
Abstract
Purpose:
To assess the incidence of ocular hypertension (OHTN) following penetrating keratoplasty (PKP) versus deep anterior lamellar keratoplasty (DALK) corneal transplant surgeries, and to assess the impact of indication for transplantation versus surgery type on OHTN development.
Methods:
A retrospective study of 76 eyes of 76 patients who underwent PKP or DALK between 1 January 2009 and 1 September 2014. Data included: preoperative intraocular pressure (IOP), indication and type of surgery, post-surgical IOP at 1 to 5, 14 to 21 days, 3, 6 months, 1 year and at the last follow up. Primary outcome was post-operative OHTN (defined as IOP >21 mm Hg).
Results:
A total of 13 patients (17.1%) developed OHTN of whom 9 (20.45%) underwent PKP and 4 (12.5%) DALK (p = 0.33). OHTN occurred after an average of 16.46 ± 8.47 months (0.1–58 months). Twenty-one keratoconus patients (39.62%) underwent PKP and 32 (60.37%) underwent DALK. Patients with indications other than keratoconus all underwent PKP. Keratoconus patients were less likely to develop OHTN (9.43% vs 34.78%, p = 0.02). Among patients developing OHTN, mean age of the non-keratoconus group was significantly higher (63.25±16.7 vs 33 ± 10, p = 0.01). No significant difference in OHTN among keratoconus patients undergoing DALK versus PKP (12.5% vs 4.76%, respectively, p = 0.35) was found. PKP was associated with less OHTN in keratoconus eyes (4.76% vs 34.78%, p = 0.02).
Conclusion:
Patients who underwent keratoplasty due to keratoconus are at a lower risk to develop OHTN than those who underwent surgery for other indications.
Keywords
Introduction
Glaucoma is one of the more severe complications that can occur following keratoplasty and may lead to permanent vision loss.1,2 In addition, it increases the risk for endothelial cell loss, 3 and constitutes the second most common cause of corneal graft rejection. 4
The incidence of glaucoma following penetrating keratoplasty (PKP) varies between 10% and 35%, 5 while the incidence of glaucoma following deep anterior lamellar keratoplasty (DALK) varies between 0% and 9%. 6 Reported risk factors for OHTN following keratoplasty include inflammatory disease, anterior synechiae, history of glaucoma and combined procedure. 7
The purpose of the current study was to determine the incidence of OHTN following PKP and DALK and to assess the impact of the indication for transplant versus type of surgery on the development of OHTN.
Materials and methods
All data for the study were collected and analyzed in accordance with the policies and procedures of the Institutional Review Board of the Bnei Zion Medical Center and the tenets set forth in the declaration of Helsinki.
This is a retrospective study that included patients who underwent PKP or DALK surgery between January 2010 and September 2014. In cases in which both eyes of a patient underwent keratoplasty, the right eye only was included. The following were excluded from the study: patients with a history of glaucoma, trauma history in the operated eye and those with incomplete follow up. Data collected from the patients’ charts, included: demographic data, pre-operative intraocular pressure (IOP), indication for corneal transplantation, type of surgery, post-operative IOP at Days 1 to 5, 14 to 21, 3 months, 6 months, 1 year and IOP at the last follow up examination. IOP was measured using a Tono-Pen XL (Reichert, Inc, Depew, NY).
For the purposes of this study, OHTN was defined as any IOP > 21 mm Hg.
Surgical technique
All surgeries were performed by a single surgeon (R.S.M) at the Department of Ophthalmology at Bnai Zion Medical Center, Haifa, under general anesthesia. DALK procedures were performed using the Anwar Big Bubble technique. 8 The average donor corneal button diameter was 8 mm (7.5–8.5 mm). The average recipient corneal bed diameter was 0.25 mm smaller than the graft. The cornea was sutured with a combination of interrupted and continuous sutures or with interrupted sutures only.
