
Abstract
Purpose:
We reported the occurrence of a congenital unilateral huge peripapillary staphyloma in association with craniofacial clefts for the first time.
Case report:
A 1-year-old boy presented with a large defect on his left eyelid, a wide oblique columella nasi and an atypical wedge-shaped extension of the unilateral anterior hairline. Magnetic resonance imaging (MRI) examinations revealed there were cracks on his nasal septum, palate, and superior alveolar midline. Moreover, we surprisingly uncovered a gourd-shaped eyeball with the compressed optic nerve on the right side, while the right eye seemed normal from appearance. Under anaesthesia, fundus examination of the right eye showed a 15 mm-deep excavation surrounding the optic disc with defective choroid and dysplastic optic papilla. We reconstructed the left eyelid of the patient to protect his cornea and would make other solutions according to the results of follow-up.
Conclusion:
Peripapillary staphyloma and craniofacial clefts are two dissimilar rare congenital anomalies. In this patient, we firstly observed the co-existence of the two defects, which may provide the experience to the diagnosis and treatment of peripapillary staphyloma and craniofacial clefts. This case also gives us the pathogenic inspiration for further studies of peripapillary staphyloma and craniofacial clefts.
Introduction
Peripapillary staphyloma is a fairly rare nonhereditary congenital anomaly, which has a relatively normal optic disc located at the base of a deep fundus excavation. This abnormality of fundus is generally unilateral accompanied with poor vision.1–4 Craniofacial clefts are rare skeletal deformities, which have a multitude of clinical presentations. 5 To date, peripapillary staphyloma and craniofacial clefts are still little known. Herein, we present a case with these two deformities co-occurred and referred to the different eyes.
Case presentation
A 1-year-old boy presented to our department to thoroughly correct his eyelid defect. Partial tarsorrhaphy had been performed according to the diagnosis of craniofacial clefts at the local hospital. There was no history of consanguinity and teratogen ingestion, as well as no family history of congenital anomalies.
On examination, we found that the child had a remaining large coloboma on the left upper eyelid, an obvious wide oblique columella nasi, and an atypical wedge-shaped hairline extension on the left side (Figure 1). Definitely, cracks on nasal septum, palate and superior alveolar midline were found by magnetic resonance imaging (MRI). Surprisingly, MRI examination also revealed the existence of a gourd shaped right eyeball combined with a compressed optic nerve (Figure 2). Under anaesthesia, fundus examination of the right eye showed there was a 15 mm-deep excavation surrounding his optic disc with dysplastic optic papilla and pigmentary changes (Figure 3). No other abnormalities were detected in his left eye fundus and binocular anterior segment. Since he was only 1 year old, his visual acuity was not clearly assessed. According to the description of his parents, no abnormal performances of his vision had been observed since birth. His other systems were also well developed. Taken together, the diagnosis of this case is corrected to peripapillary staphyloma accompanied with craniofacial clefts, which has not been reported before.

A 1-year-old boy presented with a large coloboma on the left upper eyelid, a wide oblique columella nasi and an atypical wedge-shaped anterior hairline extension. Note that tarsorrhaphy had been done at the local hospital and cornea exposure still existed.
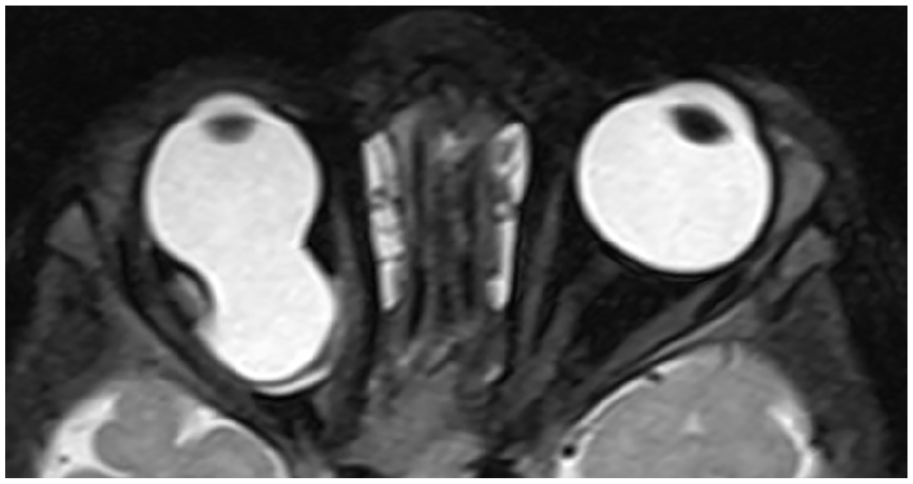
Magnetic resonance imaging showed a gourd shaped right eyeball with the displaced optic nerve. Measuring the peripapillary staphyloma was 15-mm depth and 3.2-mm breadth.
