
Abstract
Purpose:
To report the characteristics of non-proliferative fellow eyes in patients with unilateral proliferative macular telangiectasia type 2 (MacTel).
Methods:
This was a multicenter, retrospective study and included fellow eyes of eyes with subretinal neovascular membrane (SRNVM). Multimodal imaging including fundus photography, optical coherence tomography (OCT), and OCT angiography (OCTA) was performed. OCT and OCTA measurements included central macular thickness (CMT), subfoveal choroidal thickness (SFCT), foveal avascular zone (FAZ) area and qualitative parameters such as distortion or enlargement of FAZ, increased inter-vascular spacing, dilated, tortuous vessel at margin of FAZ, crowding of vessel, and loss of choriocapillaris (CC).
Results:
Thirteen fellow eyes of 13 patients with mean age of 63.6 ± 12.0 years were included. Fellow eyes had various stages of the diseases – stage 2 (four eyes), 3 (six eyes), and 4 (three eyes). OCTA showed increased intervascular spacing (8; 61.5%), dilated (11; 84.6%), and elongated vessels (8; 61.5%) at the margin of the FAZ, crowding of vessels (6; 46.2%), capillary non-perfusion areas outside the FAZ (4; 30.8%), and areas of CC loss (4; 30.8%). Mean follow-up was 9.1 ± 12.9 months. Out of six eyes with follow-up of ⩾12 months, two developed SRNVM at 18 and 33 months with OCTA showing crowding and entanglement of dilated retinal vessels in deep capillary plexus at baseline which corresponded to the area affected by SRNVM.
Conclusion:
Fellow eyes of proliferative MacTel showed established disease stages on OCTA with progressive capillary crowding and entanglement of vessels likely corresponding to the future site of SRNVM.
Keywords
Introduction
Macular telangiectasia type 2 (MacTel) is a neurodegenerative disorder characterized by changes in the inner and outer retina in the form of ectatic retinal capillaries and right-angle venules and pigment plaques.1–4 Gass and Oyakawa provided the original description of MacTel with further changes subsequent to the availability of newer imaging techniques.2–4
The classification system proposed by Gass and Blodi summarized the disease pathology in five stages. The earliest that is, stage 1 showed late phase diffuse hyperfluorescence in fundus fluorescein angiography (FFA) whereas stage 2 (reduction of parafoveal transparency), stage 3 (dilated right angled venules), stage 4 (pigment plaques), and stage 5 (subretinal neovascular membrane; SRNVM) represented unique clinical findings. 2 Various authors have also described the clinical, angiographic (FFA) and optical coherence tomography (OCT) based changes in eyes with MacTel.1,3,5,6 Recently, OCT angiography (OCTA) has been used to provide details of superficial and deep capillary plexus (SCP/DCP) and other capillary changes in the form of loss of SCP/DCP, thinning of vascular caliber and presence of telangiectasia.7–11 Toto et al. reported a reduction in foveal and parafoveal vessel density in eyes with MacTel compared to normal control eyes and described the superiority of OCTA compared to FFA in diagnosis of SNRVM. 8 OCTA, compared to the previous gold standard FFA, may also prove beneficial in early stages of MacTel. However, the majority of OCTA based studies have been cross-sectional studies without any long term follow-up.7,8,11,12
Although MacTel is commonly a bilateral disease with a prevalence rate of 0.1% in population of age >40 years, it is typically asymmetric in its progression and up to 2% of all MacTel eyes may harbor SRNVM, a vision threatening complication.1,6,13,14 The annual rate of transition from non-proliferative to proliferative (SRNVM) stage is currently not known. It is possible that fellow eyes of SRNVM carry a higher risk of conversion compared to eyes with no SRNVM in fellow eye. OCTA may be used to identify the long term changes in retinal vasculature and possibly predict the development of neovascularization. In the current work, we study this unique subgroup that is, fellow eye of eyes with SRNVM and report the long-term qualitative changes on OCTA, and factors predictive of SRNVM formation in these eyes.
Methods
This multicentric study was a retrospective study and included patients with MacTel and associated SRNVM (either treatment naïve or previously treated) in one eye. The study focused on the clinical and imaging characteristics of the fellow eyes of eyes with proliferative MacTel at baseline and during follow-up. Institutional review board (IRB) approval was obtained and the study was performed in accordance with the tenets of Declaration of Helsinki.
The diagnosis of MacTel was established using comprehensive ophthalmological examination and multimodal imaging. Clinical diagnosis of MacTel was made using signs such as perifoveal graying of retina, right angled venules, pigment clumps, and/ or crystalline deposits as reported earlier. 1 Multimodal imaging included fundus or multicolor photography (Topcon, Tokyo, Japan; Heidelberg Engineering, Heidelberg, Germany), autofluorescence, OCT (Swept source DRI OCT Triton, Topcon, Tokyo, Japan; Spectralis, Heidelberg Engineering, Heidelberg, Germany; Cirrus HD-OCT, Carl Zeiss Meditec, Dublin, CA), and OCTA (Swept source DRI OCT Triton, Topcon, Tokyo, Japan; Spectralis, Heidelberg Engineering, Heidelberg, Germany; Cirrus, AngioPlex OCT angiography, Carl Zeiss Meditec, Dublin, CA; Plex Elite 9000, Carl Zeiss Meditec, Dublin, CA).
