
Abstract
Purpose:
To compare refractive surgery outcomes in patients with different periods without contact lenses prior laser surgery.
Materials and methods:
Patients included in this study underwent myopic keratorefractive laser surgery between January 2005 and December 2014. Patients were divided into three groups based on the duration of time passed free of soft contact lens wearing prior to final preoperative evaluation and surgery (<24 h, 1–3 days or >3 days). Spectacle wearers served as a control group. Postoperative safety index, efficacy index and % of eyes within 0.5 D of the four groups were compared. A general linear model was used to compare main outcomes while adjusting for age, gender, preoperative measurements, and procedure type (LASIK vs PRK).
Results:
Overall, 19,747 eyes were included. Soft contact lenses were worn by 42.3% (<24 h: 4.8%, 1–3 days: 18.5% and >3 days: 19.0%) and spectacles by 57.7% prior to surgery. In the PRK group, after adjusting for differences in baseline variables, the <24-h group had a significantly lower efficacy index than all the other groups. There were no significant differences between groups in terms of % eyes within ±0.5 D of intended correction (p = 0.55) or safety index (0.20). In the LASIK group, after adjusting for differences in baseline variables, there were no significant differences between groups in all primary outcomes.
Conclusion:
Soft contact lenses should be removed at least 24 h prior to final preoperative evaluation and refractive surgery, especially for patients undergoing PRK.
Introduction
Many candidates for refractive surgery use soft contact lenses (SCL) which may induced changes in keratometry, corneal astigmatism, and topographic alterations induced by the contact lenses.1–5 The accuracy of these preoperative measures affect corneal refractive surgery outcomes. 6 Thus, prior to undergoing elective keratorefractive surgery, it is common practice to advise patients to remove contact lenses in order to allow for precise preoperative assessment and measurements.
SCL material and duration of wear can affect the time required for resolution of corneal changes after SCL wear discontinuation.7–10 While no specific guidelines are given, SCLs discontinuation for at least 2 weeks before consultation was recommended by the United States Food and Drug Administration. 11 Whereas, SCL discontinuation for 1 day before consultation was recommended by the Royal College of Ophthalmologists in the United Kingdom. 12 However, there are no guidelines for duration of SCL discontinuation before the refractive surgery. In current clinical practice, there is a wide variability among refractive surgeons related to the recommended time period to discontinue SCLs before surgery. Most surgeons agree that patients wearing SCLs should discontinue SCLs for at least 3 to 7 days before final refractive assessment and surgery.13–15
Our study purpose of this study was to compare refractive surgery outcomes in patients with different periods of time without contact lenses prior to preoperative evaluation and surgery.
Materials and methods
This study was approved by the ethics committee of the Barzilai Medical Center.
Study participants
Patients who underwent myopic LASIK or PRK from 1 January 2005 until 31 December 2012 at the Care-Vision Laser Centers, Tel-Aviv, Israel were included in this retrospective study. Patients were included if they were ⩾18 years of age, demonstrated refractive stability for 1 year, were without ocular hypertension, no rigid contact lens wearing in the past year, no previous ophthalmic surgery and no systemic comorbidities that may affect outcomes. Patients were excluded if they had myopia greater than 12 diopters or cylinder greater than 6 diopters. Only patients with a follow-up time of 3 months or more following PRK or 1 month or more following LASIK were included in this study.
Data collection
The following data were extracted from the medical files of patients who met the inclusion\exclusion criteria: age, gender, type of contact lenses used, time free from contact lenses prior to examination, refractive measurements, and visual acuities. Of note, the preoperative data included relates to the final refractive measurements obtained at the day of surgery. For cases in which both eyes were eligible only the right eye was included.
Groups
Patients were divided into three groups based on the duration of time passed free of soft contact lens wearing prior to the final preoperative evaluation which was performed at the day of surgery (<24 h, 1–3 days or >3 days). Spectacle wearers, defined as patients that had not worn contact lenses in the past year, served as a control group. Postoperative safety index, efficacy index, and deviation from target refraction of the four groups were compared. In the PRK group this was based on measurements 3 to 6 months following surgery and in the LASIK group based on measurements 1 to 6 months following surgery.
