
Abstract
Purpose:
To determine orbital anatomical parameters that affect surgical outcome of deep lateral orbital wall decompression.
Methods:
Twenty orbits of 20 patients with moderate proptosis (maximum 25 mm) due to thyroid eye disease who were stable for at least 6 months were included in this prospective cohort study. Four parameters including lateral orbital wall distance (LOWD), removable surface area (RSA), removable surface length (RSL), and sphenoid door jamb thickness (SDJ) were evaluated by computed tomography (CT) scan prior to surgery in these patients. Deep lateral orbital wall decompression without fat removal was done in all patients. Relationship between all these factors and proptosis reduction, 6 months after surgery was assessed.
Results:
Mean proptosis before decompression surgery (mean ± SD) was 23.22 ± 1.19 mm and reduction in Hertel exophthalmometry (mean ± SD) was −3.27 ± 1.03 mm (p = 0.006). Pearson correlation showed that LOWD, RSL, and SDJ had statistically significant correlation with proptosis reduction (p = 0.017, 0.002, and 0.001, respectively.). Linear multivariate regression analysis showed SDJ as the only independent factor in predicting surgical outcome.
Conclusion:
several orbital anatomical factors have significant role in predicting surgical outcome following deep lateral wall orbital decompression. Among these parameters, SDJ is an independent factor, whereas LOWD and RSL are dependent factors. Preoperative assessment of the bony sphenoid anatomy may be helpful in predicting the amount of potential decompression.
Keywords
Introduction
Thyroid eye disease is an autoimmune disease associated with orbital inflammation, fibrosis, and soft tissue expansion leading to compression of orbital structures and subsequent proptosis.1–6 Orbital decompression surgery is designed to decrease proptosis and congestion by expanding the bony orbital volume or orbital fat is removed to debulk the soft tissue volume.3,7,8 Multiple decompression techniques have been introduced in previous decades including lateral wall removal, 9 transcoronal approach, 4 balanced decompression,10,11 endoscopic medial decompression,12,13 and fat decompression.14,15
First described by Leone et al in 1989, deep lateral orbital wall decompression is a frequently recommended surgical option.16–20 There are evidences that deep lateral orbital wall decompression could result in fewer complications such as chronic sinusitis. However, the risk of cerebrospinal fluid leakage, corneal ulcer, and hollowness in the temporal region is still considerable. 21 In previous studies, it was found that the rate of new onset gaze diplopia after this procedure was as low as 2.6%.22,23 Both medial and lateral decompression can effectively reduce proptosis and congestion.24–27
Few studies have evaluated the predictors of surgical outcome in thyroid eye disease (TED) patients. Individual orbital morphology, size of the globe, globe-orbital volume ratio, and stiffness of orbital tissues were among these studied predictors.28–33 The volume of available sphenoid diploe would logically affect the capacity of deep lateral orbital decompression to reduce proptosis. The aim of this study was to assess the relationship between the orbital anatomical dimensions and the outcomes of deep lateral orbital wall decompression.
Methods
The study protocol was approved by local ethical committee of Farabi eye hospital related to Tehran University of Medical Sciences Clinical Research Ethics Board (ID: IR.TUMS.FARABIH.REC.1397.054) and adhered to the tenets of the Declaration of Helsinki. Eligible patients for the study were provided written informed consent after fulfilling inclusion criteria.
This prospective cohort study was conducted from March 2013 to March 2019 at Farabi eye hospital as a tertiary ophthalmic center in Iran. Patients with confirmed thyroid eye disease who were in euthyroid state proved by laboratory data including serum TSH and Free T4 and Free T3 level and had stable condition for at least 6 months were included in the study. Patients with moderate proptosis (maximum 25 mm) were enrolled in the study. Exclusion criteria for the study was prior maxillofacial surgery, facial trauma, orbital surgery, patients with compressive optic neuropathy or severe sight loss, exposure keratopathy, patients who had severe proptosis or those who required a more aggressive decompression surgery as compared with the simple deep lateral wall removal in order to decrease more than 5 to 6 mm of proptosis. At baseline and every visit during the follow-up period, all patients underwent a complete ophthalmologic examination, including exophthalmometry with the same Hertel exophthalmometer (Oculus, Woodinville, WA, USA). Measurements were done by two observers and mean value was used for analysis. Orbital computed tomography (CT) scan (bone window with 1.5 mm fine cut slices) was done for all of the patients and surgery was planned based on the findings of the CT-scan. All patients underwent deep lateral decompression without fat removal by a single oculoplastic surgeon (M.T.R.). Patients were seen in routine follow-up and data from the sixth month visit were used as post-operative results in this study.