After surgery, Ofloxacin 0.3% and Dexamethasone 0.1% eye drops were administered five times daily for 1 week. The antibiotic was discontinued 1 week after the surgery. The topical steroid was tapered by one drop every month, until once a day, which was continued for the duration of 2 years post operatively. Following DALK, the Dexamethasone 0.1% was replaced with fluorometholone 0.1% once per day, after the first post-operative year.
Data collection
Data collected from patients’ records included: age, gender, indication for the surgery, the operated eye, IOP before and after the surgery (as detailed above), post-surgical complications including graft rejection and significant post-surgical inflammatory response. The objective of taking note of these complications was to assess the association between increased steroid dosage and the risk of developing OHTN.
Statistical analysis
The incidence of OHTN in the various groups was assessed using the generalized estimating equations method, taking into account data from both eyes. Assessment of risk factors for the development of OHTN was performed using regression analysis based on the Cox linear regression model. All statistical tests were performed using SPSS (version 22, IBM Inc., Illinois, USA). Significance level was set at p ⩽ 0.05. Continuous data are shown as mean ± standard error or mean.
Results
Overall, the study included 76 eyes of 76 patients, 47 (61.84%) males and 29 (38.15%) females, with an average age of 40.6 ± 19.7 years. Demographic data, the indication for surgery and the type of surgery are shown in Table 1. The mean follow-up period was 13.36 ± 11.57 months.
Indication for corneal transplantation, demographic characteristics and type of surgery.
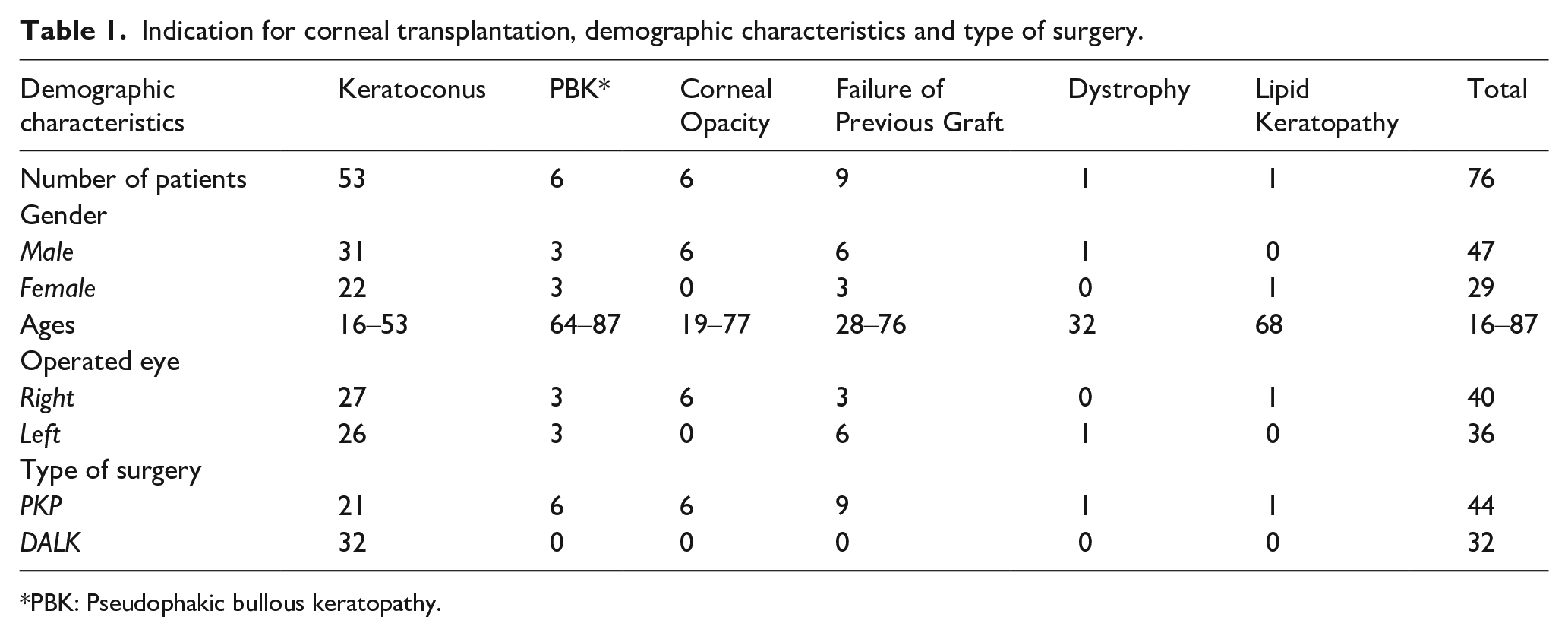
PBK: Pseudophakic bullous keratopathy.