OCT analysis included central macular thickness (defined from internal limiting membrane (ILM) to retinal pigment epithelium (RPE), subfoveal choroidal thickness (from outer border of RPE-Bruch’s complex to choroidoscleral interface), and other qualitative parameters such as disruption of inner retinal layers, ellipsoid zone (EZ), external limiting membrane (ELM) integrity within 1000 µm of fovea, presence of ILM drape sign or any cystoid changes. Both 3 × 3 mm and 6 × 6 mm OCTA scans were done in all patients; however, only 6 mm scans were used for quantitative analysis. OCTA images were qualitatively graded for identification of foveal avascular zone (FAZ), distortion or enlargement of FAZ, the area of FAZ, presence or absence of increased inter-vascular spacing, dilated, and/or crowding of vessels, loss of choriocapillaris (CC) and tortuous vessels at margin of FAZ. Two independent observers performed the qualitative analysis of OCT and OCTA scans and any discrepancy was resolved by mutual consensus.
Statistical analysis: Data were tabulated in excel and statistical analysis was performed using Statistical Package for the Social Sciences (SPSS version 23, IBM, USA). Comparison of continuous variables between SRNVM and fellow eyes was done using linear mixed model to accommodate the common intra-individual variables in both eyes. Continuous variables in fellow eyes at baseline and last visit were compared using paired t-test. P values ⩽0.05 were considered statistically significant.
Results
The fellow eyes of 13 patients with bilateral MacTel and unilateral SRNVM were retrospectively analyzed. Mean age of the study cohort was 63.6 ± 12.0 years and included seven males and six females. Two patients had a history of non-insulin dependent diabetes mellitus and other two patients had a history of systemic hypertension.
