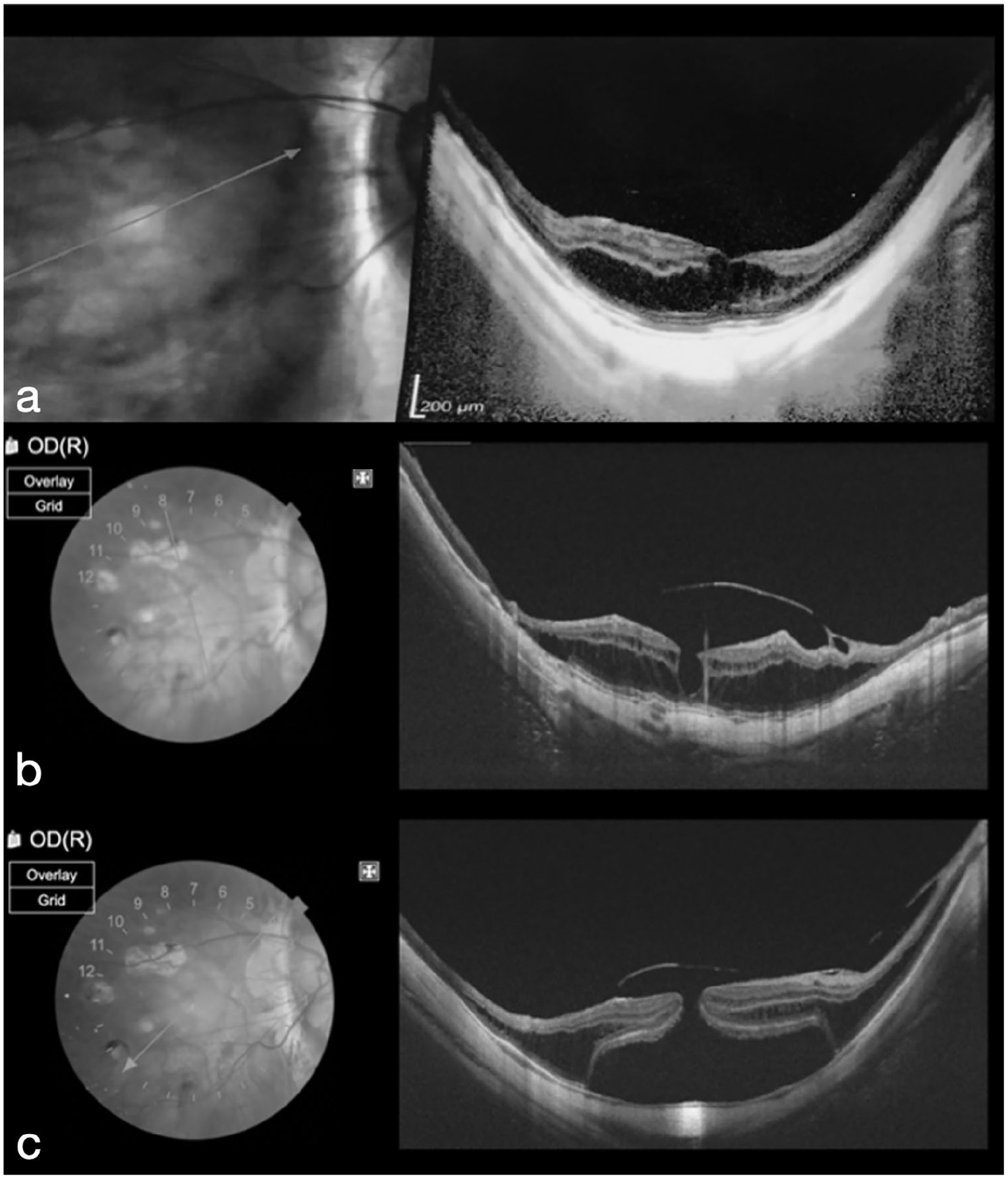
Natural evolution of MTM with prevalent forces perpendicular to the retina in a female patient. (a) OCT taken at the age of 43 on 5 February 2011, showing MTM in the form of inner–outer schisis and normal fovea (Stage MSS 1a). BCVA was 0.8 decimal. (b) The OCT taken at the age of 43, on 11 September 2011 shows a worsening of MTM in the form of inner–outer schisis and normal fovea (Stage MSS 1a). BCVA was 0.8 decimal. (c) OCT taken at the age of 44, on 1 August 2012, showing MTM in the form of predominantly outer schisis and normal fovea (stage MSS 2a). BCVA was 0.7 decimal. (d) OCT taken at the age of 47, showing MTM in the form of predominantly outer schisis (stage MSS 2a). BCVA was 0.7 decimal. (e) OCT taken at the age of 50, showing further worsening of MTM in the form of predominantly outer schisis (stage MSS 2a). The inner component of the schisis is less apparent. The schisis is visible only in the area where the concavity of the sclera is more evident and pronounced. BCVA was 0.7 decimal. (f) OCT taken at the age of 51, showing MTM in the form of schisis detachment with normal fovea (stage MSS 3a). BCVA was 0.2 decimal.
Natural evolution of MTM with prevalent tangential forces in a female. (a) OCT taken at the age of 43, showing MTM in the form of inner outer schisis and inner lamellar macular hole with epiretinal abnormalities (Stage MSS 1b+). BCVA was 0.7 decimal. (b) OCT taken at the age of 53, showing MTM in the form of inner outer schisis and full thickness macular hole with epiretinal abnormalities (Stage MSS 1c+). BCVA was 0.1 decimal.
