
Abstract
Purpose:
To examine the nature and frequency of ocular side effects due to systemic target therapy with BRAF and MEK inhibitors as well as immunotherapy with cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death 1 (PD-1) monoclonal antibodies used in the treatment of cutaneous malignant melanoma (CMM).
Design:
While proven effective in cancer treatment, target therapy and immunotherapy have been associated with ocular side effects likely due to their ability to alter the immune privilege of the eye. We conducted a retrospective chart review of patients undergoing target and immunotherapy for CMM and documented all associated eye findings.
Methods:
We reviewed the records of 34 patients receiving target and immunotherapy for CMM who were examined in the academic ophthalmology clinic between 2012 and 2017.
Results:
Ocular side effects were present in 41.1% of patients in this study with 14.7% presenting with uveitis. Patients undergoing therapy with either vemurafenib only or dabrafenib/trametinib combination therapies comprised 70.5% of the study cohort. Ocular side effects occurred in 45.5% and 46.1% of patients on vemurafenib and dabrafenib/trametinib combination therapy, respectively. About 47.5% of males presented with ocular side effects compared to 30.5% of females. Notably, 13/14 patients with ocular symptoms recovered.
Conclusion:
This study highlights the frequency of ocular side effects in patients treated with target therapy and immunotherapy for CMM and shows that symptom resolution can be effectively achieved with proper ophthalmic care. Further research is required to answer whether cessation of these therapies is mandatory during ophthalmic treatment.
Introduction
The worldwide incidence of melanoma has drastically increased in the past 50 years with over 96,000 new cases diagnosed in the United States in 2019. 1 When treated early, melanoma has a 94% survival rate; however, in cases of metastasis, the 5-year survival rate drops dramatically resulting in the death of 1 in 27 males and 1 in 40 females, respectively. 1 Recently, target therapy and immunotherapy have emerged as efficacious treatment options for patients with advanced melanoma. The molecular mechanisms of these therapies involve alterations in either surface proteins involved in the body’s immune response or proteins involved in cell growth and proliferation pathways. 2 These molecular interactions, however, can result in increased immunological activity in organs such as the eye which normally exhibits immune privilege in order to prevent vision loss due to inflammation.3,4
Immune privilege in the eye is facilitated through a variety of mechanisms including lack of lymphatic drainage, low major histocompatibility complex molecule expression, and increased expression of certain surface molecules. 4 This phenomenon is primarily mediated through direct cell to cell interactions between T cells and pigmented epithelial (PE) cells of the eye. 5 More specifically, interactions between the CD86 surface protein of PE cells and the CTLA-4 surface protein of T cells results in cytotoxic T cell suppression and conversion into T regulatory cells.6,7 Certain therapies for advanced stage melanoma likely disrupt ocular immune privilege and have been associated with ocular side effects such as uveitis, conjunctivitis, and decreased vision. 8 The agents indicated in these adverse reactions include Mitogen-Activating Protein Kinase (MAPK) pathway inhibitors such as BRAF and MEK inhibitors as well as immunotherapies such as CTLA-4 and PD-1 monoclonal antibodies.