Surgical technique
All patients underwent either microkeratome assisted LASIK or alcohol assisted PRK (the choice of which was left to the surgeon) in a similar manner as previously described by us. 16 The common practice in our institution is not to perform LASIK when the Central corneal thickness (CCT) is less than 500 µm. Patients were routinely examined the day after surgery as well as 1 week, 1 month, 3 months, 6 months, and thereafter as necessary.
Statistical analysis
Data were analyzed with the Minitab Software, version 17 (Minitab Inc., State College, PA). For comparison of multiple group averages one way analysis of variance was used. For the analysis of categorical variables, Chi-Square was used. A multivariate general linear model was performed in an attempt to determine whether time free of contact lens remained significantly associated with safety index, efficacy index, and deviation from target refraction after accounting for differences between groups at baseline. In all analyses a two-sided p value <0.05 was considered statistically significant.
Results
Overall, 19,747 were included in the final analysis. The age of the participants was 25.8 ± 5.8 years and 56.6% were male. The mean spherical equivalent was −3.86 ± 2.09 D (range −12 to −0.50 D). Soft contact lenses were worn by 42.3% and spectacles by 57.7% prior to final preoperative evaluation and surgery. Although all patients were instructed to discontinue contact lenses at least 3 to 5 days prior to final preoperative examination, 4.8% discontinued their use <24 h prior to examination, 18.5% discontinued 1 to 3 days and 19.0% discontinued >3 days before examination.
Entire cohort
Table 1 depicts the results of the univariate analysis when comparing baseline and type of procedure of the groups. Briefly, the spectacle group was slightly older, had a higher proportion of males, a lower preoperative spherical equivalent, larger cylinder, and lower proportion of PRK treatments. In univariate analysis, the <24-h group had a significantly lower safety index (p = 0.02) and efficacy index (p = 0.007). After adjusting for baseline differences between groups (general linear model) there were significant differences in terms of safety index (p = 0.02) and efficacy index (p = 0.002) but not with % of eyes within ±0.5 D from target (p = 0.30). Specifically, the <24-h group had a significantly lower safety index (Figure 1) and efficacy index (Figure 2) than each of the other individual groups. No statistically significant difference in % eyes within ±0.5 D from intended correction was found between the <24-h group and the other groups.
Preoperative data and primary outcomes – entire cohort.

P* - ANOVA and chi square wherever appropriate.
P** - General Linear model and Binary Logistic Regression accounting for differences between groups at baseline.
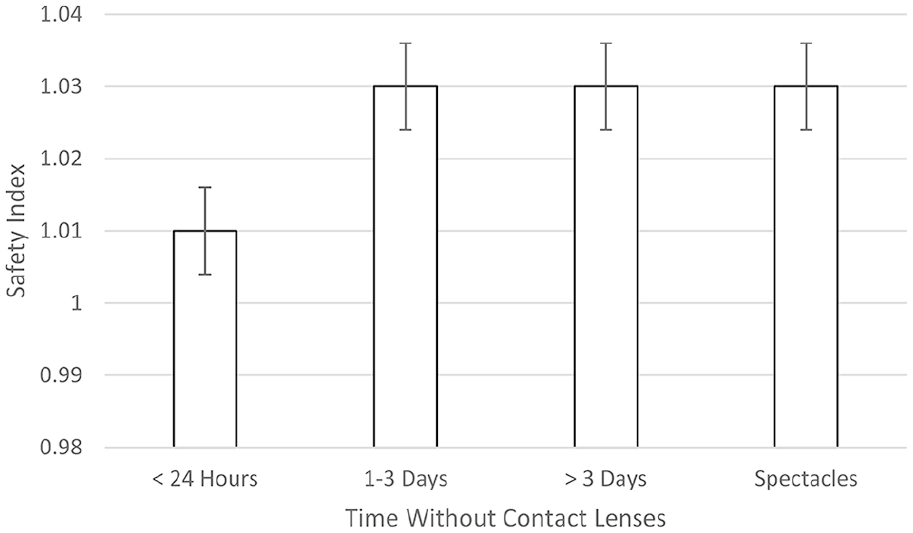
Safety index. The safety index of the different contact lenses free groups. The <24 h without contact lens wear group had a significantly lower safety index than all of the other groups.