One case (Figure 7), initially in stage 3, spontaneously improved to stage 1 after vitreous detachment. The same eye, 2 years after the spontaneous resolution progressed to stage 3 and then stage 4 in the absence of evident vitreous traction.
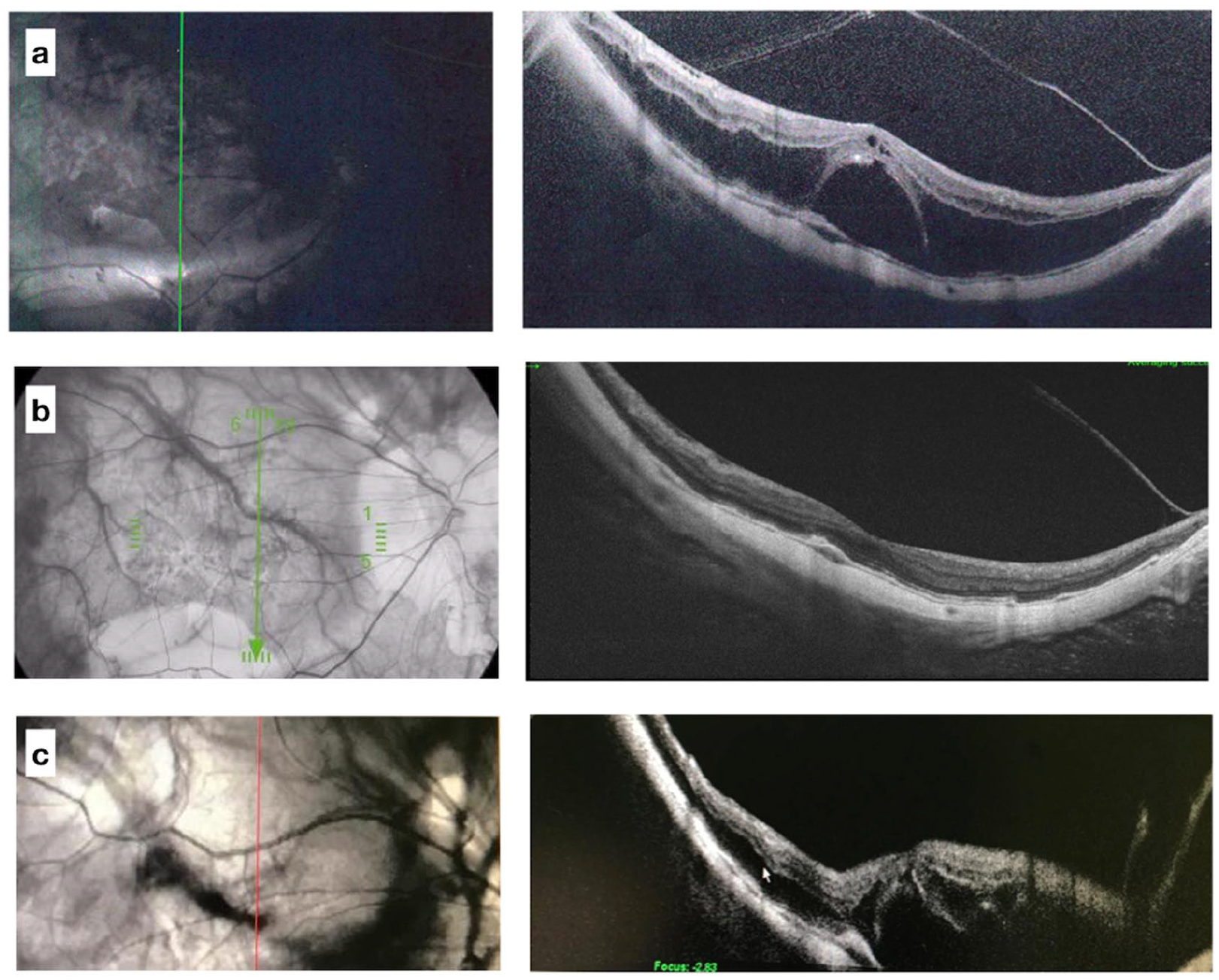
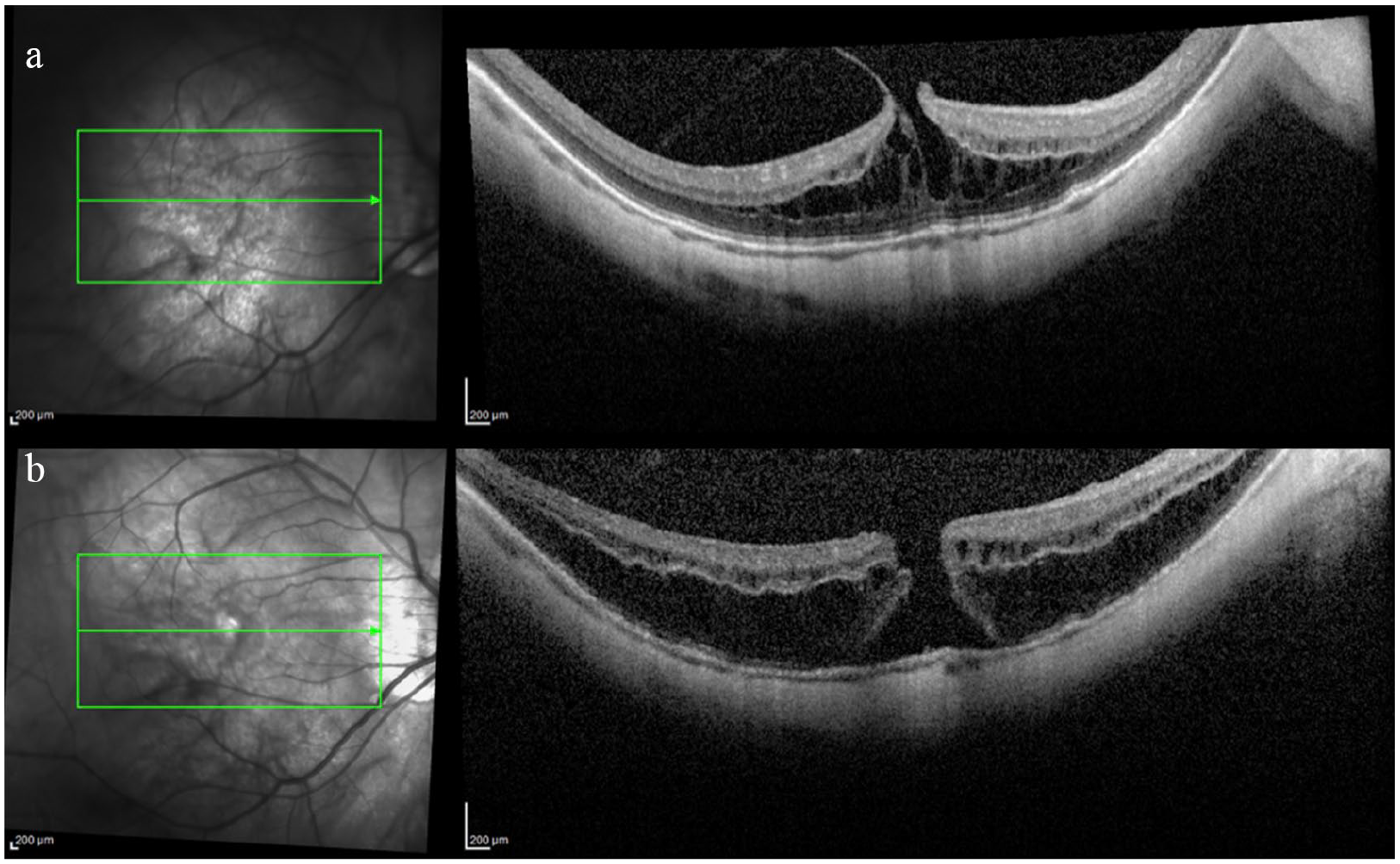
Eye affected by MTM in a female, showing temporary spontaneous resolution. (a) OCT taken at the age of 42, showing MTM in the form of schisis detachment with normal fovea (stage MSS 3a). The vitreous is visible and detached from the macula completely. BCVA was 0.2 decimal. (b) OCT taken 4 months later, showing a spontaneous regression and improvement in vision. The detached vitreous cortex is visible. BCVA was 0.6. (c) OCT taken 4 years later, showing evolution to stage MSS 3a. The eye progressed to stage 4a in 3 months.
The mean time to evolve from pattern 1 to 2 was 40 months, from pattern 2 to 3 was 12 months, from pattern 3 to 4 was 3 months.
We analyzed how BCVA changed with the evolution of the disease. We calculated the BCVA changes as the difference between BCVA at one visit and BCVA at baseline.
The graph in Figure 8 represents the correlation between BCVA changes and the elapsed time from baseline. A negative correlation was present between these two quantitative variables (p = 0.47), meaning that a longer elapsed time led to a worsening of BCVA.
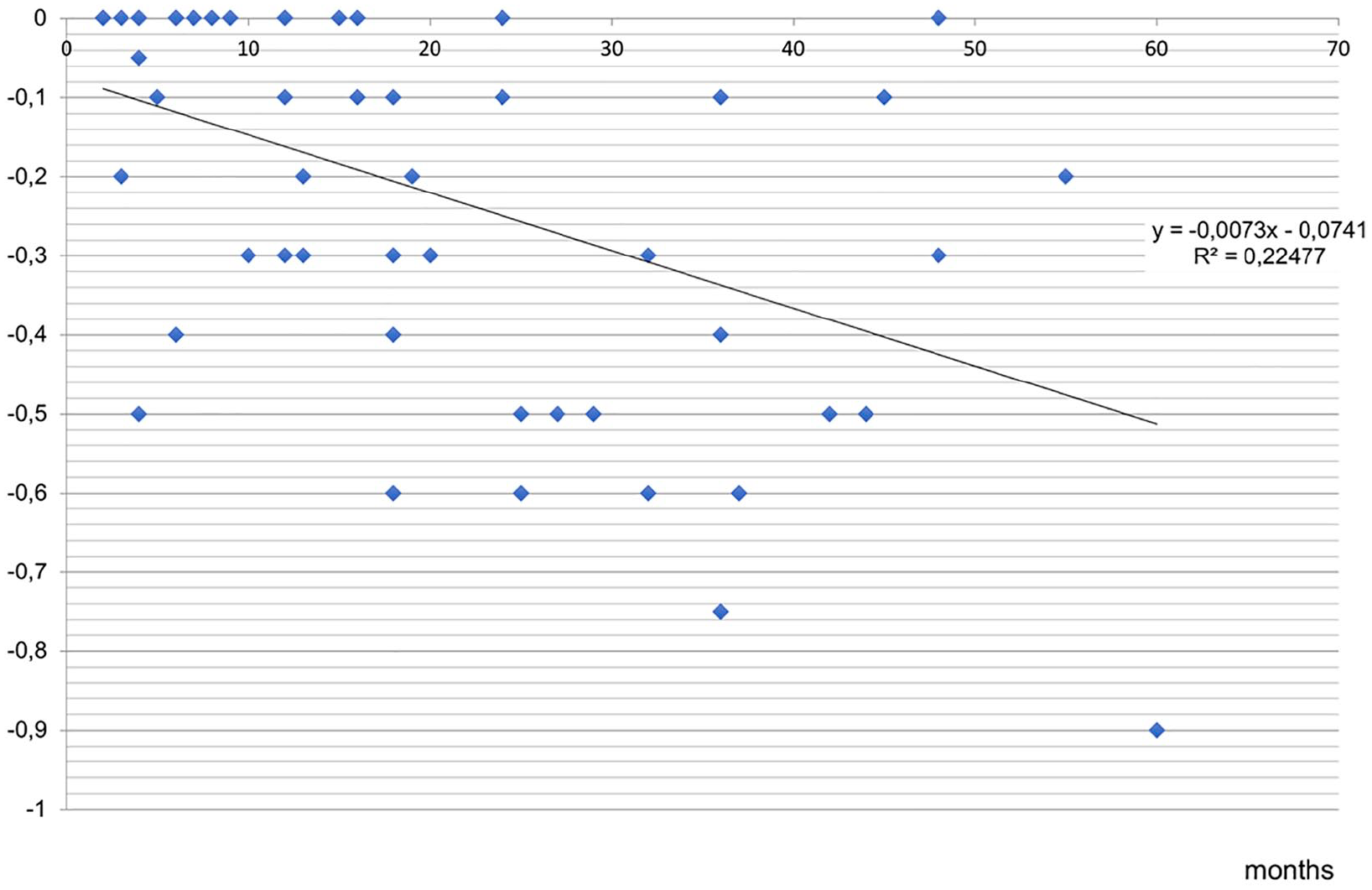
The graph represents the correlation between BCVA changes and the elapsed time from baseline. A negative correlation was present between these two quantitative variables (Regression index p = 0.47).
A new staging system