BRAF inhibitors
The BRAF oncogene encodes a signaling protein in the RAS/MAPK pathway, which promotes cell growth and proliferation when activated. Interestingly, uveal melanomas lack the more common cutaneous melanoma-associated mutations, such as the BRAF mutation, and are instead characterized by other oncogenic mutations. 9 In patients with BRAF mutations there is a continuous activation of cell proliferation as a result of a constitutively activated MAPK pathway, which can lead to certain solid tumor cancers such as melanoma and colorectal cancer. 10 BRAF inhibitors such as vemurafenib and dabrafenib effectively reduce cell proliferation by interrupting the MAPK signaling pathway; 11 however, interruption of the MAPK signaling pathway has also been associated with ocular side effects. One retrospective analysis including 568 patients with melanoma treated with vemurafenib identified adverse ocular effects in 22% of the study cohort. Uveitis, conjunctivitis, and dry eyes were the most common diagnoses occurring in 23, 16, and 12 patients, respectively. The median diagnosis of uveitis occurred at 117 days after vemurafenib initiation and uveitis was managed in all patients using local therapies while continuing vemurafenib treatment. 12 Another study identified uveitis ranging from mild anterior uveitis to severe explosive panuveitis in a cohort of seven patients. 13 Additional reports of adverse ocular events associated with vemurafenib treatment include macular edema, panuveitis, and retinal detachment.14–16
MEK inhibitors
In addition to the BRAF protein, mitogen-activated protein kinase kinases (MEK1/2) are also MAP kinase pathway proteins that serve as molecular targets for treatment of BRAF-mutated melanoma. Suppression of the MAP kinase pathway in the treatment of melanoma can be effectively accomplished by the use of a BRAF inhibitor in combination with a MEK inhibitor, namely dabrafenib, and trametinib, respectively. 17 Similar to vemurafenib, the use of the dabrafenib and trametinib combination therapy has also been associated with ocular side effects. Cases of uveitis in patients undergoing treatment with dabrafenib and trametinib for melanoma have been previously reported, including multiple cases of severe panuveitis with serous retinal detachments.18–22 Multifocal choroiditis and bilateral choroidal neovascularization has also been associated with treatment of melanoma with dabrafenib and trametinib therapy. 23 Interestingly, the individual use of a MEK inhibitor without the use of a BRAF inhibitor for treatment of different cancer types has resulted in the development of multi-focal serous-like chorioretinopathy and uveitis with serous retinal detachment.24,25 However, there is insufficient evidence at this time to determine the individual role of either dabrafenib or trametinib in the production of ocular side effects.
CTLA-4 and PD-1 monoclonal antibodies
Immunotherapy used in the treatment of melanoma includes modulating immune checkpoints through CTLA-4 monoclonal antibodies, such as ipilimumab, along with PD-1 monoclonal antibodies like nivolumab and pembrolizumab. Neoplastic cells are able to upregulate CTLA-4 receptors on the surface of T cells leading to their destruction.26,27 Ipilimumab blocks CTLA-4 receptor and prevents the signaling of T cell death, whereas nivolumab can upregulate the rates of programmed cell death in tumor cells and dendritic cells, among others. A 2015 study of 945 patients with stage III or IV melanoma found that when ipilimumab and nivolumab are used in combination, treatment response rates were 58% while survival increased by 11.5 months in comparison to only 2.9 months with ipilimumab alone. 28 Despite its positive effect on diminishing tumor burden in patients, CTLA-4 antibodies are associated with certain ocular related adverse events such as peripheral ulcerative keratitis, uveitis, and Vogt–Koyanagi–Harada syndrome, which typically manifests within the first 2 months of therapy initiation. 8 Additionally, ipilimumab has been indicated in certain orbital inflammatory diseases such as thyroid-associated orbitopathy (with associated symptoms of proptosis, conjunctivitis, diplopia, pain with extraocular movement, etc.) and idiopathic orbital inflammation (with associated symptoms of dacryoadenitis, myositis, scleritis, optic neuritis, etc.).29–31 One case of idiopathic orbital inflammation even resulted in Tolosa–Hunt syndrome in a 65-year old male patient. 32 In regards to PD-1 antibodies such as nivolumab, uveitis, and iritis are the two most common adverse events documented in a small population of patients. 33 Overall, combination therapy with CTLA-4 and PD-1 antibodies seem to result in increased survival rates though clinical studies continue to be performed to determine the exact degree of high-grade ocular adverse events that may occur in patients.8,28,34,35
Understanding the relationship between target and immunotherapies and the potential for vision-threatening side effects is important for the management of patients with melanoma. Knowledge of this relationship enables providers to effectively balance continuing cancer treatment while simultaneously managing ocular symptoms with local therapies. Our goal is to raise awareness among clinicians that the development of uveitis and other ocular side effects are more than just rare side effects and patients should be educated about these potential adverse events. In an effort to further develop this understanding, we report a series of cases of ocular side effects in patients receiving target therapy and/or immunotherapy for cutaneous malignant melanoma (CMM) and compare these findings to the current literature.
