
Abstract
Purpose:
To report the different uncommon pathogenesis of three cases of severe vertical restrictive strabismus associated with progressive unilateral proptosis with similar clinical features.
Methods:
Case series of three patients who presented to the Orbit Outpatient Service of Policlinico Gemelli with a history of left progressive unilateral proptosis, slowly worsening vertical strabismus and the left eye fixed in downward position. A thorough hematologic work up was performed. All patients underwent complete abdomen ultrasonography, orbital contrast enhanced magnetic resonance imaging, forced duction test under general anesthesia, and orbital biopsy.
Results:
Patients were 30, 60, and 46 years old respectively. MRI showed left inferior rectus enlargement in two cases and superior rectus enlargement in one case, with contrast enhanced combined muscle belly and tendon enlargement in all cases. Patients underwent forced duction test, muscle weakening (in two cases), and muscle biopsy with histopathologic examination. The superior rectus appeared infiltrated by an undifferentiated high-grade pleomorphic sarcoma, whereas the two inferior recti were positive for idiopathic orbital inflammatory disease with fibrosis areas and neuromuscular choristoma, respectively.
Conclusion:
Although proptosis and acquired vertical restrictive strabismus are most commonly associated with thyroid associated orbitopathy (TAO), they can also be a manifestation of many other conditions and the differential diagnosis can be particularly challenging. The three reported cases presented indeed with similar clinical features but had three distinct underlying orbital etiologies, two of which were extremely uncommon.
Keywords
Introduction
An acquired vertical restrictive strabismus associated with proptosis, secondary to extraocular muscles (EOM) infiltration, is often a consequence of thyroid associated orbitopathy (TAO), that is by far the most frequent cause of single extraocular muscle enlargement (EME) with restrictive strabismus.1,2 However, single EME can be secondary to a wide range of non-thyroid local and systemic diseases, with inflammatory, vascular or neoplastic origin.1,3–5 Due to the frequently overlapping clinical and imaging features, the differential diagnosis can be difficult, particularly as, to date, no pathognomonic findings, either clinically or radiologically, have been clearly identified in literature. 3
We report a case series of three patients who presented with unilateral severe, slowly worsening, vertical strabismus, and proptosis. The clinical and radiological features showed single EME. Orbital biopsy revealed three different and uncommon histological causes.
Case description
Sixty-eight patients with vertical restrictive strabismus were referred to the Orbit Unit at Fondazione Policlinico Gemelli of Rome between May 2017 and May 2019. A diagnosis of TAO was made in 38 cases (55.9%). Eighteen patients (26.4%) were diagnosed with blow-out fractures, two cases (2.9%) with post-vitreoretinal surgery strabismus. A diagnosis of orbital neoplastic disease was made in five cases (7.3%) and five cases showed an inflammatory orbital infiltration (7.3%), Three out of 10 neoplastic and inflammatory cases were retrospectively selected for this case series because of similar clinical onset and peculiar radiological signs hiding three uncommon different conditions.
All patients underwent first line ophthalmological assessment, with evaluation of visual acuity at distant fixation (logMAR), cover test with Berens prism bars, and exophthalmometry.
First-line assessment of proptosis with vertical restrictive strabismus should also include thyroid function tests blood investigation and neuroimaging to rule out a TAO. When TAO is improbable, further blood tests should be runned: serum Angiotensin Converting Enzyme (ACE), C-reactive protein (CRP), rheumatoid factor, serum IGg4 levels, anti-neutrophil cytoplasmic antibodies (ANCAs), and a complete abdomen ultrasonography to rule out multiple organ involvement.
When clinical and radiologic findings are inconclusive, a surgical biopsy is needed.1,3,6
All the selected patients underwent forced duction test under general anesthesia and orbital biopsy of the involved muscle with histopathologic examination. All muscle biopsies were performed involving belly, insertion, and perimuscular sheaths.
All patients gave informed written consent to publish their cases, after the purpose of the study was explained.