In light of the results of phase 1 and phase 2, we propose to define the changes in the retinal and foveal patterns, not just as different types of MTM, but as different stages of one evolving disease. We called the new classification “Myopic Traction Maculopathy Staging System,” shorten in the acronyms MSS.
The MSS Table is represented in Figure 9 and shows four stages (1–4) to describe the retinal patterns and three stages (a–c) to describe the foveal patterns.
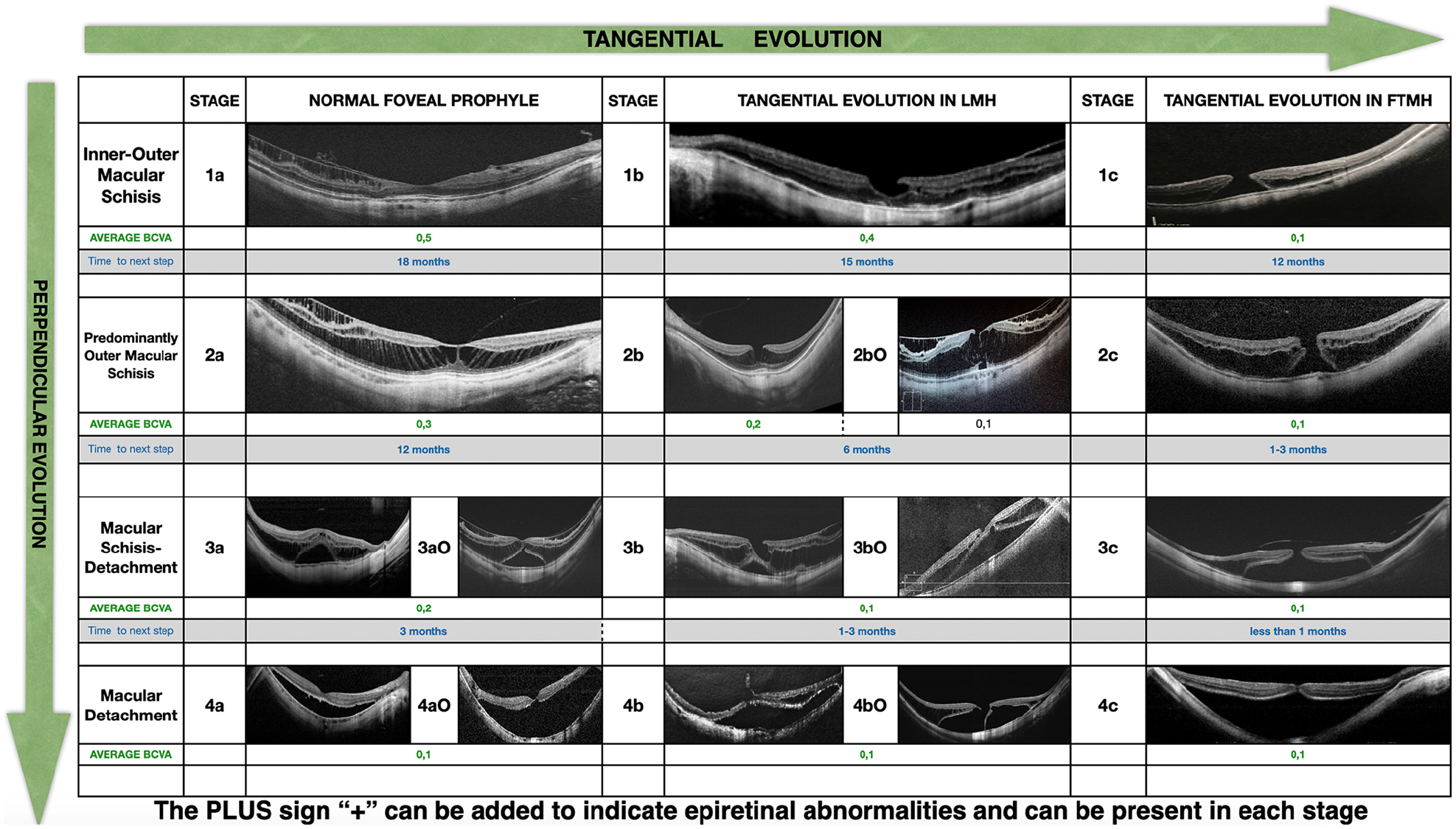
The MTM staging system (MSS) Table. The four rows represent the evolution perpendicular to the retina from inner/outer schisis (stage 1) to predominantly outer schisis (stage 2) to schisis-detachment (stage 3) to complete MD (stage 4). The three columns represent the evolution tangential to the retina and the fovea from normal fovea (stage a) to inner lamellar macular hole (stage b) to full-thickness macular hole (stage c). The outer lamellar macular hole is marked as O and might occur in stage 2, 3, and 4. The presence of epiretinal abnormalities is marked as +, read as “plus” and might occur in every stage.
The retina stages are reported in the four rows of the MSS Table, along the vertical axis, to emphasize the evolution in the layers perpendicular to the retinal plane. The foveal changes are reported in the three columns of the table, along the horizontal axis in order to emphasize the evolution in the layers tangential to the retinal plane. The presence of an O-LMH is reported with “O”, while the presence of epiretinal abnormalities is reported with “+”, read as “plus”.
Stage 1a indicates the presence of inner or inner–outer maculoschisis and the absence of splitting in the fovea.