Methods
Retrospective chart review was conducted from 2012 through 2017 for patients treated with various target and immunotherapies for cutaneous metastatic melanoma who were referred for eye examination to the Eugene and Marilyn Glick Eye Institute, Indiana University School of Medicine, Indianapolis, IN, USA. The retrospective study was approved by the institutional review board (IRB) of Indiana University School of Medicine. Information on patient demographics, therapy type, as well as the dose and frequency of therapy was collected. The effects of ocular symptoms were evaluated by collecting data including the time of presentation, the ocular diagnosis, and visual acuity at presentation. We additionally recorded the type of target therapy or immunotherapy, local treatment of ocular side effects, and overall patient outcome.
Results
A total of 34 patients (21 male, 13 female) treated for CMM with target therapy and/or immunotherapy were referred for an eye examination. The mean age at examination of the entire study group was 51.5 ± 12.7 years. About 13 patients received a single therapy, 12 patients received a combination of therapies, and the additional nine patients were transitioned from one therapy to a different therapy during the treatment process either due to failure of that particular treatment or due to certain clinical trial protocols. More specifically, single therapy with dabrafenib, vemurafenib, or ipilimumab was administered to 1, 11, and 1 patients, respectively. Combinations of dabrafenib/trametinib, and ipilimumab/nivolumab were administered to 11 and 1 patients, respectively.
Of all patients receiving target and/or immunotherapy for CMM in this study, 41.1% presented with ocular side effects (Figure 1). The individual presentation of ocular symptoms in each of these 14 patients is described in Table 1. Out of all male patients in this study, 47.6% presented with ocular symptoms compared to 30.8% of females presenting with ocular symptoms (Figure 2). Of patients presenting with ocular symptoms, five received vemurafenib only, four received dabrafenib/trametinib combination, one received ipilimumab only, two transitioned from dabrafenib/trametinib combination to ipilimumab, one ipilimumab to dabrafenib/trametinib combination, and one transitioned from ipilimumab to pembrolizumab. The corresponding administered dose of each therapy or combination of therapies is also displayed in Table 1. The mean time between initial treatment and presentation of ocular symptoms was 4.6 months. Therapy was suspended in five of these patients in response to uveitis and all five of them experienced resolution of their symptoms with ophthalmic treatment. For other adverse ocular events, therapy was temporarily suspended in two cases. The decision to stop or resume a particular therapy was ultimately decided by the oncologist and not the ophthalmologist. All but one of the patients who experienced non-uveitic ocular side effects had resolution of their ocular symptoms within 2 weeks to 2.5 months.
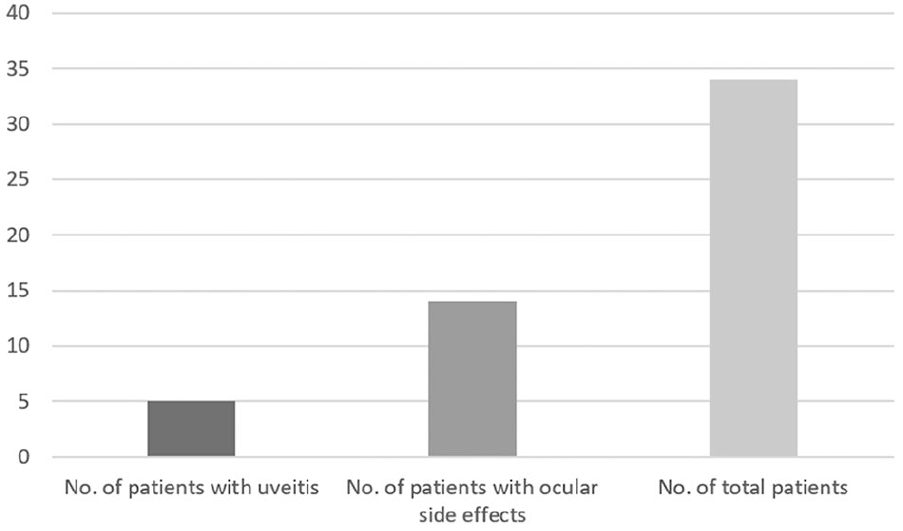
Number of patients with ocular side effects compared to the total number of patients receiving any type of target therapy or immunotherapy.
