
Abstract
Purpose:
To evaluate changes in corneal biomechanics after LASIK and F-SMILE.
Setting:
Elite Eye Center, Tanta, Egypt.
Design:
Prospective, randomized, unmasked, interventional comparative case series.
Patients and methods:
A total of 60 eyes were equally divided into two groups; group A: received LASIK and group B: received F-SMILE. Pentacam and CorVis ST parameters were compared before and 6 months after procedures. P ⩽ 0.05 was used for significance of results.
Results:
bIOP decreased by 0.762 ± 1.211 mmHg in group A (p = 0.092), and by 2.52 ± 1.389 mmHg in group B (p < 0.001) and the difference between groups became significant (p = 0.001). A1 increased significantly in group A only (p = 0.036); while A2 decreased insignificantly in both groups. DAR increased significantly in both groups (p < 0.001, p = 0.022), but the difference between groups remained insignificant (p = 0.461). IR increased significantly in group A only (p < 0.001) and the difference between groups became significant (p = 0.026). ARTH decreased in both groups (p = 0.245, p = 0.695) and the difference remained insignificant (p = 0.928). SP-A1 decreased in group A by 8.89 ± 1.38 mmHg/mm (p = 0.637), and by 32.6 ± 4.39 mmHg/mm in group B (p < 0.001) and the postoperative difference between groups was significant (p = 0.013). CBI increased significantly in group A (p < 0.001), but insignificantly in group B (p = 0.098) and postoperative difference between groups was highly significant (p < 0.001). A significant correlation was found between change in CCT and corresponding changes in DAR, IR, and ARTH after surgery in both groups.
Conclusion:
The significant differences between groups postoperatively as regards bIOP (p = 0.001), IR (p = 0.026), SP-A1 (p = 0.013), and CBI (p < 0.001) indicate stiffer corneas after F-SMILE and suggest less influence on corneal biomechanics than LASIK.
Introduction
Recent advances in corneal refractive surgery increased our interest in understanding the biomechanical properties of the cornea. Studying the functional responses of the cornea which exhibits both viscosity and elasticity elements helps us to better understand corneal ectatic conditions such as keratoconus and post-refractive surgery ectasia. Moreover, the results of corneal refractive surgery are affected by the interaction between biological and biomechanical factors and their impact on surrounding ocular tissues.1,2
Although safety and efficiency of corneal laser refractive surgery have been well documented by many studies, the induced biomechanical weakening of the cornea occurs because of the irreversible corneal alterations like flap creation and tissue removal. 3 In extreme cases, postoperative ectasia results from progressive corneal steepening and thinning, causing an irregular astigmatism and compromised visual results.4–7
Histological studies have described the unique ultrastructure of corneal stroma where the density and branching of collagen fibrils of the anterior stroma are significantly higher than posterior stroma which is more hydrated, giving the anterior part of the cornea stiffer mechanical properties. 8
LASIK is a flap surgery approach, in which a flap is created in the anterior part of corneal stroma using a micokeratome, with an intended flap thickness of about 100 μm; however, the attempted flap thickness may vary between 90 and 160 μm, depending upon the utilized flap creation method. The achieved flap diameter depends upon the corneal curvature and therefore will vary between 7.5 and 9.5 mm. After reflection of the flap, photo ablation treatment is performed in a 6.0 to 6.5 mm diameter optical zone in addition to 0.5 to 1.5 mm transition zone using excimer laser; and the flap is repositioned afterwards. 9
On the other hand, femtosecond laser small incision lenticule extraction (F-SMILE) does not require a flap creation; instead, a stromal lenticule is extracted through a 2 to 3 mm incision leaving the remaining anterior stroma and Bowman’s layer untouched. 10
Preoperative assessment of corneal biomechanics might be beneficial to select appropriate patients for refractive surgery, taking in consideration that some ectasia cases have been reported after refractive surgery in eyes with normal preoperative topography.11,12
In 2010, the CorVis ST (CST; Corneal Visualization Scheimpflug Technology, Oculus, Wetzlar, Germany), was released in the market for non-contact measuring of IOP. The device incorporates a high-speed camera that captures sequential horizontal Scheimpflug images of the cornea, through which both time and length of corneal inward and outward movements under the influence of a projected metered air puff are calculated; and many corneal biomechanical parameters are described accordingly.13,14
The aim of our study is to evaluate the changes in biomechanical properties of the cornea after two different modalities of laser corneal refractive surgery; LASIK and F-SMILE, using the CorVis ST device to compare the changes in different parameters in the Vinciguerra screening report and study the correlation between these changes and the change in central corneal thickness (CCT) at 6 months after refractive procedures.
Patients and methods
This is a prospective, randomized, unmasked, interventional comparative case series that was carried out at Elite Center (Tanta, Egypt) and started in July 2018. The study included candidates for refractive surgery who were 18 years of age or older, with stable refraction for at least 1 year. Every single candidate was fit to receive either one of the two procedures and was assigned to one of the two groups randomly: the first group (group A) received LASIK; and the second group (group B) received F-SMILE. Treated errors of refraction included myopia less than −8 D, astigmatism less than −4 D with a total spherical equivalent (SE) of −10 D or less. All LASIK procedures were performed by a single surgeon (H.A.S.); also, all F-SMILE procedures were performed by a single surgeon (A.M.G.).