Stage 1b indicates the presence of inner or inner–outer maculoschisis and the presence of an I-LMH in the fovea.
Stage 1c indicates the presence of inner or inner–outer maculoschisis and the presence of a FTMH.
Stage 2a indicates the presence of predominantly outer maculoschisis and the absence of splitting in the fovea. It might be associated with an O-LMH
Stage 2b indicates the presence of predominantly outer maculoschisis presence of an I-LMH in the fovea. It might be associated with an O-LMH
Stage 2c indicates the presence of predominantly outer maculoschisis and the presence of a FTMH. It might be associated with an O-LMH
Stage 3a indicates the presence of an association of maculoschisis and retinal detachment and the absence of splitting in the fovea. It might be associated with an O-LMH
Stage 3b indicates the presence of an association of maculoschisis and retinal detachment and the presence of an I-LMH in the fovea. It might be associated with an O-LMH
Stage 3c indicates the presence of an association of maculoschisis and retinal detachment and the presence of a FTMH. It might be associated with an O-LMH
Stage 4a indicates the presence of a retinal detachment and absence of splitting in the fovea. It might be associated with an O-LMH
Stage 4b indicates the presence of a retinal detachment and the presence of an I-LMH splitting the fovea. It might be associated with an O-LMH
Stage 4c indicates the presence of a retinal detachment and the presence of a FTMH. It might be associated with an O-LMH.
Considering six ophthalmologists classified the cases, there was an interobserver agreement of 92% and an intraobserver agreement of 98%.
Discussion