OHTN was detected in 13 patients (17.1%), of whom 9 (20.45%) had undergone PKP and 4 (12.5%) had undergone DALK. The difference was not statistically significant (p = 0.33) (Figure 1). The elevated intraocular pressure was detected after an average of 16.46 ± 8.47 months (range: 0.1–58 months) postoperatively.
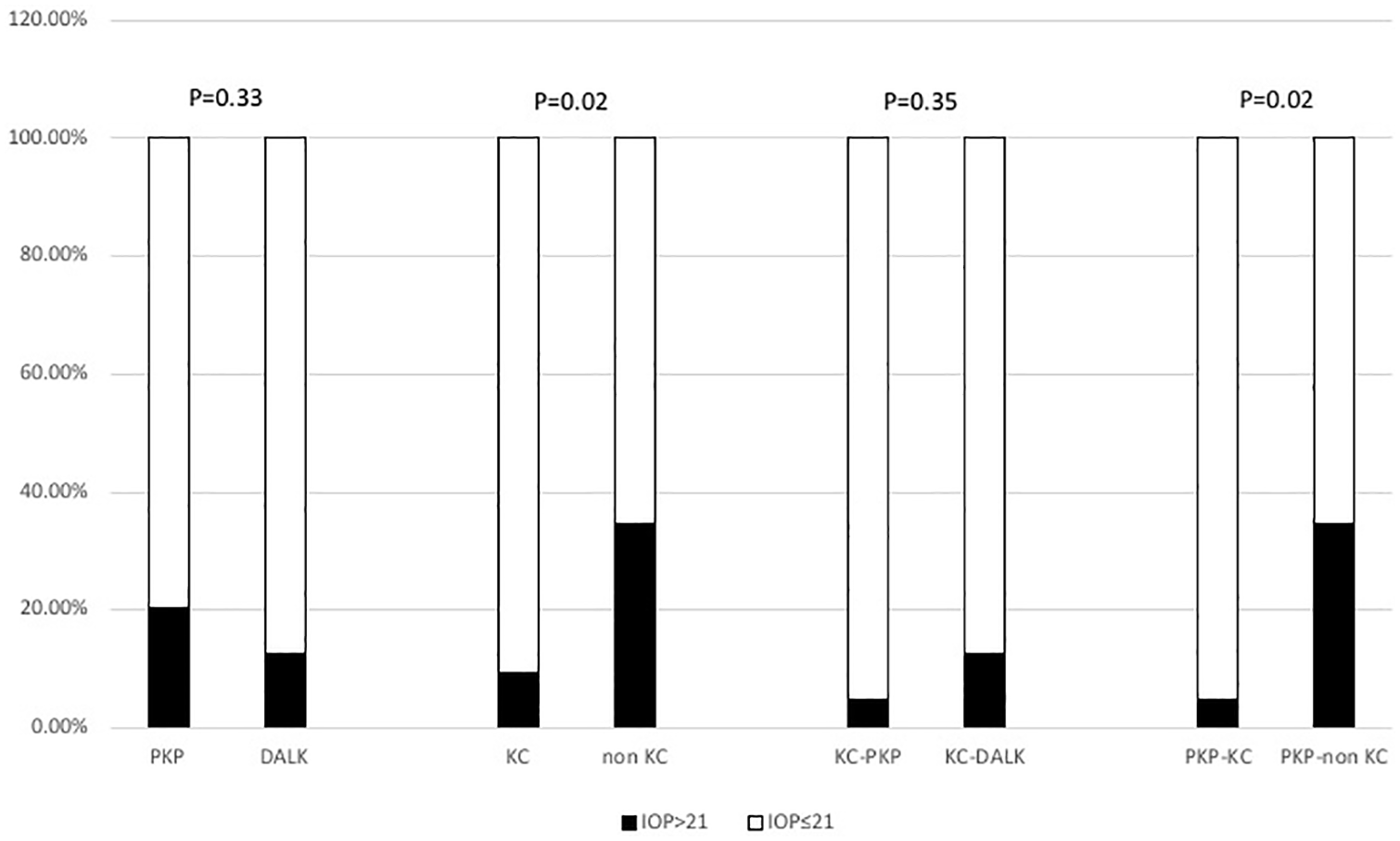
Comparison of ocular hypertension (IOP>21) between the following groups: PKP versus DALK, KC versus non-KC, Keratoconus patients: PKP versus DALK, and PKP: KC versus non-KC.