We excluded individuals with: central corneal thickness <500 μm, calculated residual corneal bed <300 μm, progressive or unstable myopia, ocular diseases like severe dry eye, corneal opacity, keratoconus, iris irregularities, cataract, glaucoma, retinal detachment, systemic diseases like connective tissue diseases (e.g. lupus, rheumatoid arthritis) and insulin-dependent diabetes mellitus, systemic medications that are likely to affect wound healing (e.g. retinoic acid, steroids), history of prior ocular surgery or trauma and any suspected or irregular corneal topography (e.g. forme fruste keratoconus, pellucid marginal degeneration, irregular astigmatism). Contact lens wearers were instructed to stop using them for at least 2 weeks before the baseline examination.
Preoperative examination included: slit-lamp examination, fundus examination, IOP measurement, measurement of both uncorrected distance visual acuity (UDVA), and corrected distance visual acuity (CDVA) with glasses in the same lane using H type chart (ACP-8R Auto chart projector, Topcon Corporation, Tokyo, Japan) by the same doctor (E.A.A.); in addition to cycloplegic refraction.
Corneal tomography using Pentacam (Pentacam HR, Oculus, Wetzlar, Germany) and corneal biomechanics measurement using CorVis ST were performed by one masked technician. Corvis ST has a high speed Scheimpflug camera (4330 f/s) that covers 8.0 mm horizontally and records 140 images, showing corneal deformation in response to a metered air puff. Only acquisitions with a quality of scan (OK) were accepted for analysis.
Microkeratome-based conventional LASIK procedure was performed using Moria M2 microkeratome (Moria SA, Antony, France) to cut the flap using the disposable 90 µm head and the suction ring was chosen per the manufacturer’s nomogram based on the steepest keratometric value (K1). Achieved flap thickness was verified using an ultrasound pachymeter (SP-100 Handy Pachymeter, Tomey, Nagoya, Japan) to ensure a minimal residual stromal bed thickness of 300 μm after laser ablation. EX500 Allegretto excimer laser platform (WaveLight GmbH, Erlangen, Germany) was used to perform a wavefront-optimized treatment of myopia and astigmatism using a 6.5 mm optical zone with a 1.25 mm blend zone.
The VisuMax 500 kHz laser system (Carl Zeiss Meditec, Jena, Germany) was used to perform F-SMILE surgeries using the following parameters: small-sized disposable cone, 6.5 mm optical zone, 7.5 mm cap diameter, 100 µ cap thickness, 3 µ spot distance for lamellar cuts, and 2 µ for side cuts, 130 nJ spot energy, a minimum lenticule side cut thickness of 10 µ, a lenticule side cut angle of 130°, incision side cut angle of 70°, and 3 mm wide that was created superiorly for lenticule extraction.
The postoperative regimen of treatment was similar after both procedures and included: moxifloxacin 0.5% eye drops (Vigamox; Alcon, Fort Worth, TX, USA) four times daily for 1 week, prednisolone acetate 1% eye drops (PredForte; Allergan, Inc., Dublin, Ireland) four times daily for 1 week and then tapered on weekly basis and artificial tears (Systane Ultra, Alcon, Fort Worth, TX, USA) four times daily and whenever desired to alleviate any foreign body or burning sensation for at least 3 months.
Follow-up examinations were performed postoperatively on first postoperative day, 1 week, 1, 3, and 6 months postoperatively. Upon the 6 months’ visit, Pentacam and CorVis ST examinations were performed.
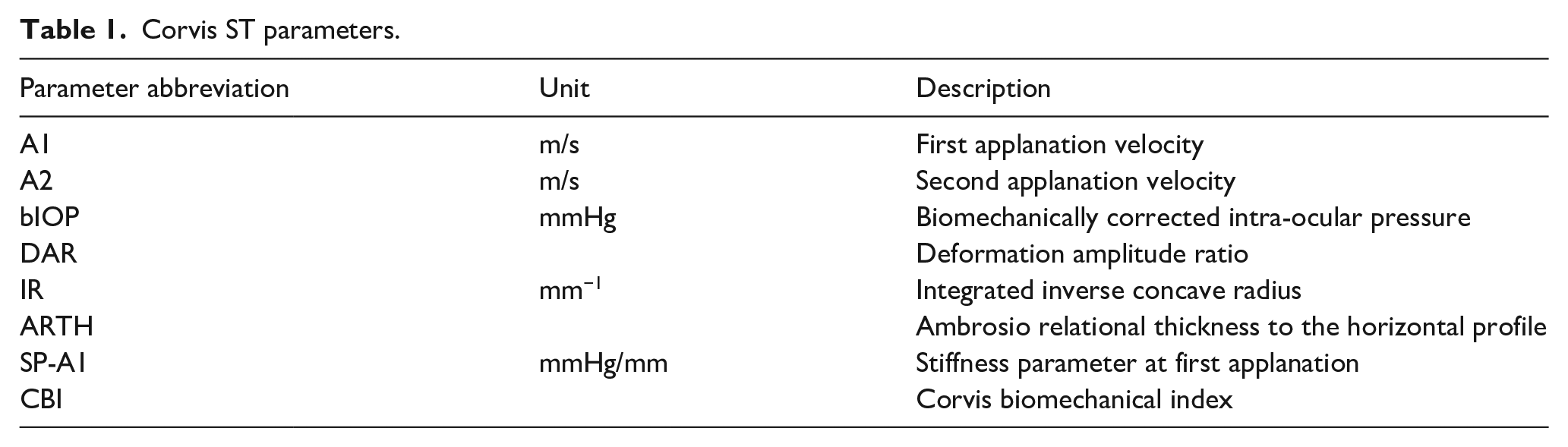
Preoperative demographic data (age, sex), preoperative spherical equivalent, preoperative, and 6 months postoperative flat and steep K reading values (K1 and K2) together with central corneal thickness (CCT) obtained from the Pentacam output; in addition to the parameters of Vinciguerra screening report of CorVis ST 14 (Table 1) were all collected and stored in a spreadsheet for further statistical analysis.