Image analysis
Spiral orbital multi detector CT-scan was performed in order to measure orbital dimensions. CT-scan of the patients were imported and analyzed in the Image J software. Those axial images which optic nerve had the widest diameter (slices 14–16 in CT-scan) were evaluated and the following parameters were calculated (Figure 1):
1- SDJ: sphenoid door jamb thickness (cm)
2- LOWD: lateral orbital wall distance (cm)
3- RSA: removable surface area (cm2)
4- RSL: removable surface length (cm)
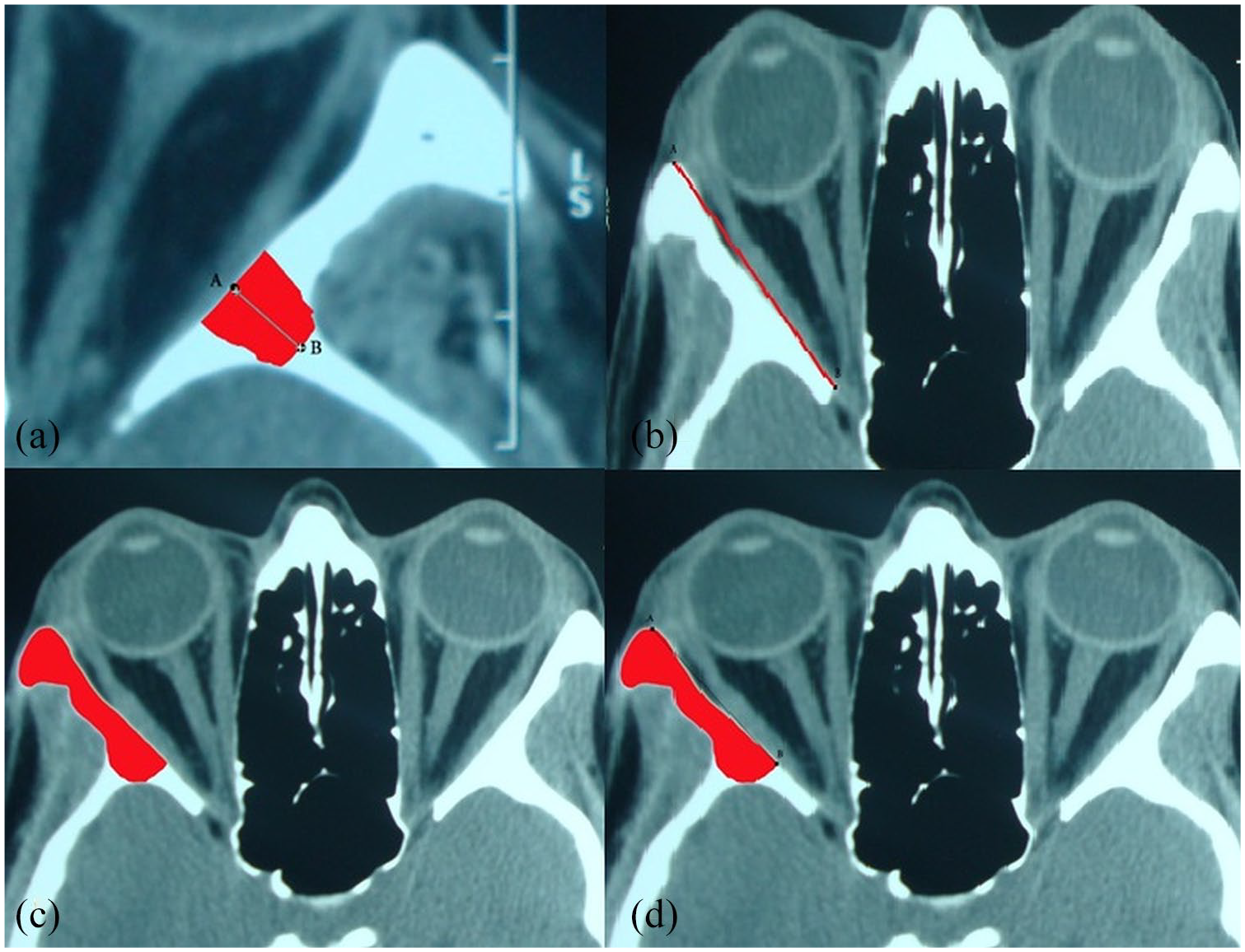
(a) Sphenoid door jamb (SDJ). (b) Lateral orbital wall length (LOWD). (c) Removable surface area (RSA). (d) Removable surface length (RSL).