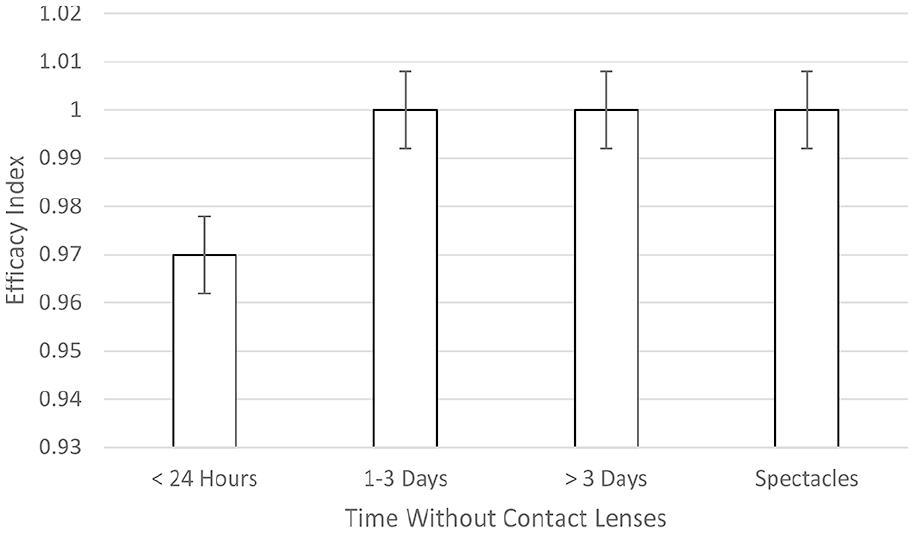
Efficacy index. The efficacy index of the different contact lenses free groups. The <24 h without contact lens wear group had a significantly lower efficacy index than all of the other groups.
PRK only
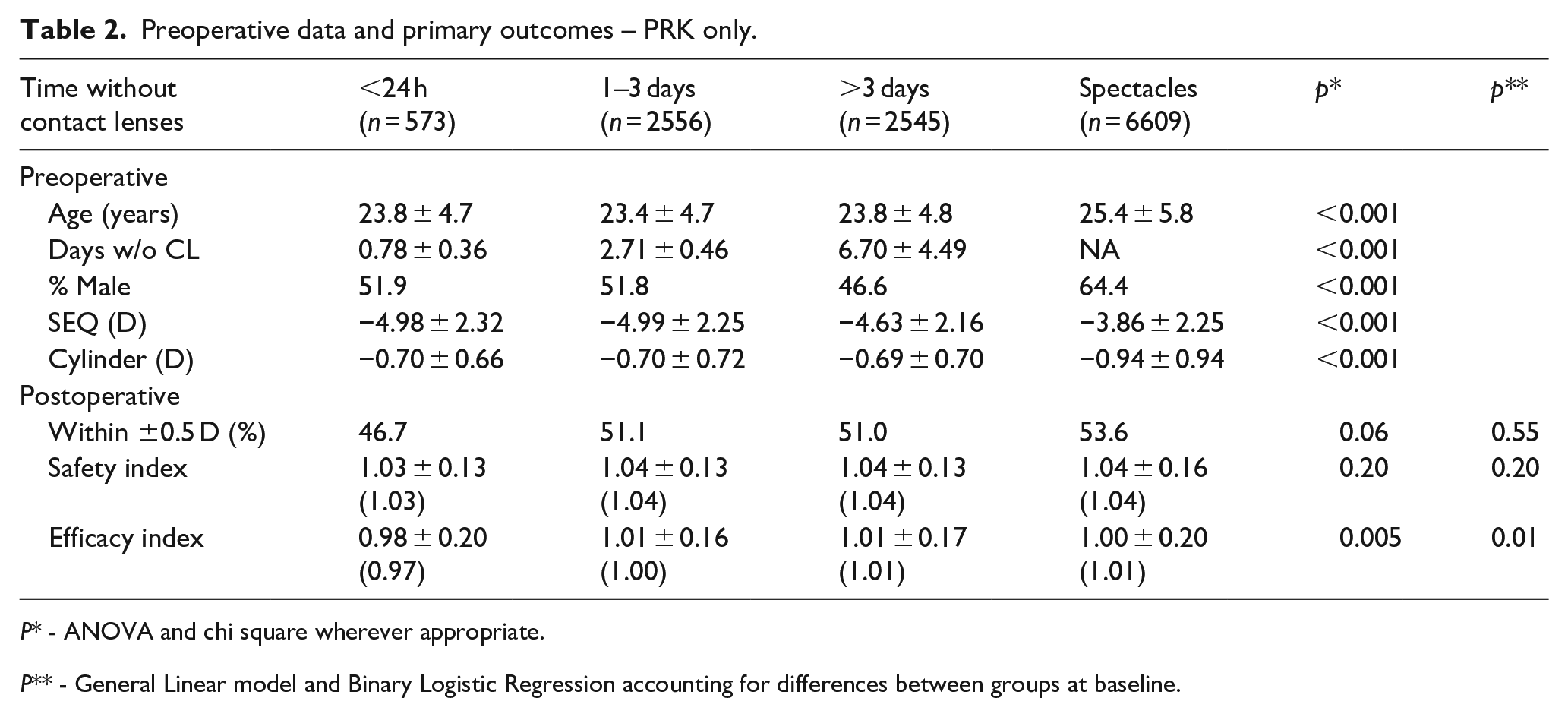
A sub-analysis of the PRK group only is depicted in Table 2. Briefly, in univariate analysis there were no significant differences between groups in terms of safety index (p = 0.20) or % eyes within ±0.5 D (p = 0.06). The <24-h group had a significantly lower efficacy index when compared to all other groups (p = 0.005) and this finding remained significant after adjusting for differences in baseline (p = 0.01).
Preoperative data and primary outcomes – PRK only.
P* - ANOVA and chi square wherever appropriate.
P** - General Linear model and Binary Logistic Regression accounting for differences between groups at baseline.
LASIK only
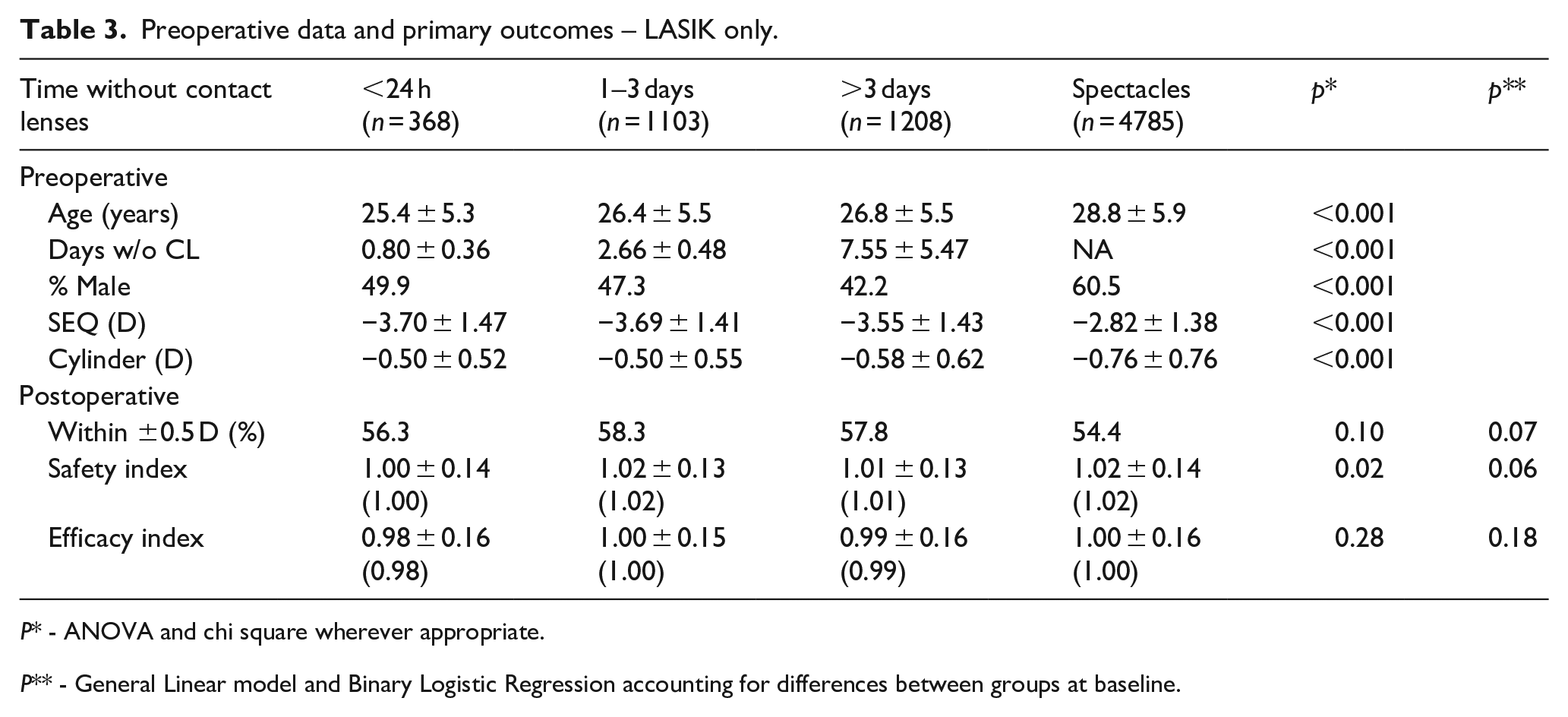
A sub-analysis of the LASIK group only is depicted in Table 3. Briefly, in univariate analysis there were no significant differences between groups in terms of efficacy index (p = 0.28) or % eyes within ±0.5 D (p = 0.10). The <24-h group had a significantly lower safety index when compared to all other groups (p = 0.02), however this no longer remained significant after adjusting for baseline differences (p = 0.06).