Corvis ST parameters.
Statistical analysis
Statistical presentation and analysis of the present study were conducted, using the mean, standard deviation, unpaired t-test, paired t-test, and linear correlation coefficient by SPSS V20 (IBM, Chicago, USA). P value of ⩽0.05 was used as a cut off value for significance of results.
Results
This study was conducted on 60 eyes of 30 patients who were randomly divided into two groups: the first group (group A) received LASIK (n = 30, 15 patients); and the second group (group B) received F-SMILE (n = 30, 15 patients).
The differences between the two groups regarding age, sex, and the mean value for preoperative SE were statistically insignificant (Table 2).
Age, sex, and preoperative spherical equivalent.
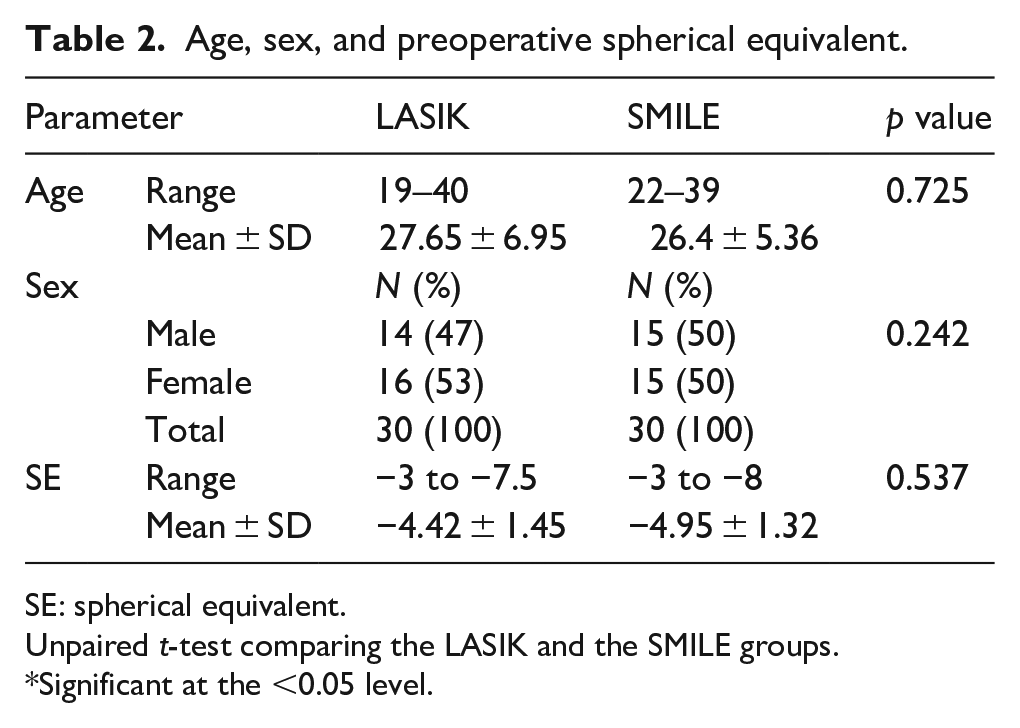
SE: spherical equivalent.
Unpaired t-test comparing the LASIK and the SMILE groups.
Significant at the <0.05 level.
No significant difference was recorded between both groups; neither preoperatively, nor postoperatively regarding mean K1, mean K2, and central corneal thickness (CCT). As expected, CCT decreased significantly after surgery in both groups (p < 0.001; Table 3). The achieved flap thickness in LASIK group (group A) was 115.0 ± 5.95 μm as measured intraoperatively using subtraction ultrasound pachymetry technique.
K1, K2, and CCT.