Patients were categorized into two groups according to the indication for transplantation: keratoconus and non-keratoconus groups. Five (9.43%) patients from the keratoconus group developed OHTN, as opposed to 8 (34.78%) patients from the non-keratoconus group. This difference was statistically significant (p = 0.02) (Figure 1). Within the OHTN group, the mean ages of the keratoconus and non-keratoconus patients were: 33 ± 10 years and 63.25 ± 16.7 years, respectively (p = 0.01).
A total of 21 keratoconus patients (39.62%) underwent PKP, compared to 32 (60.37%) who underwent DALK. When we compared the two procedures for keratoconus patients, we found that of the patients who developed OHTN, 4 (12.5%) had undergone DALK, as opposed to one patient (4.76%) who had undergone PKP (p = 0.35) (Figure 1).
Nine of the patients who underwent PKP (20.45%) developed IOP >21. Of these, one was a keratoconus patient (4.76%), as opposed to eight who did not have keratoconus (34.78%) (p = 0.02) (Figure 1).
Discussion
Ocular hypertension following keratoplasty can lead to glaucoma which is one of the most serious complications following corneal transplantation. Post-surgical glaucoma is difficult to diagnose and treat. Glaucoma causes graft rejection if misdiagnosed and not treated promptly, 9 as well as optic nerve damage and blindness.
The pathophysiology of OHTN following PKP includes a number of mechanisms: the use of corticosteroids, damage to the angle and the trabecular meshwork, suturing method and peripheral anterior synechiae (PAS) 1 which could develop in part due to leakage from the surgical incision and hypotony in the presence of inflammation.
Survey of the literature reveals that the prevalence of glaucoma following PKP surgery is high, compared to DALK surgery,10,11 since the latter is in fact an extraocular procedure. There is also a tendency to use less potent steroids for a shorter period of time following DALK compared to PKP, given the lower risk for graft rejection associated with DALK.12,13 It is important to bear in mind, however, that the main indication for DALK surgery is keratoconus, 14 the patients therefore being young and free of ocular co-morbidities, while the range of indications for PKP is broader including older patients suffering from additional diseases. It is therefore possible that the difference in the prevalence of glaucoma following DALK as compared to PKP is related to the complexity of the indication for the surgery rather than to the actual procedure.
The aim of the current study was to assess the incidence of IOP elevation following PKP and DALK surgeries and to determine whether the indication or the type of operation contribute to the development of post- operative OHTN.