This retrospective study allowed us to evaluate a large number of images, from patients affected by MM, visited in 12 years. Although most of the patients had received the first OCT at the time of initial symptoms, by observing the evolution of the contralateral and often asymptomatic eye, and by asking the patients to provide the previous OCT exams available, we could collect a series of OCT scans able to reconstruct a natural history up to 12 years, that is, from the very initial stages of the disease or from a stage with no manifest disease.
Early stages of MTM seem to involve mostly the inner retina. This could be confirmed by the fact that patients in stages 1 and 2 were significantly younger than patients in stages 3 and 4, and by the changes of the OCT scans of the same eyes, showing the evolution from inner schisis to outer schisis or from inner–outer schisis to MD. As expected, BCVA in stage 1 was significantly higher than BCVA in stages 3 and 4. However, we could not document the initial pattern in the inner retina for every case. Some eyes showed first a schisis into the outer retina or simultaneously in the inner and outer retina. That is the main reason why we selected to regroup Stage 1 cases of inner schisis and inner–outer schisis. Some eyes might show an inner schisis in some OCT scan and inner–outer schisis in other scans of the same exam. Only a long-term prospective study on highly myopic eyes without MTM could determine which eyes might develop the initial schisis in the inner or in the outer layers and if this difference has some implications. The vast majority of our cases with a long follow up showed an evolution from schisis in the inner layers toward a schisis into the outer layers and toward a foveal detachment.