Patient 1
A 30-year-old man presented with a 6-month history of left proptosis, inferior globe displacement and diplopia, with a palpable mass in the superior orbit (Figure 1(a) and (b)). Details on ophthalmological evaluation are summarized in Table 1. MRI showed left superior rectus (SR) involvement with moderate irregular contrast enhancement (Figure 1(c)). An incisional biopsy was performed, revealing an undifferentiated high-grade pleomorphic sarcoma of the orbit (Figure 1(d1–d4)). To stage the tumor, an abdomen ultrasonography and a total body positron emission tomography/computed tomography (PET/CT) were performed, with negative results. An exenteratio orbitae was performed and an adjuvant radiotherapy was planned.
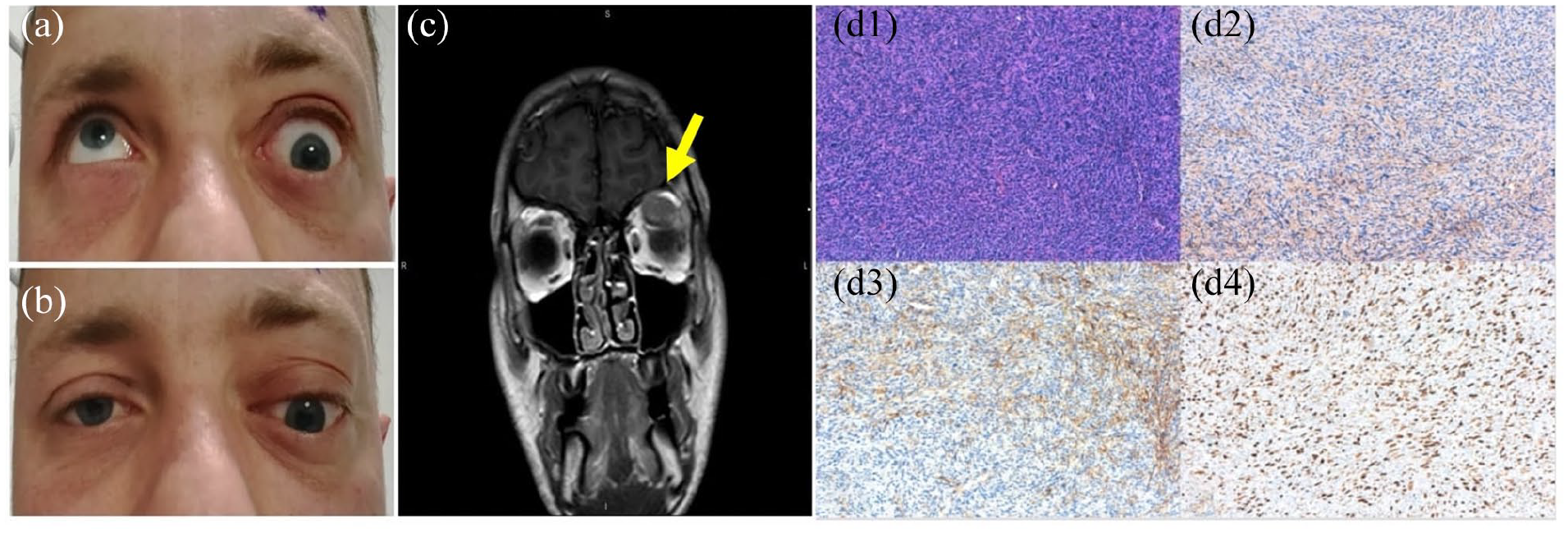
Patient 1. (a) Upgaze position; (b) primary position (right eye fixating eye); (c) T1-weighted MRI image, left superior rectus enlargement iso-hypointense to extraocular muscles compressing the eye globe (yellow arrow). (d1–d4) High-grade malignant mesenchymal neoplasia with a herringbone pattern of growth composed of spindle and epithelioid cells with marked nuclear pleomorphism and bizarre giant cells (d1). There were focal areas of necrosis. Lesion shows focal CD99 and SMA immunoreactivity (d2 and d3) with a proliferation index of 75% (Ki67%) (d4) (hematoxylin-eosin, original magnification 100× [d1]; original magnification 100× [d2–d4]).