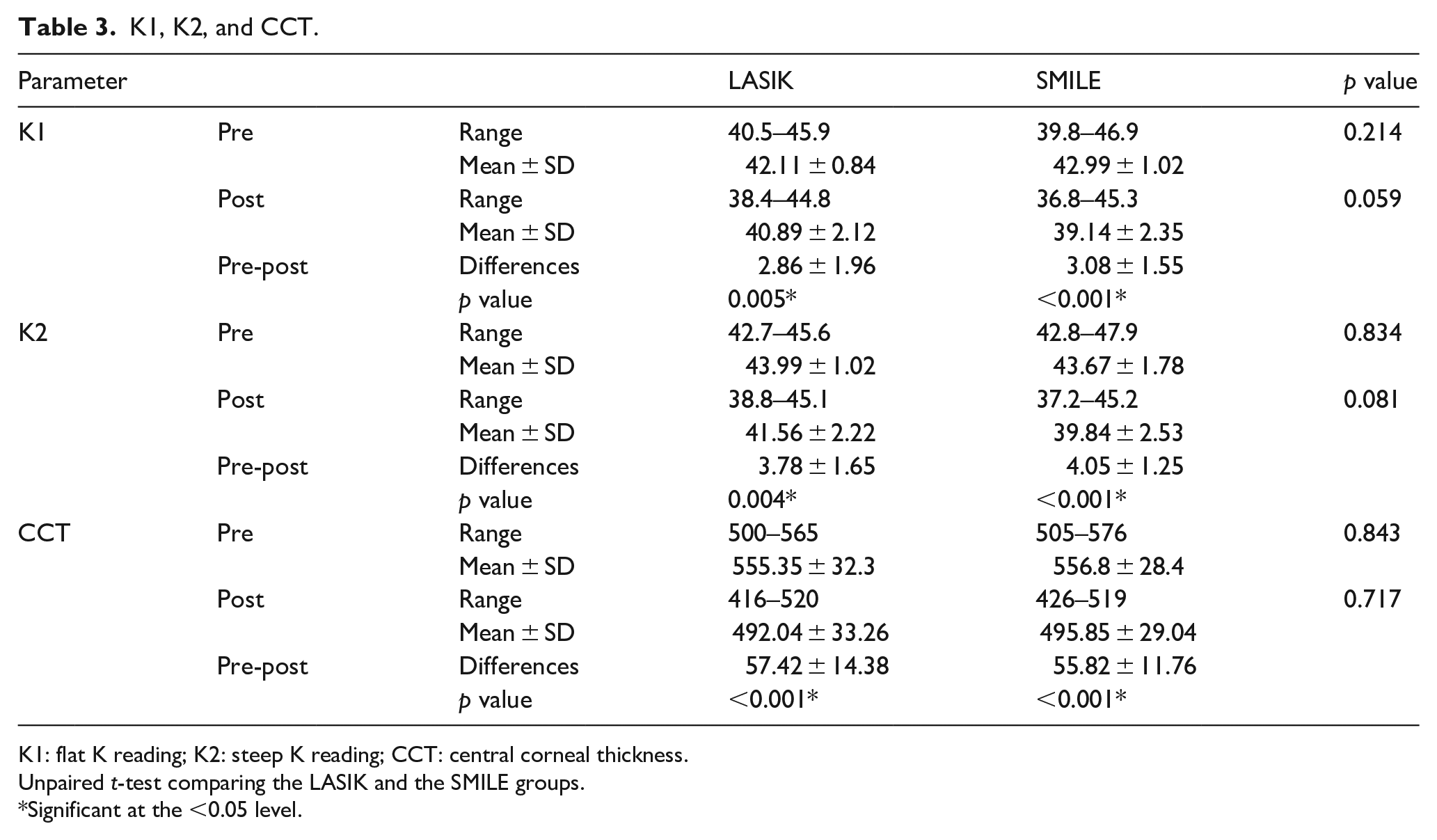
K1: flat K reading; K2: steep K reading; CCT: central corneal thickness.
Unpaired t-test comparing the LASIK and the SMILE groups.
Significant at the <0.05 level.
The biomechanically corrected intra-ocular pressure (bIOP) is a calculation of the intraocular pressure value after correction using the dynamic corneal response analysis. bIOP decreased insignificantly at 6 months by 0.762 ± 1.211 mmHg (p = 0.092) in group A, and significantly in group B by 2.52 ± 1.389 mmHg (p < 0.001). Although the difference recorded between the two groups preoperatively had been insignificant (p = 0.531); a significant difference was detected at 6 months postoperatively (p = 0.001).
First applanation velocity (A1) describes the inward movement of corneal apex at first applanation under the influence of air puff (ingoing phase), while second applanation velocity (A2) describes the outward movement of the corneal apex at the second applanation (outgoing phase). Six months postoperatively, A1 increased significantly in group A, but insignificantly in group B (p = 0.036, p = 0.314, respectively); on the other hand, A2 decreased insignificantly in both groups (p = 0.865, p = 0.321, respectively).
The deformation amplitude ratio (DAR) denotes the largest displacement of corneal apex at the maximum concavity; thus, stiffer corneas would have a lower value. DAR increased significantly from preoperative to 6 months postoperative values in both groups (p < 0.001, p = 0.022 for group A and group B, respectively) but the difference recorded between the two groups preoperatively and 6 months after surgery remained insignificant (p = 0.542, p = 0.461, respectively).