The repeatability in the evolution scheme observed in our group of patients, and the correlation between patterns of MTM, age, and BCVA may confirm that MTM is represented in stages, more than in types.
We suggest that MTM is a continuous spectrum of manifestations that evolve following two different possible pathways, depending on the tractional forces involved.
The retina is a multi-layered multicellular structure that is held together, as a unique tissue, by centripetal forces, mainly exerted by the Muller cells, the external, and internal limiting membranes.
In MM, the progressive deformation (elongation but also enlargement) of the sclera induces an increasing stretching of the choroid–RPE–retina complex in two directions: perpendicular and\or tangential to the retina.
The vitreous, as well as the sclera, can generate both tangential and perpendicular centrifugal forces, but with different directions: the vitreous toward the anterior segment of the eye or tangential to the fovea at the vitreoretinal interface, and the sclera toward the lateral and posterior orbit.
There are centrifugal forces that tend to modify the shape and the location of the retina from the natural one, and that counteract the unique centripetal intraretinal force. The combination of forces leads to the different clinical pictures of MTM. We might define these forces as MTM-inducing forces.
Figure 10 describes the interaction of all the different MTM-inducing forces exerted on the retina.
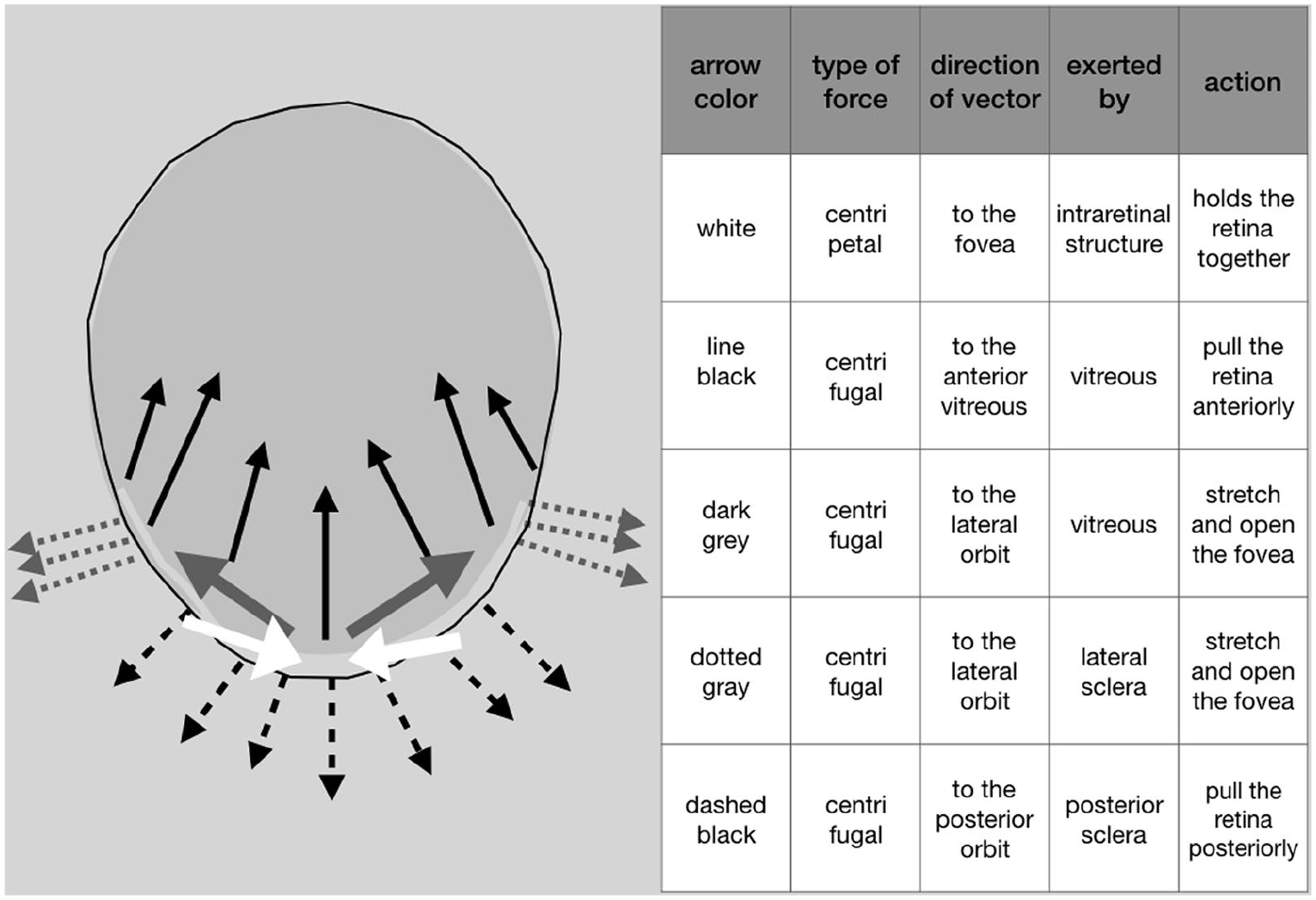
Schematic representation of the different forces exerted on the retina in an eye with pathologic myopia. One centripetal force (white) maintains the shape of the retina and the fovea. Different centrifugal forces tend to detach or stretch the retina and the fovea. Black arrow: centrifugal perpendicular force directed to the anterior segment of the eye. Dark grey arrow: centrifugal tangential force, directed to the lateral wall of the eye and lateral orbit. Dotted grey: centrifugal tangential force, directed to the lateral wall of the eye and lateral orbit. Dashed black: centrifugal perpendicular force, directed to the posterior orbit.