Individual clinical presentation of patients undergoing target therapy and/or immunotherapy for cutaneous malignant melanoma and presenting with ocular side effects.
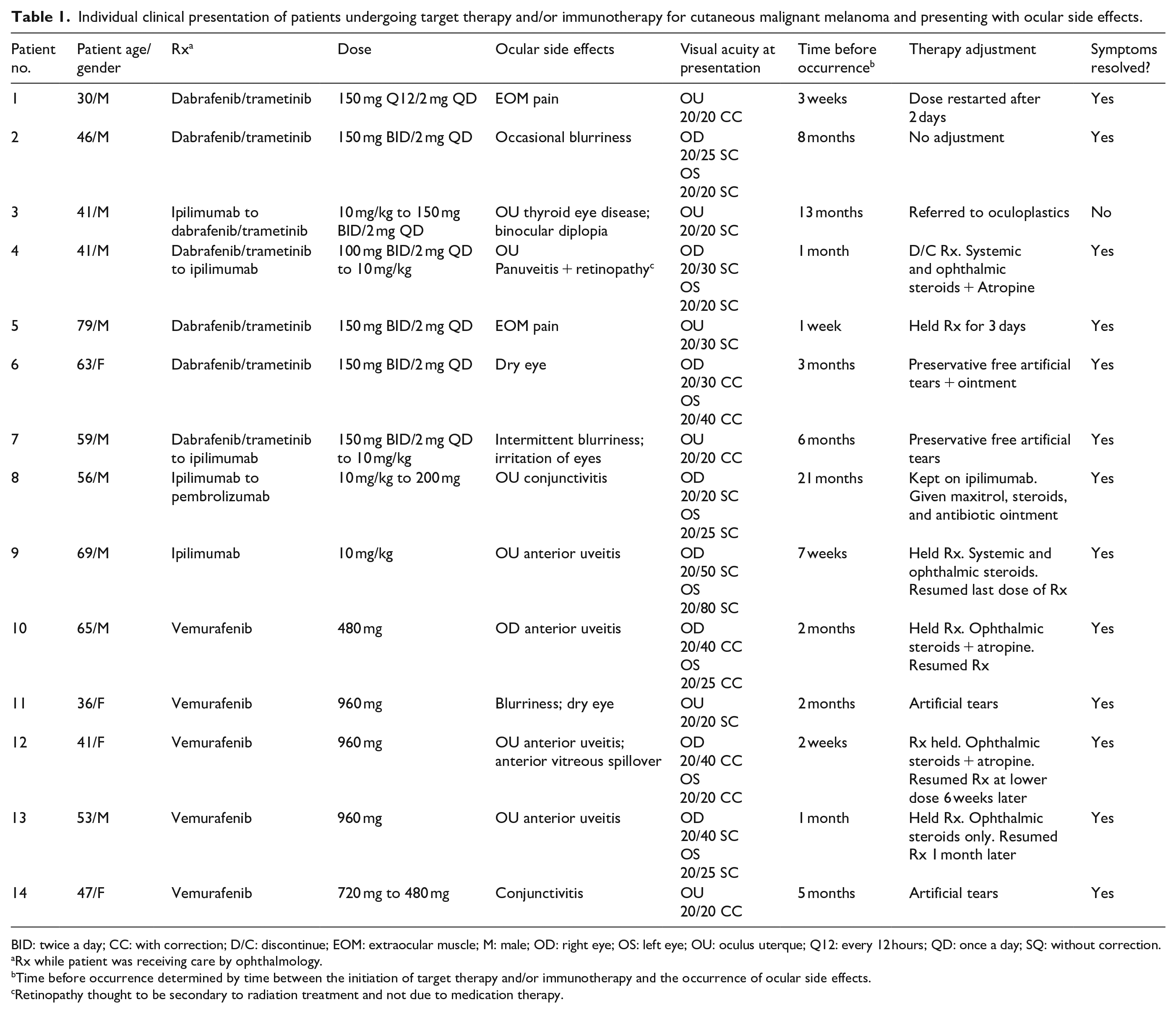
BID: twice a day; CC: with correction; D/C: discontinue; EOM: extraocular muscle; M: male; OD: right eye; OS: left eye; OU: oculus uterque; Q12: every 12 hours; QD: once a day; SQ: without correction.