Integrated inverse concave radius (IR) is the radius of curvature during the concave phase of deformation; thus, higher values indicate stiffer corneas. IR increased significantly from preoperative to 6 months postoperative values in group A (p < 0.001) and insignificantly in group B (p = 0.557). Although the preoperative difference of IR parameter between the two groups had been insignificant (p = 0.681); it became significant at 6 months after surgery (p = 0.026).
Ambrosio relational thickness to the horizontal profile (ARTH) is the division of the thinnest corneal thickness value by pachymetric progression index; thus, a lower value indicates a thinner cornea and/or a faster thickness progression toward the periphery. ARTH decreased insignificantly from preoperative to 6 months postoperative values in both groups (p = 0.245, p = 0.695 for group A and group B, respectively) and the difference recorded between the two groups preoperatively and 6 months after surgery remained insignificant (p = 0.214, p = 0.928, respectively).
The stiffness parameter at first applanation (SP-A1) is the difference between the air-puff pressure at corneal surface and the bIOP divided by the deflection amplitude; thus, stiffer corneas are associated with higher values. SP-A1 decreased insignificantly from preoperative to 6 months postoperative values in group A by 8.89 ± 1.38 mmHg/mm (p = 0.637), while a significant decrease of 32.6 ± 4.39 mmHg/mm was detected in group B (p < 0.001). Although the difference in SP-A1 parameter recorded between the two groups preoperatively had been insignificant (p = 0.855); it became significant at 6 months postoperatively (p = 0.013).
Corvis biomechanical index (CBI) is obtained using logistic regression with combination of different dynamic Scheimpflug analyzer parameters, ranging from 0 (normal) to 1 (abnormal). CBI increased significantly from preoperative values to 6 months postoperatively (p < 0.001) in group A, but an insignificant increase was recorded in group B (p = 0.098). Although the difference in CBI between the two groups had been statistically insignificant preoperatively (p = 0.356); 6 months after surgery, a highly significant difference was evident (p < 0.001) (Table 4).
Corvis ST parameters.
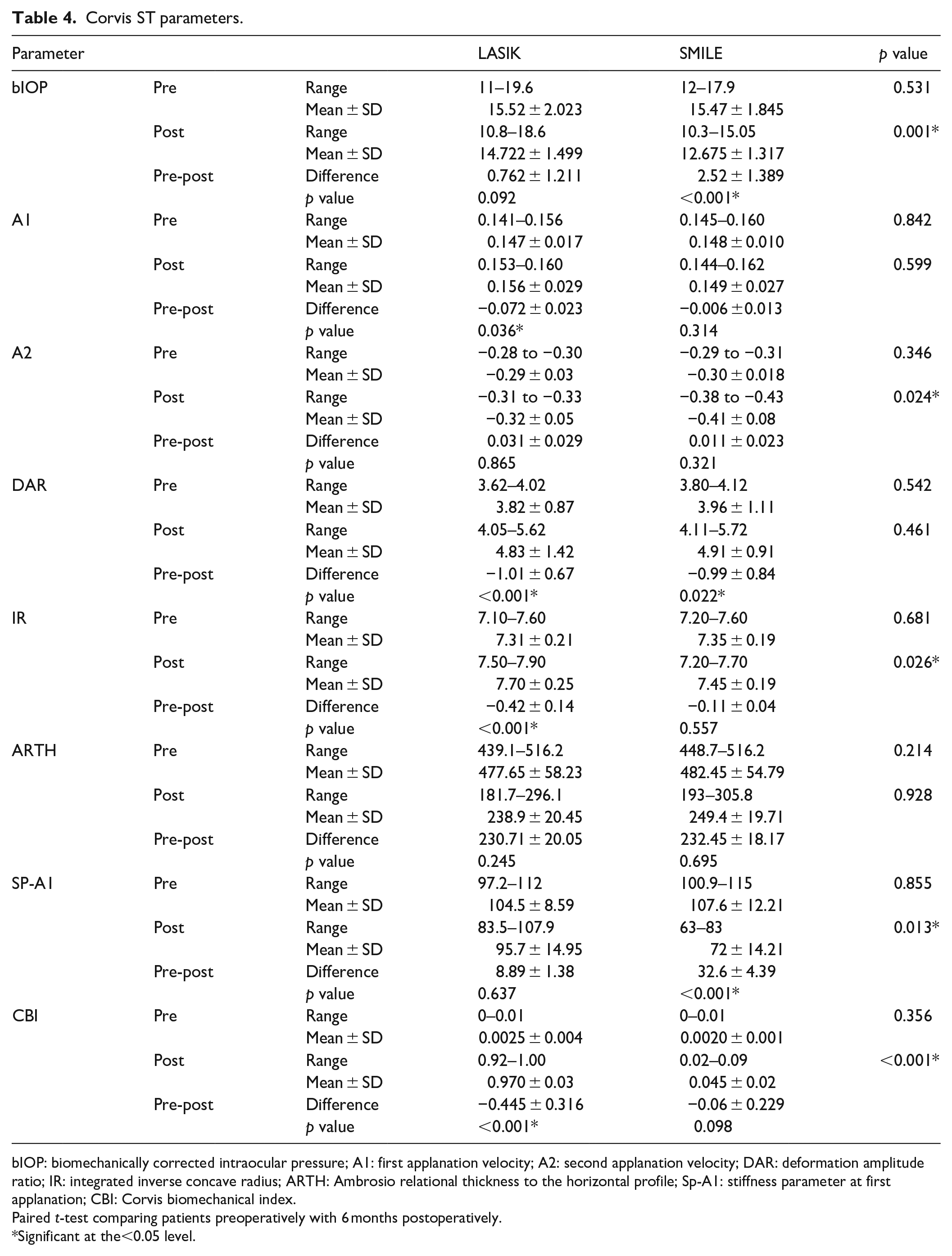
bIOP: biomechanically corrected intraocular pressure; A1: first applanation velocity; A2: second applanation velocity; DAR: deformation amplitude ratio; IR: integrated inverse concave radius; ARTH: Ambrosio relational thickness to the horizontal profile; Sp-A1: stiffness parameter at first applanation; CBI: Corvis biomechanical index.