The baseline comparison of parameters in SRNVM eyes and their respective fellow eyes is presented in Table 1. Briefly, mean BCVA in SRNVM eyes (0.61 ± 0.21 logMAR; Snellen’s equivalent 20/80) was better compared to BCVA in fellow eyes (0.30 ± 0.32 logMAR; 20/40) (p value = 0.01). There was no significant difference in OCT thickness parameters in eyes with SRNVM compared to fellow eyes (CMT, p = 0.22; SFCT, p = 0.40). The area of FAZ in fellow eyes was smaller, but this was not significantly different (p = 0.07). Eyes with SRNVM had received a mean of 3.86 ± 1.57 intravitreal anti vascular endothelial growth factors (VEGF) injections prior to inclusion in the study. In four eyes, SRVNM was still active at the time of inclusion in the study and these eyes continued to receive anti VEGF injections as necessary (mean ± SD: 4.0 ± 2.0). This group showed no significant change in BCVA through last follow-up (p = 0.62). The eyes with non-exudative disease received last injection at least 6 months prior to the inclusion. Only one eye received macular laser.
The baseline comparison of parameters in eyes with subretinal neovascular membrane (SRNVM) and their fellow eye in patients of macular telangiectasia (MacTel) type 2.
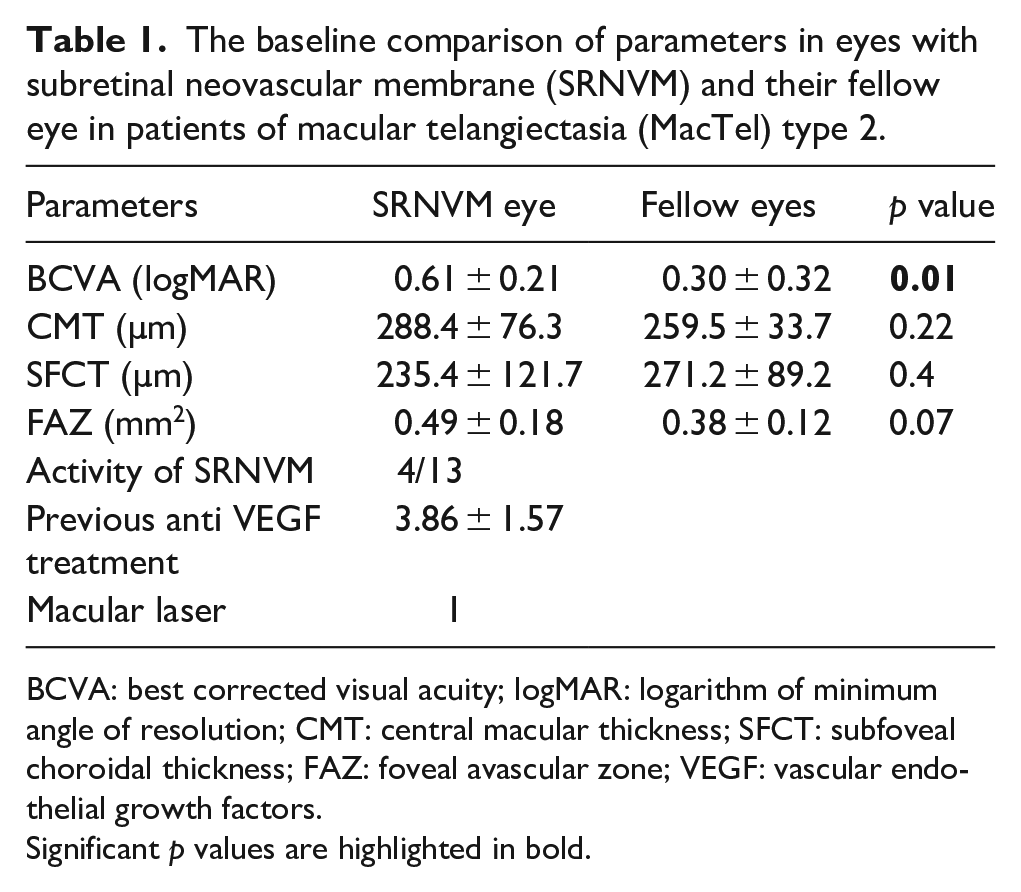
BCVA: best corrected visual acuity; logMAR: logarithm of minimum angle of resolution; CMT: central macular thickness; SFCT: subfoveal choroidal thickness; FAZ: foveal avascular zone; VEGF: vascular endothelial growth factors.
Significant p values are highlighted in bold.
Fellow eyes
Among these 13 fellow eyes, various stages of MacTel were noted including stage 2 (four eyes), 3 (six eyes), and 4 (three eyes). None of the eyes had stage 1 disease at the time of inclusion. Disorganization and dipping of inner retinal layers as graded on OCT imaging were present in more than half the eyes (Table 2) and ILM drape sign was present in 3 (23.1%) of eyes. The integrity of outer retinal layers described in terms of EZ and ELM integrity within 1000 µm of fovea was maintained in 5 (38.5%) and 6 (46.2%) of eyes, respectively.
The baseline OCT and OCT angiography (OCTA) features of the fellow eyes of SRNVM associated with macular telangiectasia (MacTel) type 2.
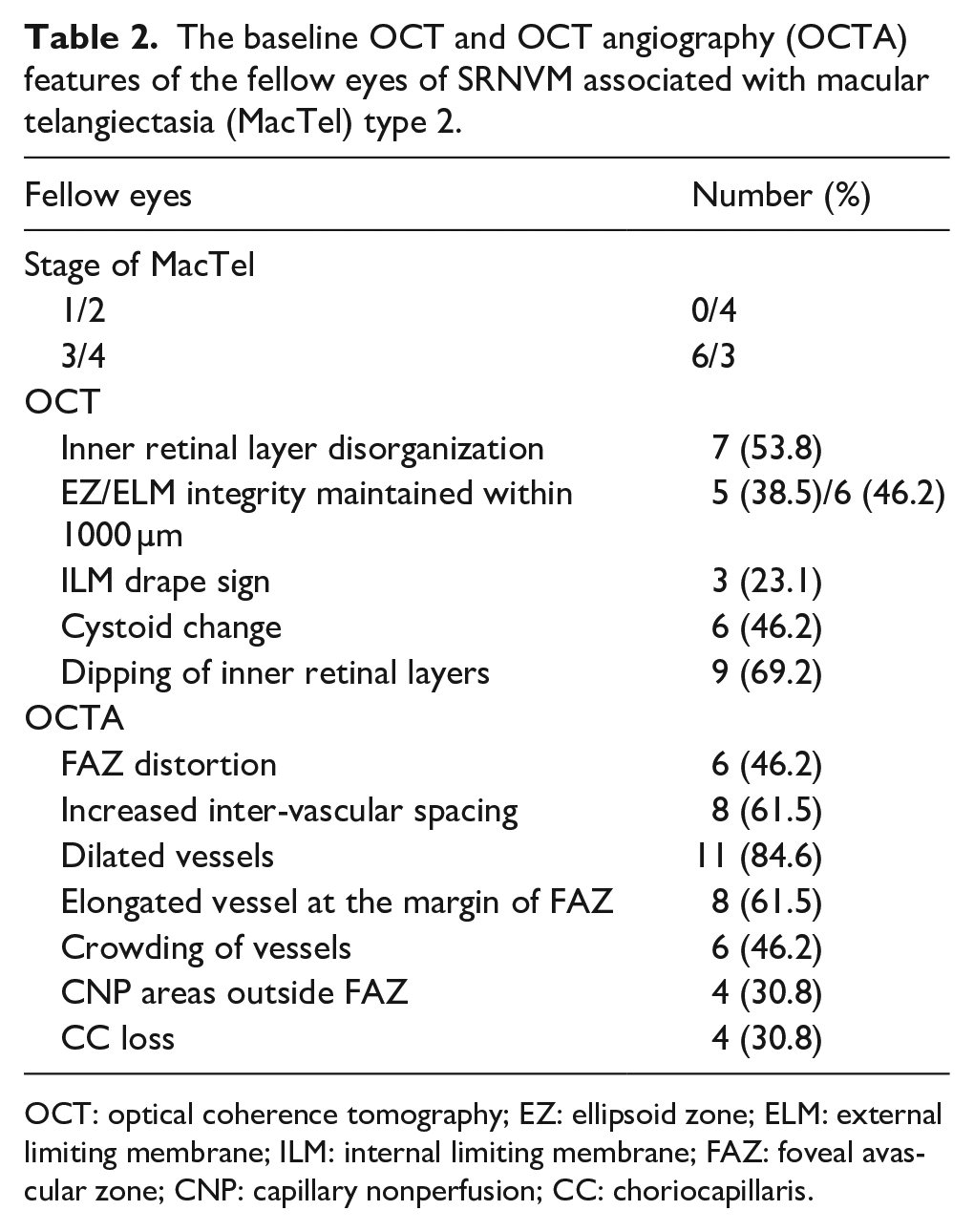
OCT: optical coherence tomography; EZ: ellipsoid zone; ELM: external limiting membrane; ILM: internal limiting membrane; FAZ: foveal avascular zone; CNP: capillary nonperfusion; CC: choriocapillaris.