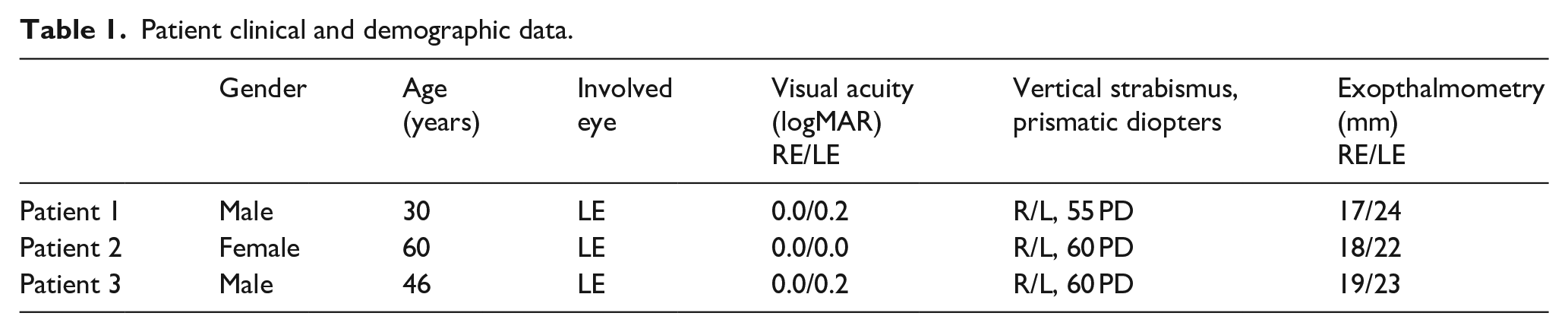
Patient clinical and demographic data.
Patient 2
A 60-year-old female presented with a 5-month history of progressive proptosis associated with downward displacement of the left globe with inability to elevate the eye (Figure 2(a) and (b)). She complained of diplopia in downward and primary position and pain on LE movements (Table 1 summarizes ophthalmological findings).
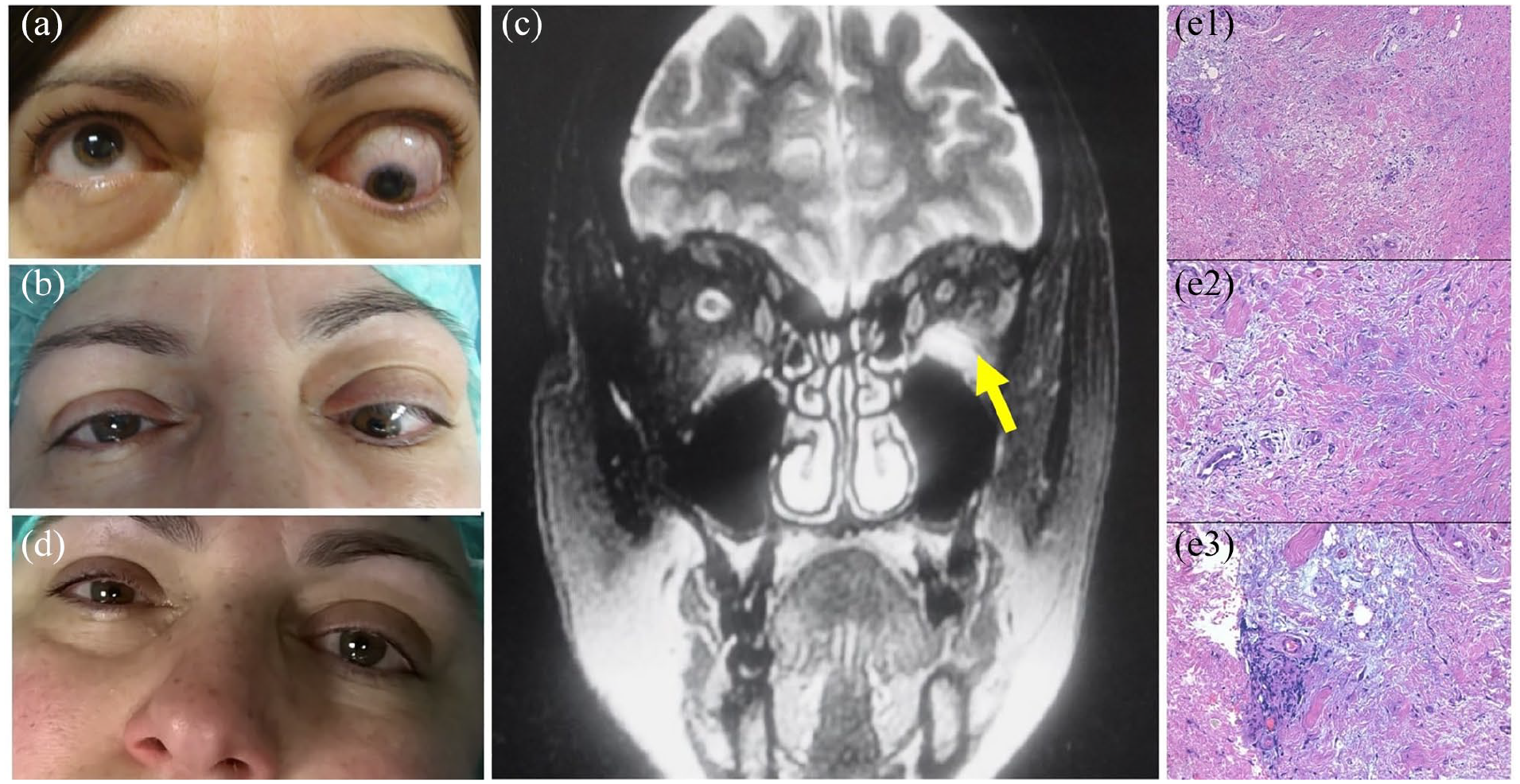
Patient 2. (a) Upgaze position; (b) primary position (right eye fixating eye); (c) T2-weighted MRI image, left inferior rectus enlargement with contrast enhancing spreading to perimuscular tissues (yellow arrow); (d) postoperative primary position; (e1–e3) fibro-connective tissue with areas of mixedema, also perivascular, and mild lymphoplasmacellular inflammation mainly perivascular (hematoxylin-eosin, original magnifications 100× [e1] and 200× [e2 and e3]).
Orbital MRI showed enlargement and intense enhancement of the belly and insertion of the left IR (Figure 2(c)). On forced duction test, the LE was fixed in downward position. The IR was detached from the scleral insertion and widely recessed (10 mm by hang-back sutures). Postoperatively, the patient had a single vision in primary position and in downward gaze position. An incisional biopsy of the left IR