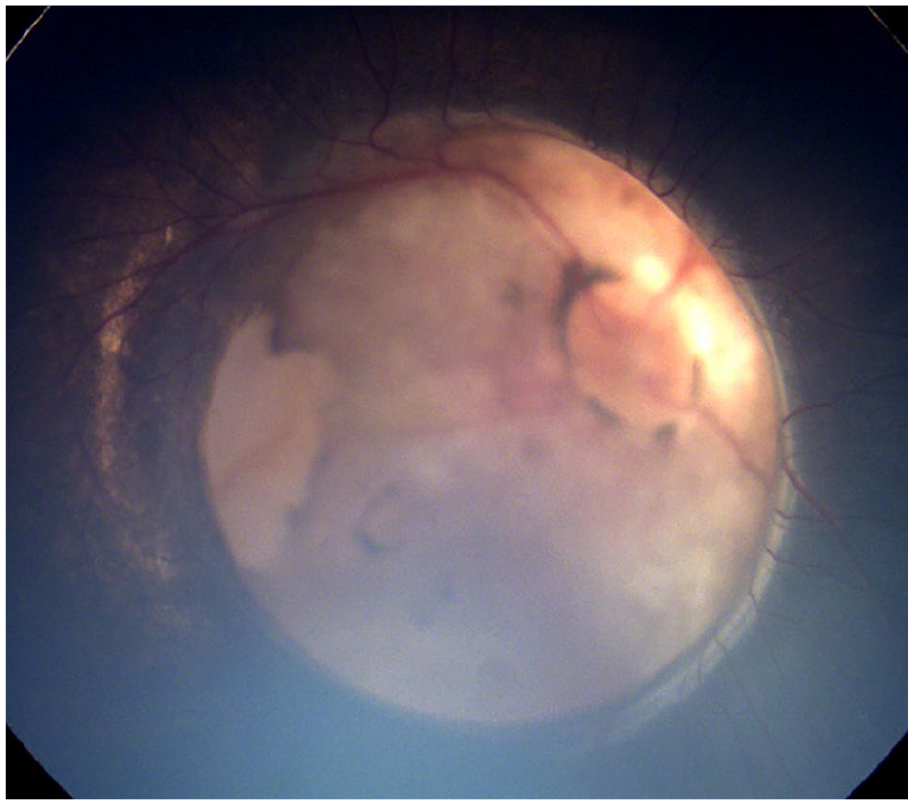
Fundus photograph showed a quite deep excavation surrounding the optic disc with dysplastic optic papilla and pigmentary changes. Note that there was a huge peripapillary staphyloma in the right eye and the walls of the staphyloma around the optic disc was abnormal. The peripapillary retina and disc excavation could not be focused simultaneously.
As far as we know, such a large peripapillary staphyloma with the depth of 15 mm has not been reported.1,2,6 Moreover, peripapillary staphyloma is rarely associated with systemic abnormalities and unilateral peripapillary staphyloma accompanied with craniofacial clefts, which harm the different eyes in one patient, is also the first report. 6
Discussion and conclusion
Peripapillary staphyloma is a rare, nonhereditary type of congenital optic disk anomaly, which includes a deep excavation surrounding a relatively normal-appearing optic nerve head at the base of the staphyloma.1,6–8 The exact pathophysiology of peripapillary staphyloma is unknown and its clinical features are thought to be the result of the incomplete development of the posterior sclera from neural crest cells occurring near the fifth month of gestation.7–9 Reported peripapillary staphyloma cases highly vary in depth, while it is the first time to record a 15 mm-deep one.1,7,10 Because of the small number of reported cases, the correlation between the size of peripapillary staphyloma and the prognosis, such as the vision acuity, could not be definitely confirmed statistically.