Multiple qualitative OCTA parameters were analyzed (Table 2). The majority of fellow eyes demonstrated increased intervascular spacing, and dilated, elongated vessels in DCP and SCP especially at the margin of the FAZ. Crowding of vessels and capillary non-perfusion areas outside the FAZ in both superficial and deep capillary plexus were present in 6 (46.2%) and 4 (30.8%) eyes, respectively whereas 4 (30.8%) eyes demonstrated areas of CC loss on OCTA.
Mean follow-up was 9.1 ± 12.9 months. None of the eyes developed SRNVM during the first year. Six eyes had follow-up of ⩾12 months. Two of these eyes developed inner retinal disorganization and cystoid changes on OCT whereas rest of the eyes maintained baseline imaging characteristics. Two eyes developed SRNVM during the follow-up visits. One eye developed SRNVM at 33 months of follow-up which required treatment with intravitreal bevacizumab. Compared to baseline, follow-up OCTA showed crowding and entanglement of dilated retinal vessels which was more pronounced in deep capillary plexus overlying the area of SRNVM (Figures 1 and 2). Eye with SRNVM had received three intravitreal bevacizumab injections in the past with no additional treatment during the follow-up visits.
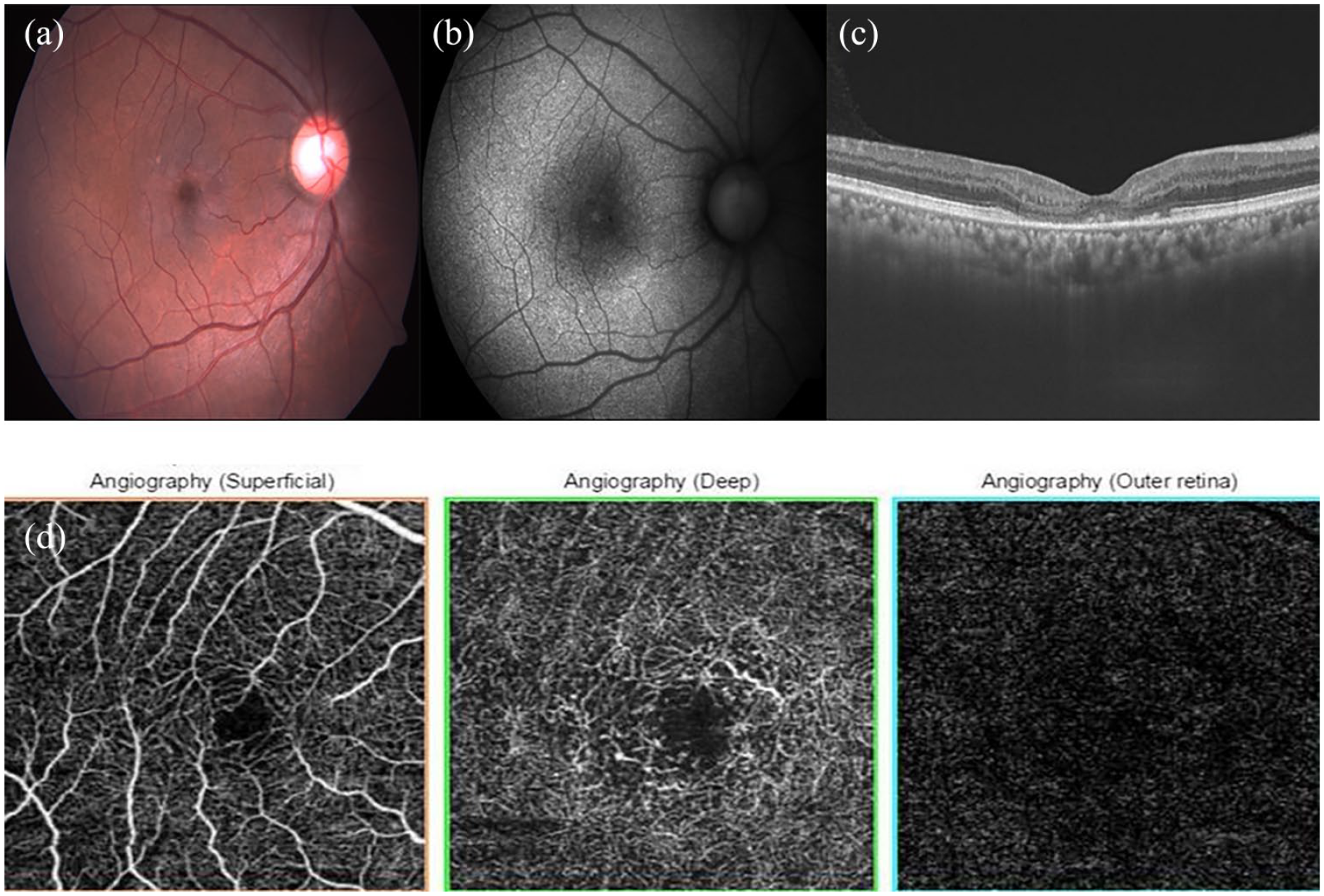
Fundus photograph (a) and autofluorescence (b) of a 62 year old patient shows loss of retinal transparency, parafoveal graying, and right-angled venule. Optical coherence tomography (OCT) showed loss of outer retinal layers with collapse of inner retinal layers (c). OCT angiography revealed distorted foveal avascular zone (FAZ), enlargement of FAZ in deep capillary plexus, with no neovascular network on outer retinal slab (d). This appearance was suggestive of macular telangiectasia (MacTel) type 2 stage 3. Other eye had presence of subretinal neovascular membrane (SRNVM) and had received three intravitreal bevacizumab injections in the past with no additional treatment during 33 months of follow-up.
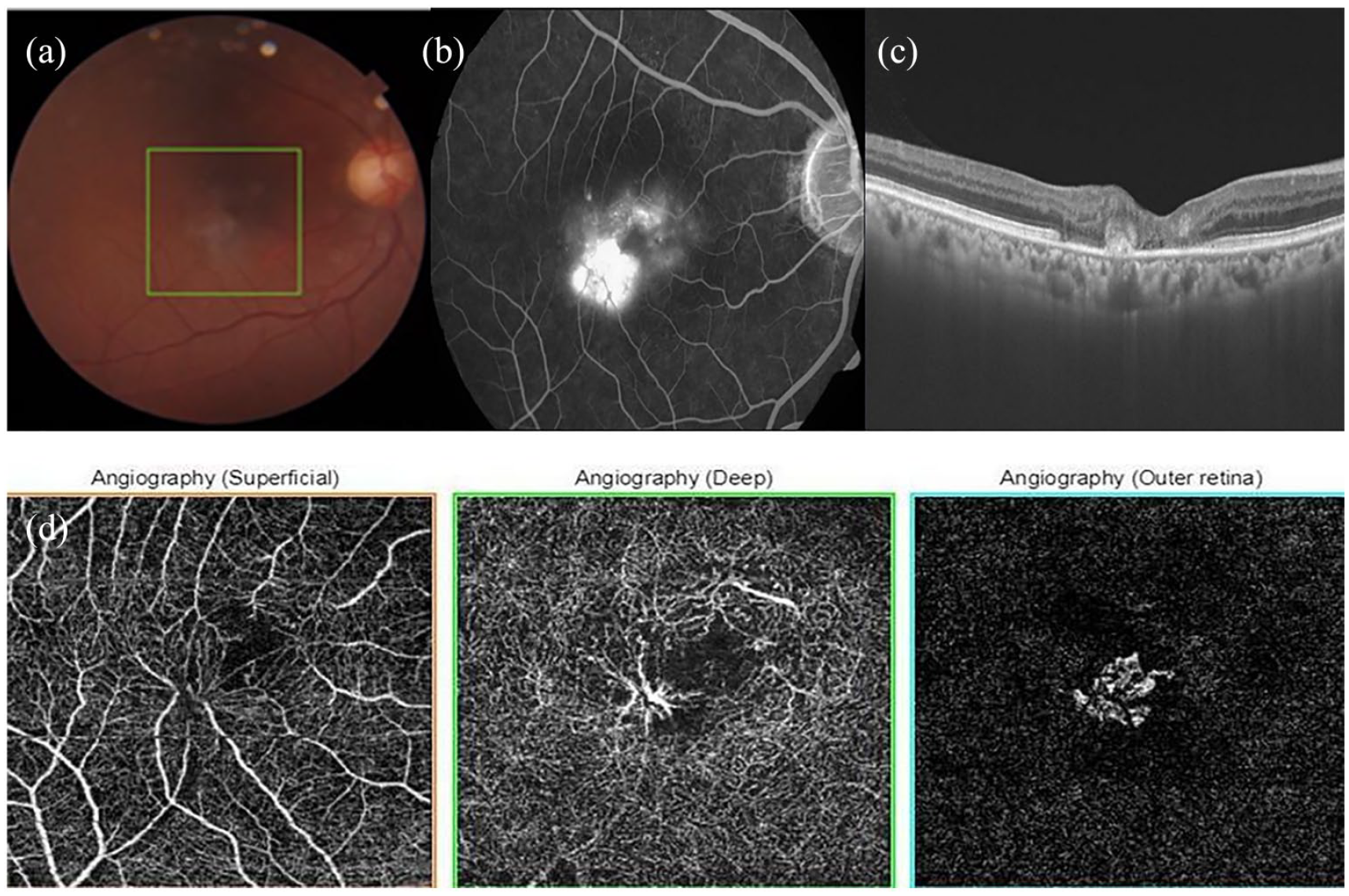
Same patient in Figure 1, at 33 months follow-up, showed small grayish subretinal neovascular membrane temporal to fovea (a). FFA showed minimum perifoveal hyperfluorscence and leakage inferotemporal to fovea (b). OCT revealed subretinal hyper-reflectivity with focal retinal thickening (c). OCTA revealed presence of entangled, dilated, telangiectatic vessel overlying SRNVM in DCP whereas neovascular net was seen in outer retina suggestive of MacTel type 2 stage 5 (d).