was also performed. Histopathologic findings revealed lymphoplasmacellular infiltration, mainly perivascular, with a fibro-connective component (Figure 2(e1–e3)). Immunohistochemical staining was negative for IgG4 plasma cells. IgG4 serum levels were normal and an abdomen ultrasonography ruled out multiple organ involvement.
Systemic glucorticoids (GCs) were administered, with mild clinical improvement (Figure 2(d)) and reduction of the IR on MRI at 6, 12, and 18 months of follow-up. At 12 months, an incisional biopsy confirmed the histopathologic diagnosis, excluding a lymphoproliferative monoclonal disorder.
Patient 3
A 46-year-old male with a 1-year history of tenderness and pain of the left inferior orbit, presented with inferior displacement of the left globe (Figure 3(a) and (b)).
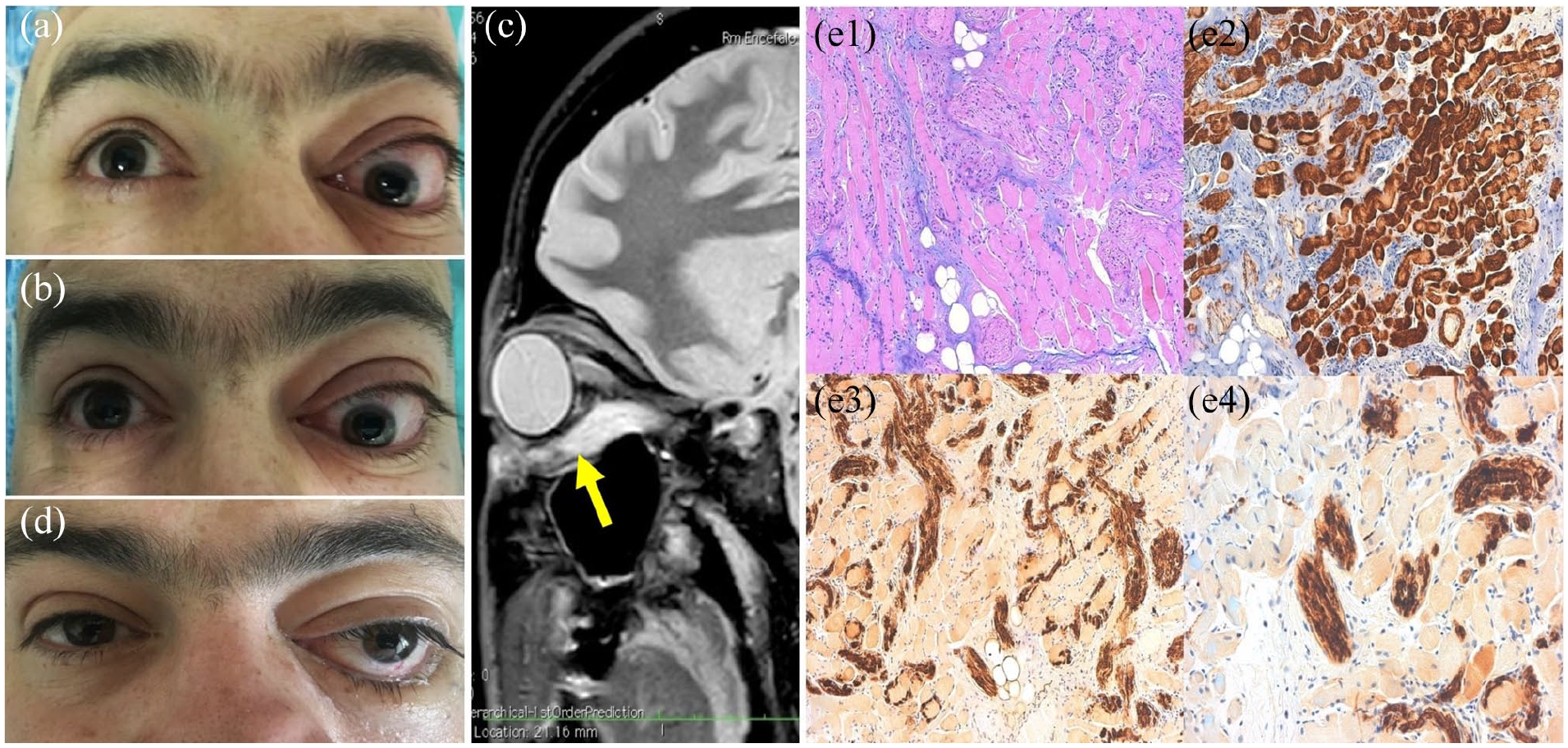
Patient 3. (a) Upgaze position; (b) primary position (right eye fixating eye); (c) T2-weighted MRI image, left inferior rectus insertion and belly enlargement with contrast enhancing (yellow arrow); (d) postoperative primary position (severe left inferior eyelid ptosis); (e1–e4) neuromuscular choristoma, with benign proliferation of mature skeletal muscle fibers and haphazardly arranged tangles of regenerating nerve in a myxoid stroma (e1). Lesion shows HHF35 immunoreactivity in the muscular component (e2) and S100 immunoreactivity in the neural component (e3 and e4) (hematoxylin-eosin, original magnification 100× [e1]; original magnifications 100× [e2 and e3] and 200× [e4]).
The patient, upon suspicion of orbital myositis, had previously received a high dose of oral steroids (1.5 mg/kg of prednisone per day for 1 week, then tapered off in 4 weeks) without improvement.
Ocular examination showed left inferior fornix injection and pain on LE movement (findings from ophthalmic evaluation are listed in Table 1). On orbital MRI, a left IR enlargement of both belly and insertion was found, with irregular enhancement involving perimuscular tissues (Figure 3(c)). Forced duction test showed severe restriction of elevation of the LE. The IR was widely weakened: the muscle was detached from the scleral insertion and widely recessed (12 mm by hang-back sutures) in the attempt to allow a field of single binocular vision; at the same time an incisional biopsy of the muscle anterior half was performed. Histopathologic evaluation revealed a neuromuscular choristoma (Figure 3(e1–e4)). Postoperatively the patient’s left eye position improved but a severe inferior eyelid ptosis developed as a consequence of the augmentated IR recession (Figure 3(d)). Follow-up MRI at 6 and 12 months showed a stable situation.