When the prevalent centrifugal MTM-inducing forces are perpendicular to the retina (Figure 5), stage 1 progresses and involves the outer layers becoming stage 2, then 3, then 4. While the outer component further progresses to MD, the inner component of schisis is progressively relieved, because the intraretinal force becomes prevalent when the retina detaches from the RPE. In fact, in stage 4, the inner schisis is no longer visible.
When the prevalent centrifugal forces are tangential to the retina (Figure 6), the eye will develop an I-LMH and eventually a FTMH on a flat retina. We observed different shapes and sizes of I-LMH and hypothesized that this could be due to the fact that the delamination of the foveal layers can be asymmetric in the different macular quadrants. We also observed different depth of the I-LMH that we explained with the predominance of the perpendicular or tangential vector of traction. However, measurements of width and depths of the I-LMH were not evaluated in this study.
The observation that a myopic lamellar macular hole evolves into a FTMH was already made.12,13
When the centrifugal perpendicular forces are combined with centrifugal tangential forces, a MD, with either a lamellar (Figure 2) or a full-thickness macular hole, will appear. We hypothesize that it is the combination of forces that lead to the disruption and splitting of the ellipsoid zone band, generating an O-LMH.
The O-LMH predominantly appears in stage 3, in subgroups a, b, and also c. In fact, even in the presence of FTMH (stage 3c), it is still possible to recognize a band of the outer contour of the hole without the ellipsoid zone. In stage 4, the occurrence of O-LMH was less visible. We explain this observation with partial relief of traction inside the retina when and where the retina is detached from the RPE. We could not make any correlation between the size of the O-LMH and the risk of developing a FTMH. This could be the subject of a future study. The observation that the O-LMH was a sign of progression from schisis to detachment with FTMH has been already made. 10
Epiretinal abnormalities may be associated with every stage and contribute to the disease progression. They were less common in stage 4. In fact, we found only two cases over 31 in stage 4 showing epiretinal abnormalities and they were in stage 4b. It is possible that when the macula is completely detached, the epiretinal abnormalities are less visible on OCT because there is less evident traction on the inner surface after detachment.
Looking at the MSS Table (Figure 9), each stage might show three different possible evolutions: horizontal (to the right), vertical (down), or oblique (down-right) based on the main vector of the centrifugal forces that act singularly or in combination.
A previous study by Shimada et al., 5 on a series of 207 eyes with MTM followed for 2 years, has shown that MTM is a slowly progressive disease. In 2 years, only 11.6% of eyes showed signs of progression and 3.9% showed spontaneous improvement. No cases of detachment were present in the series, but only schisis. The authors found that the chance of progression was significantly higher in eyes with more severe schisis involving the whole macular area.
Spontaneous improvement of MTM has been explained as induced by the spontaneous release of vitreous adhesion or disruption of the ILM.5,14 Other authors described spontaneous improvement also in presence of posterior vitreous detachment and in vitrectomized eyes. 15 We acknowledge the possibility of spontaneous improvement and resolution of the traction. In the MSS staging system, which is dynamic by nature, a stage could switch backwards from bottom to top and (theoretically) from right to left.
In phase 2 of our study, we did not observe a rate of spontaneous resolution as high as published by Shimada. 5 This was probably due to the fact that we were observing a group of patients mainly, although not only, coming to the clinic for symptomatic MTM. It is true that we asked to retrieve the previous OCT, performed in the same eye and in the contralateral eye to study the type of progression in a pre-symptomatic phase. Nevertheless, the selection of our group is mainly symptomatic MTM. However, the purpose of our study was not to study epidemiologically the natural course of the disease but more to describe the evolution of the disease which leads to threatening complications.
We are also convinced that 2 years is not a sufficient span of time to judge the course of this slowly progressive disease. As shown in Figure 5, the disease can remain in the same stage with similar visual function for more than 2 years and then rapidly worsen. It can be speculated that a spontaneous improvement could be just temporary since MM is a degenerative and progressive disease. In fact, we have observed one case (Figure 7), in stage 3, spontaneously improving to stage 1, after vitreous detachment. The same eye, 2 years after the spontaneous resolution, started to progress to stage 3 and then 4 in the absence of evident vitreous traction. We interpreted the case with the progression of the centrifugal perpendicular force exerted by the sclera on the retina, directed toward the orbit, continuously present even after partial relief of the traction induced by the vitreous.
The forces exerted by the vitreous and by the sclera might act independently from each other. Also the vitreous can pull the retina in absence of scleral deformation (as it happens in vitreomacular traction syndromes, even in non-myopic eyes), the sclera can act in absence of the vitreous, in vitrectomized eyes, or in eyes that already showed a spontaneous vitreous detachment, by exerting a centrifugal perpendicular force and a pulling effect in contrast with the rigidity of the retina.
The MSS Table correlates the anatomical with the functional progression of the disease. In fact, BCVA in stages 3 and 4 is significantly lower than BCVA in stages 1 and 2. Furthermore, there is a correlation between time from baseline and a decrease in BCVA.