Another patient was noted to develop SRNVM at 18 months follow-up at the site of capillary crowding and entanglement as shown in Figures 3 and 4 which was treated with two intravitreal ranibizumab injections and remained inactive till last follow-up at 38 months. Right eye had presence of scarred SRNVM at initial visit with visual acuity of 20/400 and did not receive any treatment during the follow-up visits.
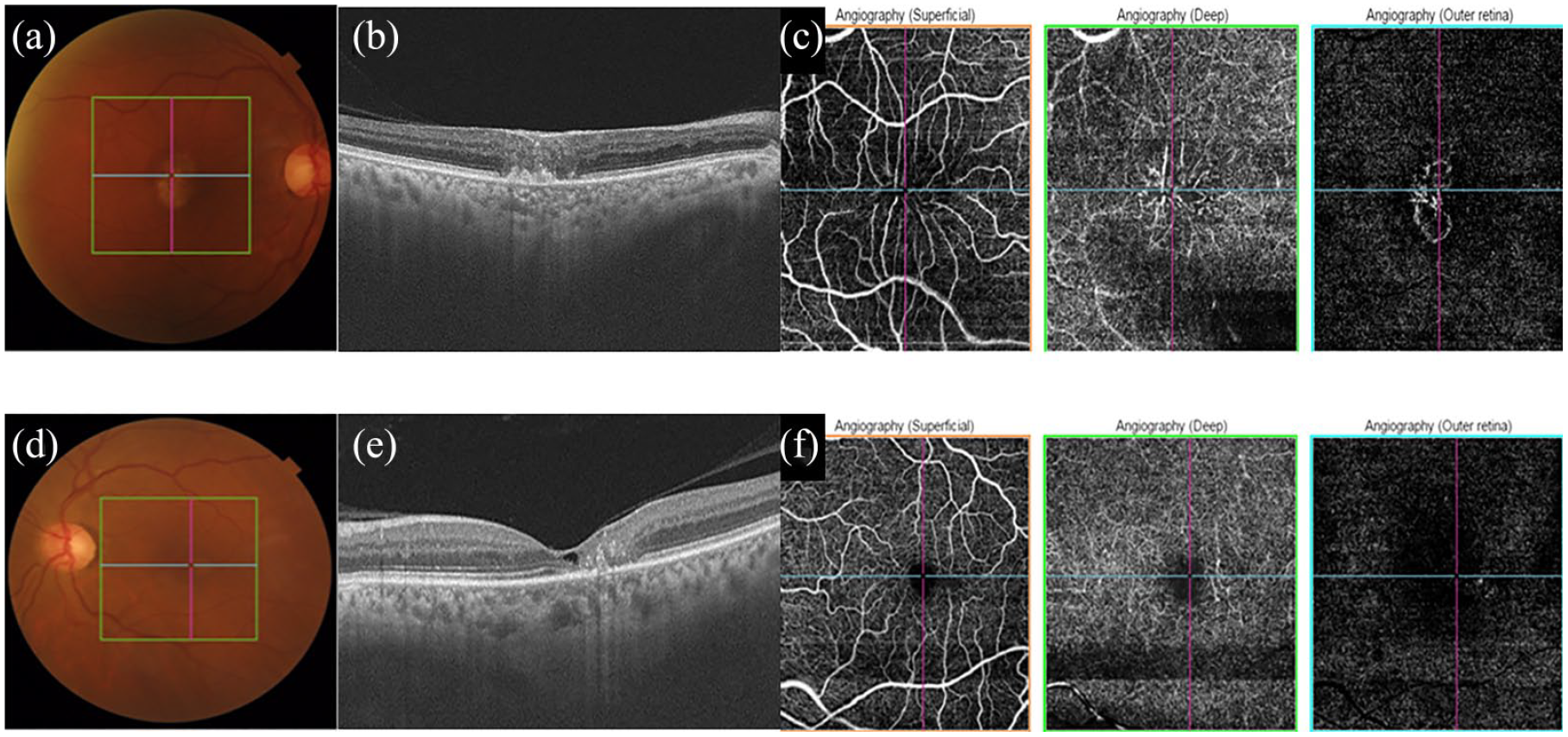
Multimodal imaging of a 65-year patient with diminution of vision in both eyes (right > left). Upper panel (a–c) shows features suggestive of scarred subretinal neovascular membrane (SRNVM) in right eye. OCT showed loss of outer retinal layers and subretinal scarring (b) and OCT angiography revealed loss of foveal avascular zone (FAZ), dilated vessels, perifoveal capillary crowding, and increased intravascular spacing with neovascular complex in outer retinal slab. Lower panel (d–f) shows multimodal imaging of left eye. OCT showed