Anatomical definition
Lateral wall length was defined as the distance between the anterior edge of the lateral orbital rim and the lateral edge of the orbital foramen as seen on a single axial view CT image. Lacrimal keyhole is the wedge-shaped portion of the bone in the superior part of the orbit consisting the frontal bone, the lesser wing of the sphenoid, and a small part of the greater wing which begins from a notch in the superolateral rim and extends into the lacrimal fossa. It is limited laterally by the temporalis muscle, superiorly by the frontal cranial fossa, inferiorly by the posterior thick border of the lesser wing of the sphenoid, and medially till the point which the orbital roof thins as the thin frontal bone. The sphenoid door jamb is a thick trigone of the greater wing of the sphenoid which locates inferior to the lacrimal keyhole. Zygomatic bone and part of the lateral maxilla consists the basin of the inferior orbital fissure 16 (Figure 2).
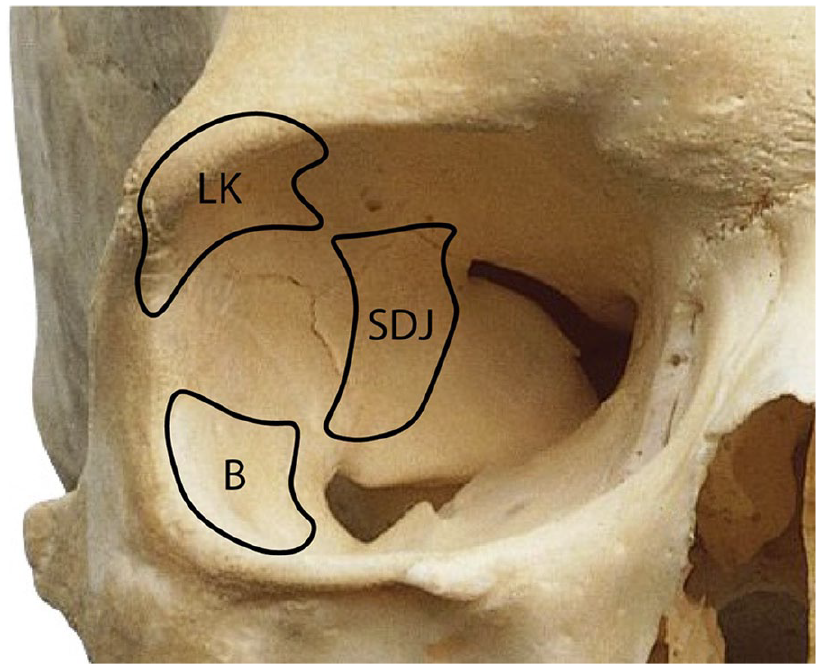
General location of lacrimal keyhole (LK), sphenoid doorjamb (SDJ), and basin (B) bone removed at surgery.