Discussion
Vertical restrictive strabismus, with a typical limitation of upgaze, associated with proptosis is most commonly induced by TAO. 2 Lacey et al. analyzed 1849 cases and reported that 95% were due to TAO, while only 5% were associated with other causes, with inflammatory conditions being the main cause of non-thyroid EME, followed by vascular processes. 1 Other authors analyzed the differential distribution of causes of non-thyroid EME. In particular, Shafi et al. reported a higher incidence of malignancy with lower incidence of inflammatory disease, suggesting to perform systemic imaging in all cases of isolated non-thyroid EME. 5
Other Authors reported that EME is suggestive of inflammatory diseases when associated with orbital and eye movement pain and painful diplopia.3,4,6
On MRI, orbital lymphoma and inflammatory disease often share similar features, appearing T1- and T2-hypointense or T2- mildly hyperintense, with homogeneous contrast enhancement. 7 EOM metastases can appear diffuse or nodular, usually hypointense on T1-weighted and iso-hyperintense on T2-weighted sequences, with variable contrast enhancement. 7
First-line assessment of proptosis with vertical restrictive strabismus should begin with thyroid function blood tests and neuroimaging to rule out a TAO. When TAO is improbable, further blood tests should be runned. However, a histopathologic examination is often needed.2,3 In our case series, we reported three cases with similar clinical and radiological presentation, hiding three peculiarly different diagnoses.
Patient 1
Soft tissue sarcomas are heterogeneous tumors showing mesenchymal differentiation. One subtype, undifferentiated pleomorphic sarcoma (UPS) is tumor formerly known as malignant fibrous histiocytoma (MFH), that encompasses the morphologic manifestation of a variety of poorly differentiated tumors. Diagnostic criteria have varied due to advancements in cytogenetics and immunohistochemistry. 8
MFH rarely occurs as a primary orbital tumor. To the best of our knowledge, less than 30 cases of orbital MFH have been reported and never infiltrating EOM. 9 Orbital MFH can be aggressive, causing intracranial invasion, local recurrence, and distant metastases with poor prognosis. 9 Although wide resection is the treatment of choice, tumors of the head pose functional problems that often make complete resection difficult. Therefore, adjuvant or neo-adjuvant radiotherapy and/or chemotherapy must be considered in these patients. 8
Patient 2
In this case, the clinical and radiological features together with the histological picture were potentially suggestive of a diagnosis of IgG4-related disease. Nevertheless, serum IgG4 levels were normal and immunohistochemical staining negative for IgG4 plasma cells. A diagnosis of idiopathic orbital inflammatory disease (IOID) was made. IOID is characterized by pleomorphic cellular infiltrate with varying degrees of fibrosis; any orbital structure can be involved, with orbital fat, lacrimal gland, and extraocular muscles representing common sites of involvement.3,4
The diagnosis is of exclusion and it is often made on the basis of clinical response to corticosteroids. 4 Significantly, many different orbital lesions, including TAO and malignancy, may respond to corticosteroids, hence a histologic diagnosis is considered pivotal by most clinicians. Patients with an unsatisfactory GCs response require additional immunosuppressant drugs and low dose radiotherapy. 3
Patient 3
Neuromuscular hamartomas (NH) or choristomas, also known as benign triton tumors, are rare tumors composed of mature neural and skeletal muscle tissue, with about 20 cases reported in the literature.
Sites of predilection include the large peripheral nerves. Very rarely, these tumors occur in the head and neck region, arising either in the central cranial nerves, with aggressive behavior, or in the smaller peripheral nerves, presenting as asymptomatic slow-growing skin nodules.
Orbital NH are exceedingly rare. Four intraorbital cases were described, likely arising from the oculomotor nerve, or in association with EOM.10,11
Due to the rarity of the lesion, the diagnosis is challenging and there are no accepted treatment guidelines. Tumor excision was reported, more aggressive for central types, conservative for peripheral tumors and in case of orbital involvement, so as to preserve visual function and binocular cooperation. Although the prognosis seems excellent, recurrence has been reported, warranting through follow-up.
Conclusion
Although proptosis and acquired vertical restrictive strabismus is most commonly associated with TAO, it may also be a manifestation of many other conditions and the differential diagnosis can be particularly challenging. No evidence of high circulating thyroid hormone levels, single muscle enlargement, muscle insertion involvement, and no evidence of lid retraction with lateral flare should put on alert and suggest further blood tests, complete abdomen ultrasonography and orbital biopsy with histopathologic examination.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.