Fewer patients developed OHTN after DALK compared to PKP, though the difference is not statistically significant. However, we found that patients who underwent surgery due to keratoconus developed OHTN at a significantly lower incidence rate than those who underwent surgery for other indications. This difference between keratoconus and non-keratoconus patients, was also significant within the group of patients who underwent PKP, strengthening the hypothesis that the indication for surgery contributes more to post-surgical OHTN than the type of the keratoplasty procedure. A number of studies in the literature support the hypothesis that the indication for corneal transplantation, in addition to other risk factors, influences the post-surgical development of OHTN. In a retrospective study of 1905 eyes that underwent keratoplasties for various indications, risk factors that significantly correlated with increased incidence of post-operative OHTN included: preoperative glaucoma, penetrating keratoplasty, lens status after the operation (higher risk for aphakic eyes) and intraocular lens exchange or removal during the operation. Of note, keratoconus was not associated with higher incidence of elevated intraocular pressure. 15 Similarly, Kirkness et al. reviewed 1122 penetrating keratoplasties and found that keratoconus was associated with the lowest incidence of post keratoplasty glaucoma. 16 On the other hand, a study by JC Fan et al., 17 reported considerably a higher rate of post keratoplasty OHTN (32%) in keratoconus patients. In their study they included patients who underwent PKP only, which can explain the higher incidence of elevated post-surgical pressure. However, this is a non-comparative study, therefore, the outcome cannot be attributed to the indication, neither to the surgical procedure. Additionally, in the current study, the mean age of non-keratoconus patients, was significantly higher than the keratoconus group. Older age is a well-known risk factor for progression to glaucoma from OHTN, 18 and in various studies, was associated with OHTN and glaucoma development following corneal transplantation. Raj et al. 19 reported a significant correlation between age > 40 and post-keratoplasty glaucoma development. Similarly, Kirkness et al. 20 found older age to be associated with higher risk of glaucoma development following keratoplasty. In our study, besides the indication, older age explains the higher rate of post keratoplasty OHTN development as opposed to the younger group of keratoconus patients.
Other studies have addressed the type of surgery as a risk factor for developing OHTN. In a ten years retrospective study performed by Zhang et al., 21 the reported incidences of OHTN and secondary glaucoma were significantly lower for the DALK group than for the PKP group (1.3% vs 46.2% and 0% vs 9.6%, respectively). The authors explained this difference as arising from the fact that PKP is an intraocular procedure, as opposed to DALK, which is an extraocular non-invasive procedure. However, the indications for the operations in these groups were not analyzed in this study to assess for potential correlation with post-operative OHTN.
In our study, comparison of the two surgical procedures in keratoconus patients showed, contrary to expectations, that more patients undergoing DALK developed post-surgical OHTN (12.5% of those undergoing DALK) compared to PKP (4.76% of those who undergoing PKP) (Figure 1). Review of data shows that two of the patients developed OHTN after DALK during the first month following the operation, after which IOP levels returned to normal. One patient who developed OHTN at a later stage was treated post-operatively with a higher dosage of steroids, due to sub epithelial infiltrates and suspected rejection. Therefore, it is still important to closely monitor IOP in patients who undergo lamellar keratoplasty.
Various studies have shown that an additional surgery combined with corneal transplantation elevates the risk for OHTN.22,23 In our study, five patients (6.57%) underwent an additional surgery combined with corneal transplantation. While conclusions cannot be drawn based on a small number of patients, it is worth noting that three out of these five patients (60%) developed post-surgical OHTN.
This study is subject to certain limitations. Its retrospective nature makes it vulnerable to certain biases such as selection bias which we believe was dealt with sufficiently by including all consecutive patients that met the inclusion\exclusion criteria. The follow up course was relatively brief which therefore warrants performing comparative studies with a longer follow-up period, in order to determine the risk factors for OHTN following various methods of corneal transplantation. Despite statistically significant results, the numbers of patients included in the various comparison groups might not be sufficient to draw clinical conclusions. A larger study population is needed to validate the clinical significance of the primary and secondary outcomes.
In summary, keratoconus is associated with lower incidence of OHTN following keratoplasty compared to other corneal diseases mandating lamellar or full thickness cornea transplantation. Interestingly, it seems that the lower risk of developing OHTN after DALK is related to the indication rather than the type of surgery. Awareness of risk factors helps in limiting the risk for the development of OHTN and increase the success rates following corneal transplantation. Patients undergoing corneal transplant surgery due to indications other than keratoconus require closer post-surgical IOP monitoring. However, keratoconus patients can also develop post-surgical OHTN particularly when exposed to risk factors. Therefore, careful monitoring of IOP in this group is imperative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.