Surgical technique
Lateral orbital wall decompression was performed via an extended skin incision in the lateral third of the upper lid crease under general anesthesia. The superior and lateral aspects of orbital rim were exposed. Periosteum was dissected 2 to 3 mm farther from lateral orbital rim and access to orbital space was provided by elevating intact periorbita. The sphenoid door jamb was drilled following removal of lacrimal keyhole. Finally, the Basin of inferior orbital fissure was removed in similar fashion (Figure 2). Afterwards, the periorbita was opened so that fat and lacrimal gland could occupy the newly created space within the carved bone.6,34 End point of the surgery was maximum drilling until dura was exposed. Following surgery, all patients were given ophthalmic erythromycin ointment and chloramphenicol eye drop.
Statistical analysis
Continuous variables were represented by mean and standard deviation (SD). Change of proptosis was calculated from before to after the surgery. Pearson correlation was used to evaluate the influence of these factors on proptosis change. Then a multiple linear regression was used to assess the independent predictors of proptosis reduction. All analyses were performed in SPSS 25 (IBM, Inc., Chicago, IL).
Results
Twenty orbits of 20 patients (age: 30.3 years (27–35), male/female: 9 (45%)/11(55%)) were enrolled in this study. The severity of thyroid ophthalmopathy was moderate in all patients. Proptosis before and after decompression surgery (mean ± SD) was 23.22 ± 1.19 mm and 19.95 ± 1.51 mm, respectively. Reduction in Hertel exophthalmometry (mean ± SD) was −3.27 ± 1.03 mm (p = 0.006). Table 1 provides summary statistics for preoperative orbital dimensions.
Preoperative orbital dimensions from 20 patients with thyroid eye disease who underwent deep lateral wall decompression.
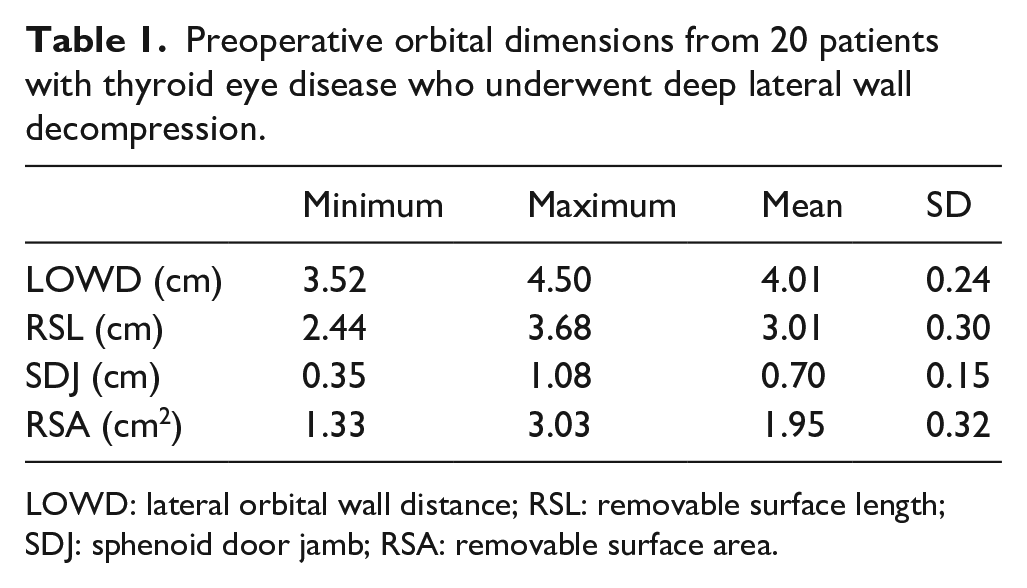
LOWD: lateral orbital wall distance; RSL: removable surface length; SDJ: sphenoid door jamb; RSA: removable surface area.
Correlation between preoperative measure of LOWD, RSL, SDJ, and proptosis reduction were statistically significant (Table 2 and Figure 3).
Correlation of proptosis reduction, LOWD, RSL, SDJ, and RSA.