Rx while patient was receiving care by ophthalmology.
Time before occurrence determined by time between the initiation of target therapy and/or immunotherapy and the occurrence of ocular side effects.
Retinopathy thought to be secondary to radiation treatment and not due to medication therapy.
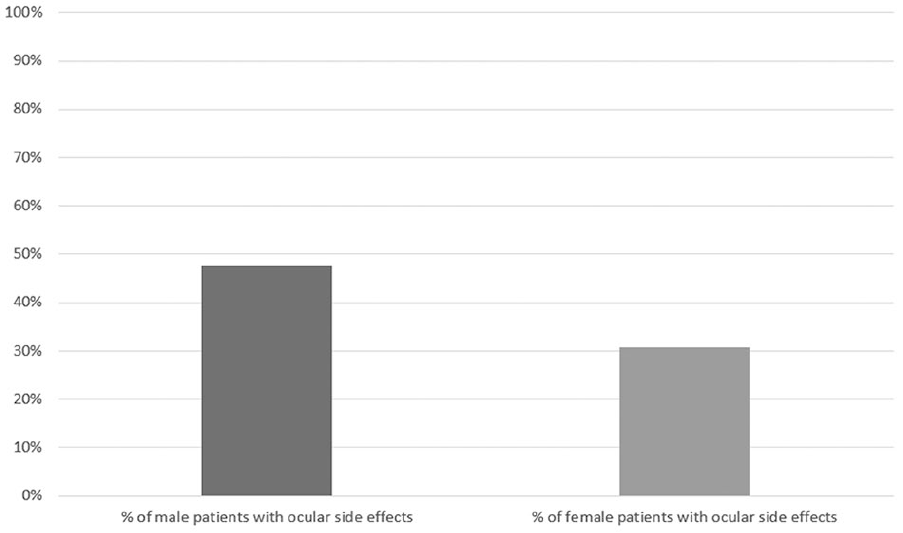
Percentage of male patients with ocular side effects compared to percentage of female patients with ocular side effects.
Among the 34 patients treated with target and/or immunotherapy, 14.7% developed uveitis. Three of the uveitic patients received therapy with vemurafenib only and presented with anterior uveitis. One uveitic patient received ipilimumab only and presented with anterior uveitis, and the remaining patient received the dabrafenib/trametinib combination and presented with panuveitis and retinopathy. Other ocular symptoms experienced by patients in our cohort included conjunctivitis, dry eye, blurry vision, extraocular motility (EOM) pain, and thyroid-like orbitopathy with intermittent binocular diplopia. Patients undergoing therapy with vemurafenib only or dabrafenib/trametinib combination accounted for 9 out of the 14 cases with ocular symptoms (Figure 3). Patients receiving ipilimumab only accounted for one case of ocular symptoms while patients receiving dabrafenib only and ipilimumab/nivolumab combination therapies did not experience ocular symptoms. The remaining four cases of ocular symptoms occurred in patients who underwent a transition of treatment, therefore a single or combination therapy cannot be implicated in these cases.