Paired t-test comparing patients preoperatively with 6 months postoperatively.
Significant at the<0.05 level.
Interestingly, we found a significant correlation between the change in CCT at 6 months after surgery and the corresponding changes in DAR, IR, and ARTH parameters in both study groups (Table 5).
Correlation between change in CCT and changes in Corvis ST parameters.
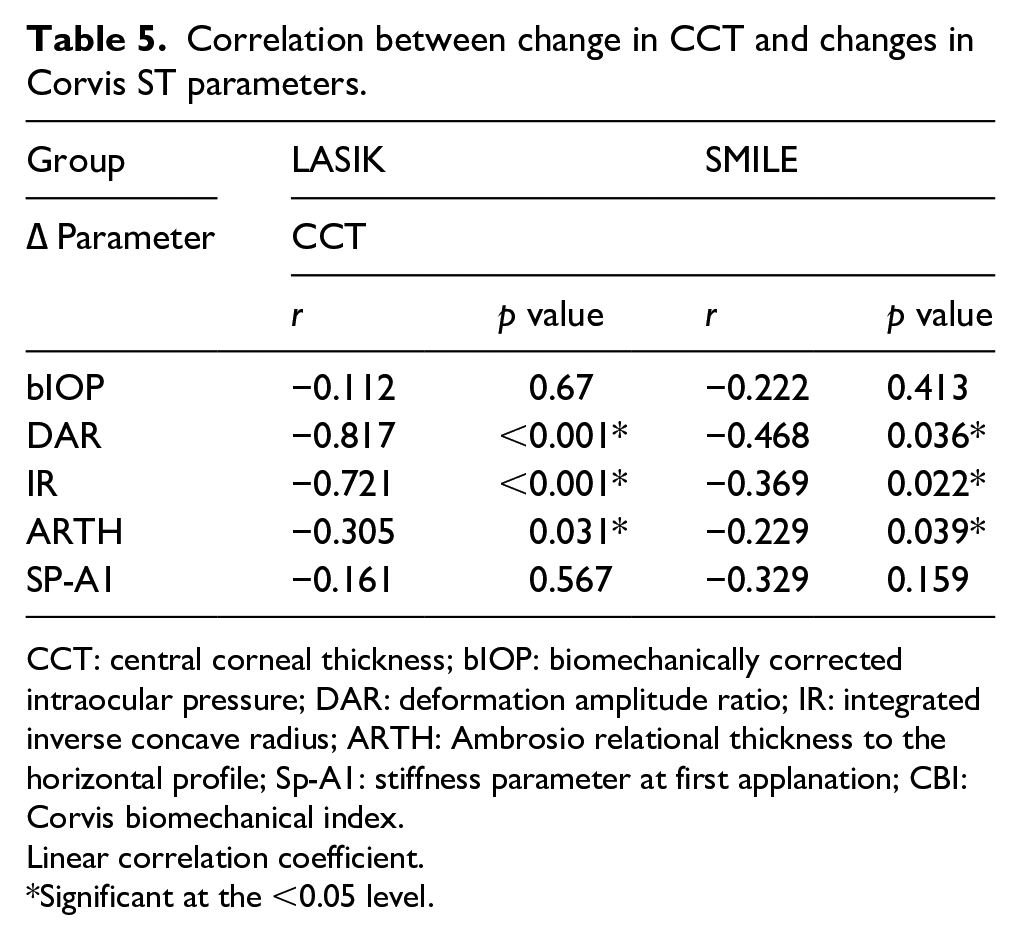
CCT: central corneal thickness; bIOP: biomechanically corrected intraocular pressure; DAR: deformation amplitude ratio; IR: integrated inverse concave radius; ARTH: Ambrosio relational thickness to the horizontal profile; Sp-A1: stiffness parameter at first applanation; CBI: Corvis biomechanical index.