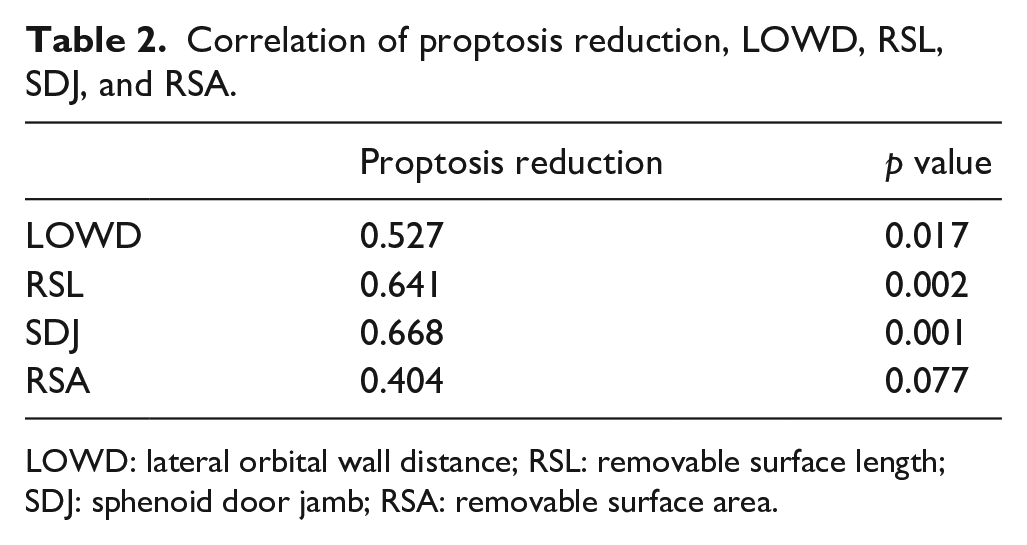
LOWD: lateral orbital wall distance; RSL: removable surface length; SDJ: sphenoid door jamb; RSA: removable surface area.
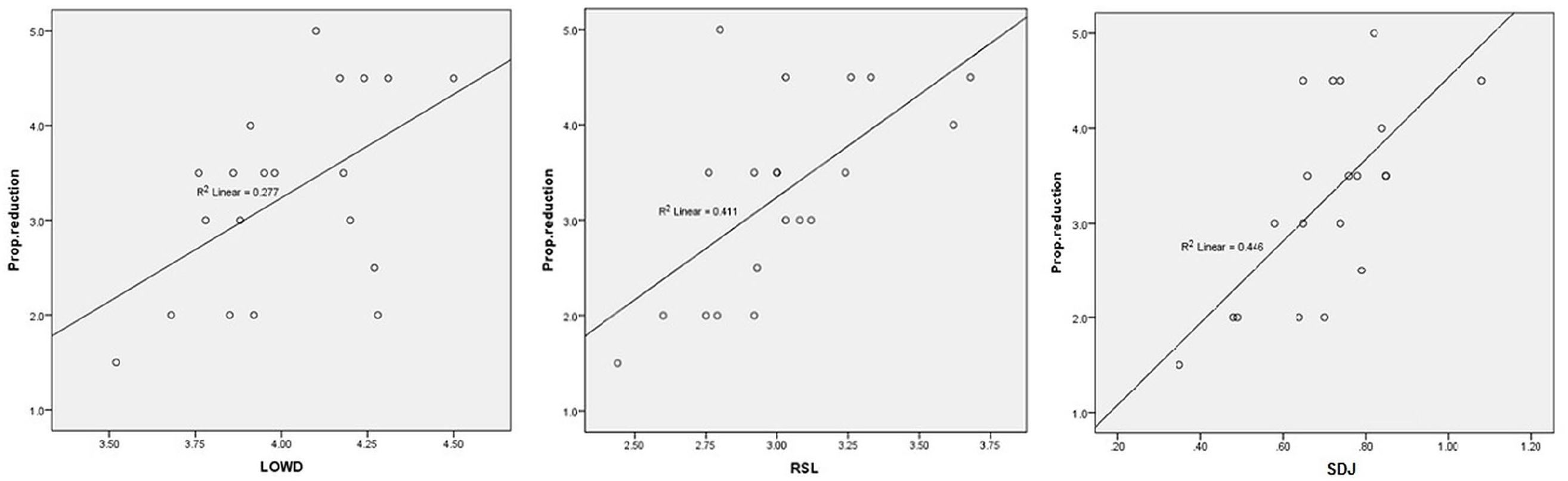
Scatterplot showing LOWD, RSL, and SDJ versus proptosis reduction.