vitreomacular adhesion, inner retinal cystoid degeneration, distorted inner retinal architecture and loss of outer retinal layers (e). OCTA of superficial plexus showed enlarged FAZ temporally with deep plexus showing dilated vessels, temporal capillary crowding, and increased intravascular spacing (f). Diagnosis of scarred SRNVM secondary to proliferative macular telangiectasia (MacTel, type 2 stage 5) in right eye and type 2 stage 3 in left eye was made.
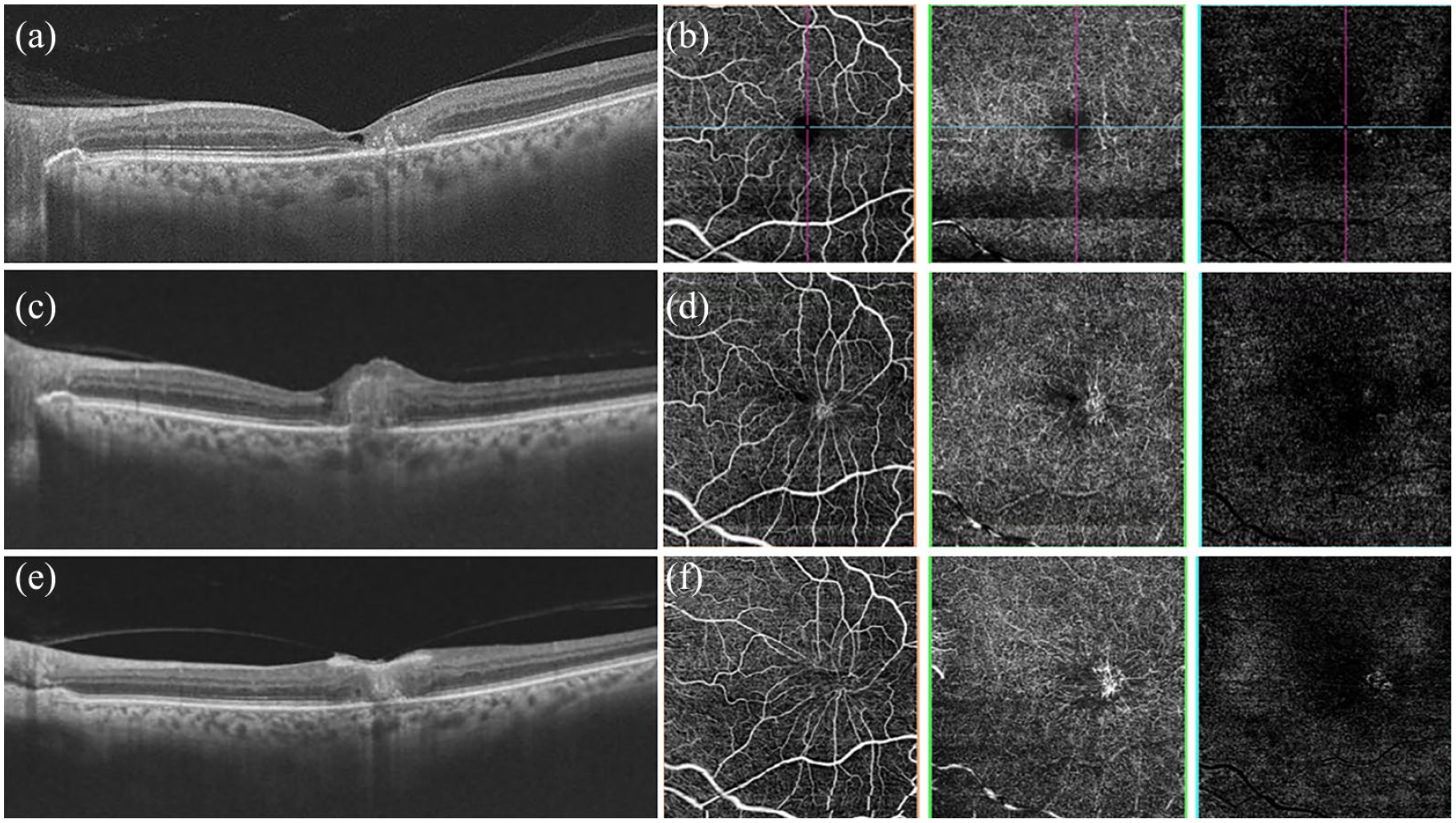
Imaging characteristics of patient in Figure 3 during follow-up visits. Baseline OCT (a) and OCT angiography (b) as described earlier in Figure 3 (d–f). At 18 months, OCT showed presence of intraretinal hyper-reflectivity and retinal thickening (c). OCTA showed increased capillary alterations more prominent temporal to fovea, narrowed FAZ with small, suspicious SRNVM in outer retina underlying the crowded capillaries (d). Subsequently, patient received two intravitreal ranibizumab injections. At 38 months, OCT showed reduced retinal thickness, intraretinal scarring (e) and OCTA reveals increased capillary crowding temporally with an obvious neovascular net (f).