Linear correlation coefficient.
Significant at the <0.05 level.
Discussion
Corneal refractive surgeries offer long-term solution and treatment for refractive errors like myopia and astigmatism. 15 One of the major difficulties in refractive surgery is the uncertainty about the risk of postoperative ectasia, even in absence of known risk factors. 11 By understanding the biomechanical properties of the cornea, the surgeon might be able to predict the outcome of surgery and avoid this devastating complication that has an estimated risk of 0.04% to 0.6% after LASIK. 16
Like most biological tissues, the cornea has viscoelastic properties. Hundreds of collagen lamellae transverse the cornea and are under tension due to loading by the intraocular pressure. The posterior part of corneal stroma was found only 39.3% as stiff as the anterior stroma. 17 Corneal biomechanics represent the interaction of three main factors: an external factor; the applied forces, and two internal factors; the viscoelastic properties of the corneal tissue in addition to the intraocular pressure (IOP). Disruption of these fibers by refractive procedure results in loss of tension and corneal expansion peripheral to the disruption and central flattening in the anterior cornea. 18
Flap creation in LASIK affects corneal biomechanics as stated in several studies. On the other hand, in F-SMILE procedure, a corneal stromal lenticule of a predetermined thickness is extracted through 2 to 3 mm incision without the need of creation of a flap, thus maintaining the integrity of the anterior corneal stroma.10,19
Many studies reported variations in flap thickness with mechanical microkeratome. Du et al. compared the Moria M2 90 head with two more heads and found that among many variables, achieved flap thickness was positively correlated with preoperative CCT only. 20 Their study included 60 eyes in each group, and the range of preoperative CCT in the Moria M2 90 head group was 485 to 616 μm. 20 In our study, the achieved flap thickness in LASIK group was 115.0 ± 5.95 μm; this smaller value of standard deviation in our study may be attributed to the smaller number of included eyes (n = 30), or the tighter range of preoperative CCT (500–565 μm).
On the other hand, the use of femtosecond laser does not only achieve a more predictable and uniform thickness of the cap, but also avoids the variation in flap diameter relative to mechanical microkeratome that tends to cut larger flaps in steeper corneas despite adjustment of the suction ring size and stop setting. 21 Those disadvantages associated with mechanical microkeratome cut could result in greater biomechanical weakening.
In theory, the SMILE procedure is expected to cause less corneal biomechanical weakening in comparison to LASIK for several reasons: first, more than 300° of Bowman’s membrane is incised in LASIK, compared to only around 30° in SMILE; second, the LASIK flap created by a micrkeratome extends deeper in the stiffer anterior collagen lamellae thus causing more stromal weakness; third, the difference in wound healing response would leave the cornea stronger after SMILE; and fourth, the smaller diameter of SMILE cap than LASIK flap would preserve the stronger peripheral corneal stromal collagen bundles in SMILE group.
CorVis ST system is equipped with an ultra-high-speed Scheimpflug camera to enhance the accuracy for detecting ectatic corneal diseases. Its value is determined on the grounds of an algorithm based on numerical simulations of dynamic corneal deformation. 22 Many studies have confirmed that CorVis ST is more helpful in outlining true biomechanical changes; so, we wanted to study the changes in CorVis ST parameters in attempt to understand the resulting changes in corneal biomechanics after LASIK and F-SMILE. 23
A study by Ahmed et al. found a significant increase in deformation amplitude with CorVis ST after both LASIK and SMILE, that was two times higher in LASIK group, indicating greater reduction in corneal biomechanical properties. 24
Elsheikh et al. studied 59 corneas from human donors aged between 30 and 99 years with a mean age of 76.0 ± 13.3 years and they found that corneas become stiffer with age. 25 In our study, this variable factor was eliminated by the younger age group and smaller age range of included candidates (19–40 years).
Because the differences between our two studied groups regarding potentially confounding variable factors like age, SE, K1, K2, and CCT before and after surgery were insignificant, we could analyze the dynamic corneal response parameters independently.
In our study, bIOP in group A showed a non-significant decrease from preoperative to 6 months’ postoperative values (0.762 ± 1.211 mmHg, p = 0.092), while in group B, there was a highly significant decrease (2.52 ± 1.389 mmHg, p < 0.001). Although the difference between the two studied groups was statistically insignificant preoperatively (p = 0.531), it became significant at 6 months postoperatively (p = 0.001).
These findings coincide with Lee et al. who reported on 64 patients who had F-LASIK and there was a non-significant decrease in bIOP after surgery (p = 0.138). 26 Also, Fernández et al. evaluated 43 eyes and reported a significant change in bIOP after F-SMILE procedure (14.68 ± 1.99 mmHg preoperatively and 13.30 ± 1.74 mmHg postoperatively, p < 0.001). 27
Chen et al. showed that the bIOP readings before and after F-SMILE was not correlated with CCT. 28 We had similar findings in our study, as there was no significant correlation between CCT and bIOP.