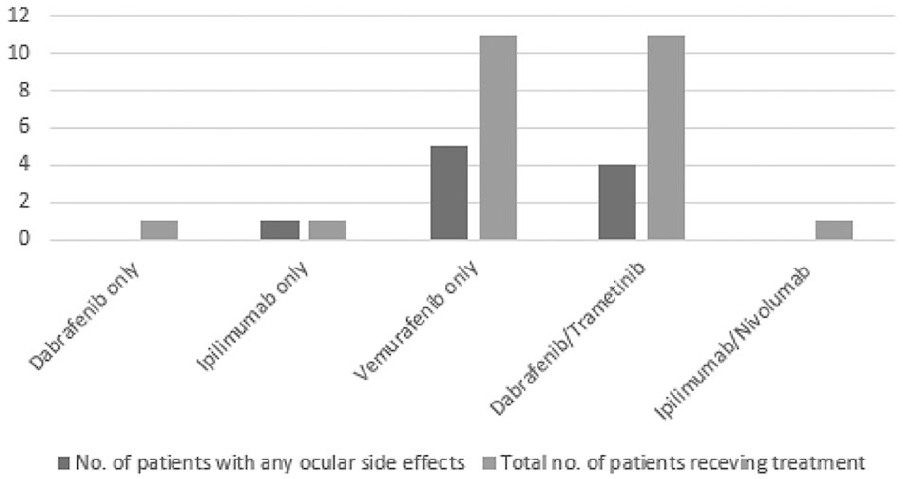
Number of patients presenting with ocular side effects compared to the total number of patients receiving a given therapy. Figure 3 does not consider patients in our cohort who switched to a different therapy during cancer treatment (n = 9).
Age did not play a role in ocular side effects. The mean age of patients presenting with ocular symptoms was 51.7 ± 13.9 years compared to a mean age of 51.3 ± 12.1 years among patients without ocular symptoms.
Discussion
The aim of this study was to showcase the ocular side effects of various target and immunotherapies for patients with CMM. In our study cohort, we found that 41.1% of patients undergoing treatment of CMM with these therapies exhibited a comorbidity of ocular side effects. Uveitis, which can lead to blindness, was found in 14.7% of patients taking these agents and accounted for 35.7% of those with ocular symptoms.
Vemurafenib
Interestingly, vemurafenib was the therapy of choice in three out of five of the patients presenting with uveitis. The association between vemurafenib and ocular side effects has been implicated in the literature with one study estimating adverse ocular events in 22% of patients undergoing treatment with vemurafenib. 12 In our present study, ocular symptoms were present in 5 out of 11 or 45.4% of patients undergoing therapy with vemurafenib. Our findings suggest a higher frequency of ocular side effects in patients undergoing target therapy for treatment of CMM as compared to Choe et al. 12 This difference may be due to differential study definition of ocular side effects as well as the fact that there is no well-established consensus of this frequency in the literature.
Dabrafenib and trametinib
Among patients treated with dabrafenib/trametinib combination therapy, 4 out of 11 or 36.3% of patients experienced ocular symptoms. This compares to 45.4% of patients in the vemurafenib only subgroup and the 41.1% of patients in the overall study cohort with ocular symptoms. It is possible the BRAF/MEK combination therapy might have a better safety profile than single-agent therapy, but more data and further study are needed before drawing a conclusion. As mentioned previously, three of the five patients with uveitis were on vemurafenib only and one was on ipilimumab only. The remaining one patient had been previously treated with vemurafenib with poor tumor control and was later stabilized on a combination of dabrafenib/trametinib. However, it was not until 4 weeks after the patient was transitioned off trametinib (due to decreased ejection fraction) to ipilimumab that uveitis developed. For patients on dabrafenib/trametinib therapy, there was no incidence of uveitis unless the patient was switched onto ipilimumab.
Because most other treatment groups only consisted of a single patient or patients who had undergone a switch in medication, it was not possible to estimate the frequency of ocular symptoms due to ipilimumab only, dabrafenib only, and the ipilimumab/nivolumab combination therapy. Our study did find that serious side effects of uveitis or thyroid-like eye disease only occurred in patients who were on vemurafenib or ipilimumab. Further studies should be conducted to better understand the relationship between these therapies and ocular side effects.