Linear multivariate regression analysis showed that SDJ was the predicting factor in proptosis reduction, whereas the two other factors (RSL and LOWD) remained the dependent factors. The equation for proptosis reduction (mm) was: 2.763 × LOWD − 4.903 (p value =0.045).
Discussion
Orbital decompression expands the orbital volume by partial removal of orbit bones and/or orbital fat in order to decrease the risk of vision loss, reduce proptosis, lid retraction, diplopia, and ocular surface damages. 5
Bony orbital decompression was first introduced by Dollinger in 1911. 35 He managed to decompress orbital contents into the temporalis fossa through lateral orbital wall removal. Naffziger developed a trans-frontal orbital roof decompression technique in order to access to the orbital apex. However, this method did not gain popularity due to its complications and failure in reduction of proptosis. 36 Medial approach was introduced by Sewall in 1936. in this method, orbital content could expand medially into the nose after removal of medial wall via an external ethmoidectomy and could result in reduction of proptosis. 37 Few years later, in 1950, Hirsch introduced a technique for removal of the orbital floor followed by medial wall removal. 38 Transantral Caldwell–Luc decompression of the medial and inferior orbital walls which has benefit of no external incisions was described by Walsh and Ogura in 1957. 39 despite its benefits, postoperative diplopia and infraorbital hypoesthesia caused by this technique, prompted further investigations for finding better approaches. 40 Although several surgical techniques have been introduced, none of them is superior. Therefore, selection of surgical method is individualized to the patient’s condition, expectations, and the surgeon’s experience. 3
Although, three-wall decompression result in higher reduction of proptosis compared to the two-wall procedure, it is associated with more. Therefore, the former is usually reserved for patients with severe preoperative proptosis and conditions such dysthyroid optic neuropathy. 41
Recently, less invasive procedures with higher aesthetic results through insignificant incisions are gaining. As decompression is performed beyond traditional indications such as compressive optic neuropathy, especially for aesthetic reasons, patients expect less postoperative complications. 42 Therefore, removal of the deep lateral wall is becoming the procedure of choice and gaining popularity, either performed alone or in combination with other techniques, as it sufficiently decompresses the orbital content. Although, balancing the removal of medial and lateral orbital walls with sparing the inferior wall, specially the strut, could also result in less diplopia because this procedure produces less inferomedial shifting of the muscle cone, sinusitis is still a concern in this procedure. However, lateral wall decompression surgery alone results in the least postoperative diplopia because bone is mainly removed posterior to the muscle cone.10,43,44 Patient might have decrease sensation of temporal area following lateral orbital wall decompression, because of damages to the zygomaticotemporal and zygomaticofacial nerves, as these nerves pass through the lateral orbital wall and innervate temporal area. This self-limiting condition could happen in 18% to 100% of the patients.17,34 Oscillopsia, resulted by transmission of movements of temporalis muscle onto the orbital contents could be bothersome in some patients. However, it could be minimized by leaving a thin layer of bone on the internal side of temporalis muscle. 45 Temporal hollowness following lateral wall decompression could also happen due to en bloc resection of lateral orbital wall. This complication could worsen over time, because of progressive temporalis muscle and subcutaneous fat atrophy. 46 Cerebrospinal fluid leakage, another important but rare complication of lateral orbital wall decompression, happens due to removal of greater wing of the sphenoid bone and mechanical damage to the dura while drilling. 21 However, by developing piezoelectric drilling method which uses ultrasonic vibrations to reduce the damage to surrounding soft tissues and important structures such as dura, the chance of CSF leak is decreased in comparison to the use of a conventional high-speed drill.47,48