Discussion
The aim of the study was to find the predictive features of SRNVM formation in MacTel eyes on OCTA. We noted capillary crowding and entanglement on OCTA during long term follow-up in eyes which developed SRNVM. These fellow eyes were classified at variable stages of MacTel: stage 2 (four eyes), 3 (six eyes), and 4 (three eyes). None of the eyes was graded as stage 1 disease.
In eyes with MacTel, analysis of OCTA images revealed the earliest location of intraretinal changes in deeper layers of retina and provided detailed information about SCP and DCP not visible on FFA.7,10,11 OCTA features in eyes with MacTel include the presence of telangiectatic vessels, intercapillary widening, FAZ distortion, and loss of deep and superficial retinal vascular capillaries. We found similar OCTA findings in our study. Both eyes which developed SRNVM had crowding of vessel and capillary entanglement overlying the area of SNRVM. This bears similarity to the previous publication with a cross-sectional design wherein the authors reported the location of SRNVM at site of maximum flow abnormalities in deeper retinal layers. 11 Here, we show these progressive OCTA changes over a longitudinal follow-up. On the other hand, out of the remaining four eyes with follow-up of at least 12 months, only one eye showed increase in crowding of vessel during follow-up. The absence of capillaries in the outer retina leads to the presence of low oxygen tension in outer retina and therefore predisposes to the formation of SRNVM. These OCTA changes can be considered the predictive signs leading to SRNVM formation and can be used to assess the risk to fellow eyes.1,3
There was no significant difference in the anatomical OCT and OCTA parameters such as CMT, SFCT, and FAZ area at baseline between SRNVM and their fellow eye. Out of six eyes with ⩾12 months follow-up, two eyes developed SRNVM which was detected at 33 months in one eye coinciding with the site of maximum change in DCP (dilated, crowded telangiectatic capillaries) on OCTA. Similar changes were seen in the other patient who developed SRNVM at 18 months. Remaining eyes failed to show any significant alteration in OCT or OCTA parameters when compared to baseline.
Prevalence of bilateral advanced age related macular degeneration (AMD) either geographic atrophy or choroidal neovascularization can be seen in 20% to 40% which can reach up to 75% over long term.15–17 A higher neovascularization rate has been associated with retinal angiomatous proliferation (RAP; 40%–100%) over 1 to 3 years. 18 Multiple OCT and OCTA based biomarkers can predict the conversion to neovascularization or onset of exudation in AMD.19,20 However, similar predictive models in MacTel to estimate conversion rate to SRNVM or any imaging biomarkers are not available. Moreover, whether the neurodegeneration follows an independent course in each eye leading to SRNVM formation is not elucidated till date.
This study has several strengths and limitations. MacTel is an uncommon retinal pathology and identification of cases with SRNVM in one eye and non-proliferative disease in fellow eye is difficult. Literature search could not reveal any studies which specifically focused on the fellow eyes’ changes using multimodal imaging especially OCTA. Since only two eyes developed SRNVM, we could not identify any discrete pattern predictive of future onset of neovascularization. Mean follow-up duration of 9.1 months was short considering the slowly progressive, long term retinal changes in MacTel; however, the progressive vascular changes on OCTA in these eyes were interesting.
In conclusion, fellow eye of patients with SRNVM does show established MacTel disease. Though most of the fellow eyes showed non-specific vascular changes on OCTA, progressive capillary crowding and entanglement might provide a clue to the probable site of SRNVM during follow-up. Studies with larger sample size of this unique cohort with long term follow-up are warranted to evaluate OCTA based predictive factors for the development of SRNVM.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Querques and Dr Sacconi confirm that they are associate editor and editorial assistant, respectively with this journal and were not involved in the peer review process for this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.