We have found a statistically significant difference in the mean age of the patients in different stages, being the earlier stages observable in younger patients. The mean age of patients in stage b and c was higher than stage a. However, we hypothesize that age is not the main significant factor to be correlated with evolution. In fact, we observed that stages 3 and 4 could be present even in patients younger than 50 years of age. We could not collect in detail the age at which myopia started to manifest for each patient. It is possible that, if high myopia starts to manifest in infancy, a patient could manifest a stage 3 or 4 even in young adult age. In other words, the MTM stage does not depend only on the age of the patient, but also on the age of onset and duration of the disease.
We could not collect the data on axial length for every eye and at each timing. However, we found no direct correlation between the MTM stage and axial length. We speculate that it is not the axial length that influences the stage of MTM, but the shape of the scleral wall, which could be reconstructed only in 3D and the relationship with the vitreoretinal adhesion and all the consequent tractions.
We can also speculate that the elongation perpendicular to the retina has more space to expand than the elongation tangential to the retina, due to the conformation of the orbit. Therefore, it might take less time to evolve from stage 1 to 4, than to stage a to c with a stretching of the fovea.
A staphyloma was not visible in 14% of the eyes, mainly in eyes with retina patterns 1 and 2. We hypothesize that the eyes with axial myopia and without a posterior staphyloma might have prevalent tangential traction on the retina and therefore more prone to induce changes in the fovea, leading to I-LMH and FTMH.
In 86% of the eyes, there was an association with one type of staphyloma. The staphyloma type 4, which is the nasal staphyloma was not evaluated in this series since we were analyzing only tractional changes into the posterior pole. More than one-third (36%) of the eyes were associated with staphyloma type 1 which is the wide macular staphyloma, the large ectasia involving the macula and the optic nerve. The staphyloma type 2 was the most represented (37% of eyes). Type 2 is known as the narrow macular staphyloma, with the scleral ectasia involving only in the area within the arcades. Interestingly the retina pattern more represented in eyes with staphyloma type 2 were pattern 3 and 4. This observation supports the idea that the retinal changes are induced by the prevalent forces which are perpendicular to the retina, induced by the elongation of the eye and exacerbated by the ectasia at the posterior pole.
Our evaluation of the staphyloma type was done with wide-field color fundus photography, which has a sensitivity and specificity of 85%. 16 We do not know whether an evaluation performed with 3D MRI might lead to slightly different results. The distribution of staphyloma types in our series was in accordance with other published papers.11,16
We studied the progression time from one stage of MTM to another. We observed that the mean time to progress from stage 1 to 2 is the slowest and infers that a patient with stage 1 MTM could be advised to receive a follow-up visit in 2 years. However, since we cannot know for how long the patient has remained in the same stage when we check at baseline, we advise to schedule the first follow-up at 12 months. The progression time from stage 2 to 3 has an average of 1 year. Differently, the time to progress from stage 3 to stage 4 was significantly shorter. Hence indication for surgery should be considered for stage 3 (especially 3b) and 4, in order to preserve and improve vision.
Although spontaneous resolution might occur, the risk to progress from stage 3 to 4a, 4b, or 4c is high and justifies intervention. The risk is higher in the presence of an O-LMH, as stated also by Shimada. 10
More data are needed to clearly identify the timing between stage a to stage b to stage c. However, the change of foveal pattern from a to b takes longer than 1 year. Certainly, a refinement on the mean time of stage change could be improved in the future with the collection of more data. BCVA in stages b and c is lower than stages a and should be considered an indication to surgery.
The correlation between the elapsed time from baseline and BCVA shows that the anatomical progression of MTM is directly proportional to the functional loss. Although BCVA is stable and can be high in stages 1a and 2a, the higher the stage, the lower the BCVA. This is one of the most relevant aspects of our new staging system. Based on MSS, physicians could be able to improve the timing of the intervention, choosing the appropriate follow-up time and the time of intervention. Our final suggestion is to consider surgery based on the actual level of BCVA, in stages 1b, 1c, 2b, 2c, 3a, 3b, 3c, and 4a, 4b, 4c.
In conclusion, we propose a new comprehensive and practical OCT-based staging system of MTM, that could help ophthalmologists to understand the progression of the disease and better manage their patients.
We called the new classification “Myopic Traction Maculopathy Staging System,” shorten in the acronyms MSS, to offer a name easy to remember. MSS was designed to be intuitive and easily categorized with the OCT. It was also designed to remind in one picture the evolution of the disease both in the retina (perpendicular or anteroposterior traction) in the rows, and in the fovea (tangential traction) in the columns. The addition of the mean time to evolve from one stage to the other was meant to offer information on the prognosis of the eye in each stage and therefore a prelude to the guidelines of management of the patient.
Our study has some limitations. Being a retrospective data collection, we could not control the follow-up to choose the interval time for the check-up of these patients. As well, we were not able to collect the OCT scans with the same OCT instrument. Furthermore, some of the older OCTs are not as high quality as the newer equipment. However, we selected for the study only eyes with a quality sufficient to make a judgment on the type of MTM.
More eyes per each stage of MTM, with more data on axial length, could offer a better understanding and confirmation of our hypotheses as well as knowing the initial time of progression of the refractive error. We advocate also a study to compare the MTM stage with the whole shape of the eye globe observed with 3D MRI and B scan, to correlate the type of evolution in the retina, with the evolution of the scleral deformation.
However, our study helps to clarify the pathogenesis as well as the evolution of MTM. And shows how forces act on the retina and the fovea, setting the foundations of the surgical treatment, which should aim to counteract these forces exerted by vitreous and by the sclera, on the retina and the fovea.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.