Demographic relationships
When looking at demographic differences within the study cohort, there was no significant difference in mean age between patients presenting with ocular side effects and patients without ocular side effects. Therefore, our study does not indicate age as a risk factor for ocular side effects in patients undergoing target and immunotherapy. Interestingly, the percentage of the entire male cohort experiencing ocular symptoms was 47.6% versus only 30.5% in the female cohort. This might suggest that male patients receiving target and immunotherapy are at an increased risk of ocular side effects compared to their female counterparts; however, more research is necessary to further elucidate this finding. Additionally, our results match current data that indicate a slight predominance of bilateral versus unilateral uveitis.36,37
Clinical implications
Regardless of the associated target therapy or immunotherapy, it is clear that when identified, these ocular side effects can often be resolved with proper ophthalmologic care. This is exemplified by the fact that most patients who experienced ocular side effects achieved full remission of symptoms with no long-term sequelae. Our results are important when considering the risk/benefit profile of these medications. Overall, patients may be able to achieve a significant decrease in tumor burden with the addition of symptomatic treatment for ocular side effects.
It is unclear whether cessation of systemic therapy is mandatory and is an area for further research. In the future, there may also be some benefit to comparing which gene markers for melanoma are more likely to develop inflammatory conditions, such as uveitis, thyroiditis, or even colitis.
Limitations
Herein we reviewed the prevalence of adverse ocular events in patients undergoing target and/or immunotherapy for CMM; however, there are some limitations to acknowledge. First, is the limited number of cases that were available in our time range between 2012 and 2017. There may be an underestimation of true outcomes if patients become lost to follow-up. This study also does not take into account the presence of comorbid systemic or ocular diseases that could potentially lead to greater adverse ocular events during therapy. Cancer severity, a possible confounding variable, was not distinguished in our study between patients experiencing ocular side effects and those that did not. Furthermore, minor ocular side effects experienced by our patients such as blurriness, EOM pain, and dry eye are common symptoms in the normal population and may result from other systemic medications/causes and not necessarily from the melanoma therapy. Thus, we may be overestimating the incidence of minor ocular side effects. Lastly, when considering our patients presenting with uveitis, it is worth noting that only a few patients received a full uveitis workup to rule out other etiologies for their symptoms.
Conclusion
In conclusion, the ocular side effects of target therapy and immunotherapy are clinically relevant. Our results show that 41.1% of our patient cohort presented with ocular side effects including dry eye, eye irritation, pain with eye movement, intermittent blurriness, conjunctivitis, thyroid eye disease with binocular diplopia, retinopathy, or uveitis. No patients experienced documented vein occlusions or visual field changes while on any of these treatments. Uveitis represented 35.7% of patients with ocular effects or 14.7% of overall patients on the target and/or immunotherapy. Among the various agents used to treat CMM, the most common agents leading to uveitis occurred with vemurfenib and ipilimumab. Since no screening protocol is recommended at this time, oncologists and ophthalmologists should be mindful of adverse ocular events when prescribing these therapies for patients. It is unclear whether or not a dose reduction or cessation of therapy is necessary for the treatment of ophthalmic symptoms. It is important to engage patients in discussion to review the risks and benefits of these life-saving therapies. Clinicians should be aware of potential ocular side effects within CMM patients in order to effectively prevent vision loss in this susceptible population.
Footnotes
Disclosure
Dr. Alon Harris would like to disclose that he receives remuneration from AdOM for serving as a consultant and a board member; he serves on the board of Phileas Pharma, and has received reimbursement from Thea for a speaking engagement. Dr. Harris also holds an ownership interest in AdOM, Luseed, Oxymap, and QuLent. The contribution of the author Alice C Verticchio Vercellin was supported by Fondazione Roma and by the Italian Ministry of Health. None of the other authors listed have any financial disclosures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.