Deep lateral orbital decompression could be done through multiple approaches. Swinging eyelid incision is made of transinferior fornix incision with lateral canthotomy and lysing of the inferior limb of the lateral canthal tendon which could lead to exposure of the lateral orbital wall after elevation of the periorbita. Alternatively, upper eyelid crease incision could lead to wide access to lateral orbital wall, specially its more anterior upper portion, called lacrimal key hole, which is not easily accessible with the former incision. 16
Su choi et al. showed that by using CT-based measurements, volume adjusted correlations between exophthalmos reduction and expanded decompression volume were higher in deep lateral decompression than in medial decompression. The also reported that deep lateral wall decompression has higher surgical predictability than medial wall decompression, as seen with CT analysis. 49 However, using a 3D reconstruction method Alsuhaibani et al. showed that medial orbital wall decompression more highly affects orbital content expansion than does lateral wall decompression. 50
By means of three-dimensional reconstruction of the orbit, Goldberg et al. calculated bony volume of the sphenoid door jamb (SDJ), lacrimal keyhole, and basin of inferior orbital fissure and showed that SDJ occupies the largest volume for bony removal in deep lateral wall decompression. 16 In the current study we showed that SDJ thickness is a predicting factor for proptosis reduction. We classified the patients into three groups as shown in Table 3. Patients with the SDJ thickness of <5 mm had the lowest mean proptosis reduction and there is high correlation between preoperative SDJ thickness and proptosis reduction. Lateral orbital wall distance was another dependent factor in our study that had significant effect on the outcome. Statistical analysis showed that RSL was a dependent factor for surgical outcome whereas RSA had no significant correlation with the outcome. This may stem from the nature of these factors. The more LOWD, the more volume and distance are available to be removed.
Mean of proptosis reduction in three different groups of patients with variable SDJ thickness.
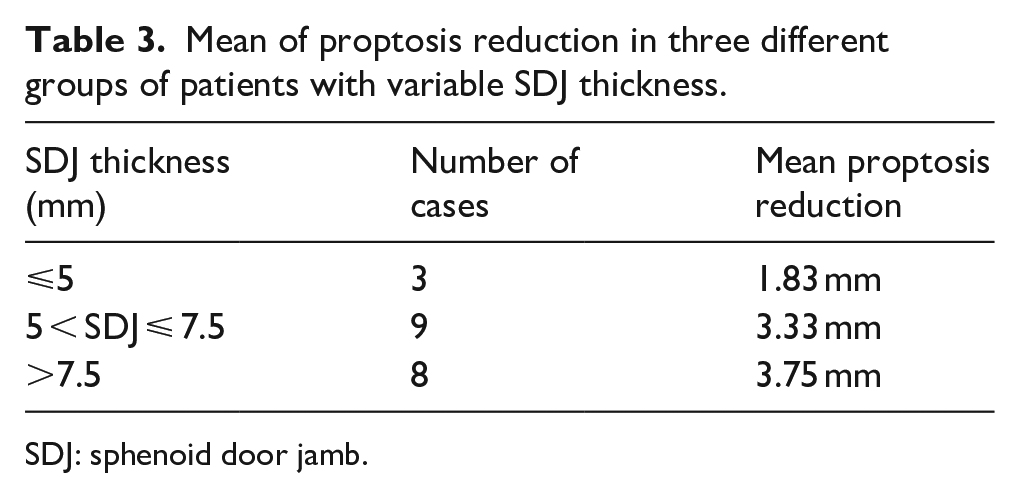
SDJ: sphenoid door jamb.
Nevertheless, we wish to acknowledge the limitations of our study. First of all, two-dimensional reconstruction of orbit may be less accurate data than three-dimensional measurement;8,51 however, three-dimensional analysis is more resource intensive. Hertel exophthalmometry measurements and quantitative CT analysis can introduce intra-observer and interobserver variation; therefore, in order to decrease variations, parameters were measured two times by two different ophthalmologists and mean values were used for analysis. The relatively small size of the study population is another limitation of this investigation. Further studies with larger sample sizes will be needed to confirm our findings.
In this study, we found that sphenoid door jamb width is an independent factor in determining proptosis reduction in deep lateral decompression. Considering the performed quantitative CT analysis, surgical effects of deep lateral orbital wall decompression could be predicted and used by the surgeon for preoperative counseling and surgical decision-making.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
Written informed consent was obtained following complete explanation of the process to the patients.