Peripapillary staphyloma is easily confused with the other congenital anomalies of the optic disc, such as optic disk pits, the morning glory syndrome, optic disk colobomas, optic nerve aplasia, and hypoplasia, as they may all contain excavations.2,11 As reported, optic disk colobomas are associated with serous or rhegmatogenous retinal detachments, while retinoschisis may not present in cases of peripapillary staphyloma.4,7 The morning glory anomaly often accompanies a shallower excavation with a centrally located prepapillary glial tuft and straightly radiated vessels.8,9 It has been reported that morning glory and peripapillary staphyloma might co-exist in one case. 12 Therefore, the identification of peripapillary staphyloma should usually exclude similar excavated optic disc anomalies based on different tiny phenotypes.
Peripapillary staphyloma patients were reported to be accompanied with other ocular abnormalities, such as congenital cataract, microphthalmia, primary vitreous hyperplasty, persistent pupillary membrane, and morning glory anomaly of ipsilateral or contralateral eye.6,8 Furthermore, acquired diseases, such as retinal detachment or refractive errors, were not rare in peripapillary staphyloma patients.3,13 Peripapillary staphyloma is generally combined with poor vision, while a bilateral case with normal visual acuity was once recorded. 6 Eyes with peripapillary staphyloma may hardly achieve visual improvement by routine occlusion therapy. 6 In this case, no treatments for the peripapillary staphyloma eye were taken, based on the situation of the patient and deferring to his parents, and the outcome of peripapillary staphyloma can not be defined.
Craniofacial clefts are rare, congenital, skeletal malformations with an incidence of about 1.4 and 4.9 per 100,000 live births, so their diagnosis and therapies are technology and experience dependent.14,15 To date, the most widely accepted classification of craniofacial clefts was proposed by Tessier, using the orbit as a central landmark.5,16 The clinical features of craniofacial cleftsthis in this case were nearest to be defined as Tessier number 1 and number 10. The Tessier number 1 cleft contains the lip cleft, the alveolar cleft, and the clefts travel through the alar dome, parasagittal nasal dorsum, medial aspect of the eyebrow. The Tessier number 10 cleft includes a coloboma of the middle third of the upper eyelid, a wedge-shaped anterior hairline extension and a divided eyebrow. Although craniofacial clefts accompanied by other ocular anomalies, including orbital hypertelorism, symblepharon, corneal opacification, congenital microphthalmia, and cryptophthalmia have been reported, the concurrent peripapillary staphyloma of the other eye has never seen. 17
The etiology of craniofacial clefts is believed to be multifactorial.16,17 Environmental factors, including radiation, influenza A2, toxoplasmosis, maternal metabolic abnormalities, drugs and especially amniotic bands can be involved in the formation of craniofacial clefts. 16 The disruption of normal development during gestation has revealed to be the common reason of craniofacial clefts and peripapillary staphyloma, while the relationship between craniofacial clefts and peripapillary staphyloma on pathogenology is still unknown and worthy further studies.6,8,14
The therapeutic programs for treating craniofacial clefts must be tailored according to the needs of patients. For this case, the initial priority is to reconstruct a cosmetically acceptable upper eyelid to provide corneal coverage and then restoration of a normal appearance should also be considered. 18 After operating blepharoplasty, the other therapies for craniofacial clefts and peripapillary staphyloma should be gradually determined according to the needs of patients, especially the vision problem over the follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shanghai Municipal Education Commission-Gaofeng Clinical Medicine Grant Support (20161421) and the Science and Technology Commission of Shanghai (17DZ2260100).
Consent for publication
Written informed consents were obtained from the parents for publication of this case report and accompanying images.