In our study, A1 velocity in group A showed a significant increase from preoperative to 6 months’ postoperative values of −0.072 ± 0.023 m/s (p = 0.036); and in group B, there was an insignificant increase of 0.006 ± 0.013 m/s (p = 0.314), which means slower corneal movements in response to the air puff, indicating a stiffer cornea after F-SMILE.
A2 velocity in both groups showed an insignificant decrease in the difference from preoperative values to 6 months postoperatively (0.031 ± 0.029 m/s, p = 0.865 and 0.011 ± 0.023 m/s, p = 0.321, respectively). There was a significant difference between both group at 6 months after surgery (p = 0.024).
Our findings are in agreement with Osman et al. who reported a significant decrease in A1 time after LASIK (p = 0.001) and no significant change after SMILE (p = 0.69), denoting stiffer corneas after SMILE. 29
With laser vision-corrective procedures, corneal tissue softening may occur not only due to reduction in corneal thickness because of tissue removal, but also due to interruption of the tension-bearing corneal stromal collagen lamellae, particularly during circumferential LASIK flap creation.
Zhang et al. described better corneal curvature stability after SMILE than F-LASIK and attributed that to postoperative corneal remodeling. They suspected that the creation of corneal flap results in keratometric flattening effect that regresses with wound healing, causing mild progressive corneal steepening and myopic shifting. 30
Eliasy et al. developed the stress-strain index (SSI), an algorithm to predict the cornea’s material behavior. Although SSI had a non-significant correlation with CCT (p > 0.05), the study addressed only corneas with normal topography and did not validate the algorithm on corneas with previous refractive surgery. 31
Similar to our results, Fernández et al. reported a significant correlation between changes in all CorVis ST parameters (except SP-A1) and the removed corneal thickness after SMILE (p < 0.05). 27
Osman et al. found by using CorVis ST that the deformation amplitude increased significantly in both groups, five times higher after LASIK than SMILE and concluded that F-SMILE had substantially decreased the corneal biomechanical properties. 29 Also, Lee et al. found that DA and IR increased significantly after F-LASIK (p < 0.001) and concluded that corneas became less resistant to deformation. 26
The findings of both studies are – to some extent – in agreement with ours, where A1 and IR changed significantly after LASIK procedures only (p = 0.036, p < 0.001, respectively); SP-A1 decreased significantly after F-SMILE only (<0.001); DAR changed significantly in both groups (p < 0.001, p = 0.022 in group A and group B, respectively); whereas the changes in ARTH were insignificant in both groups (p = 0.245, p = 0.695 in group A and group B, respectively). The above-mentioned changes refer clearly to a stiffer cornea after F-SMILE procedure.
CorVis biomechanical index (CBI) was introduced in attempt to standardize the available biomechanical parameters. In 2016, Vinciguerra et al. indicated that the CBI was highly sensitive and specific to differentiate between normal and keratoconic eyes. They suggested that a CBI value ⩾0.5 is associated with increased risk of development of corneal ectasia. 14
In our study, the difference in CBI from preoperative to 6 months’ postoperative values was significant in group A (−0.445 ± 0.316, p < 0.001), while in group B, the difference was insignificant (−0.060 ± 0.229, p = 0.098). Although the difference between the two studies groups was insignificant preoperatively (p = 0.356), at 6 months after surgery, the difference became highly significant between the two study groups (p < 0.001) which consolidates our previous findings of stiffer corneas after F-SMILE in comparison to LASIK.
Conclusion
The significant differences between our two groups at 6 months after surgery as regards bIOP (p = 0.001), IR (p = 0.026), SP-A1 (p = 0.013), and CBI (p < 0.001) suggest less influence of F-SMILE on corneal biomechanics in comparison to LASIK procedure. These differences are in favor of F-SMILE over LASIK for better stability of the corneal biomechanics and maintaining stiffer corneas postoperatively.
What was known
– Although laser refractive surgery as a popular choice for treatment of myopia has a well-documented safety and efficiency profile, in rare cases, postoperative ectasia may develop due to biomechanical weakening of the cornea.
– Because the exact etiology and pathogenesis of ectasia are not fully understood, it is a common practice for refractive surgeons to examine refractive surgery candidates for possible risk factors of ectasia like: low age, high errors of refraction, low preoperative corneal thickness, low residual stromal bed thickness, and abnormal corneal topography.
What this paper adds
– The combination of Pentacam and CorVis ST for preoperative screening of refractive surgery candidates can assist in better excluding individuals at risk for ectasia.
– The significant postoperative differences in some CorVis ST parameters highlight less influence of F-SMILE on corneal biomechanics in comparison to LASIK for better postoperative corneal stiffness and possibly lower risk of development of ectasia.
– All postoperative differences in CorVis ST parameters were significantly correlated with the removed corneal tissue, except bIOP and SP-A1; this suggests that both bIOP and SP-A1 can be used as indicators to assess the biomechanical properties of the cornea irrespective of corneal thickness or amount of tissue removed during corneal refractive surgery.
Footnotes
Clinical study approval
The study was approved by the research ethics committee at Faculty of Medicine, Tanta University, Tanta, Egypt.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Research involving human participants
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.