Preoperative data and primary outcomes – LASIK only.
P* - ANOVA and chi square wherever appropriate.
P** - General Linear model and Binary Logistic Regression accounting for differences between groups at baseline.
Discussion
In cases where corneal changes induced by CL are present and time period is not sufficient for complete stabilization of these changes, the refractive surgery results might be compromised affecting the efficacy of the procedure. In this study, we found that the visual results after refractive surgery are less favorable when discontinuing SCLs for less than 24 h before final preoperative evaluation and surgery. A sub-analysis revealed that this was true specifically for eyes that underwent PRK. However, we found no advantage for longer discontinuation periods of several days if lenses were discontinued for at least 24 h.
There is a wide variability among refractive surgeons related to the recommended time period to discontinue SCLs before surgery. Most surgeons agree that patients wearing SCLs should discontinue SCLs for at least 3 to 7 days before final refractive assessment and surgery,13–15 however there are no specific guidelines probably due to sparse evidence in the literature. Few studies evaluated the time period needed for the cornea to stabilize after SCLs discontinuation. Budak et al. evaluated corneal stability by computerized videokeratography after contact lenses discontinuation in refractive surgery candidates. They found that discontinuation of SCLs for 2 weeks was adequate for the cornea to return to its baseline topographic features. 17 Shorter periods of discontinuation time or surgical results were not reported in the study.
Ng et al. 10 compared the timeline differences among various methodologies including manifest refraction, pachymetry, keratometry, and corneal topography, in assessing refractive and corneal stability after SCLs wear in keratorefractive candidates. They found that corneal thickness and curvature were the longest to stabilize while manifest refraction was the shortest. The mean time duration-to-stability by manifest refraction was 10.7 days. However, because the first follow up after the initial exam was 7 days for all subjects, one can only interpret that, on average, at most 11 days from initial CL discontinuation are required to reach stability. As such, one cannot conclude, from the aforementioned study, what the shortest discontinuation time recommended before surgery is. 10
Definitive reports on the influence of previous SCL wear and discontinuation periods on refractive surgery outcomes are even fewer. Lloyd-McKernan et al. 18 found that LASIK and LASEK/PRK procedures were even more effective in the SCL group compared with a control group without previous SCLs regardless of the discontinuation time (2 weeks vs 24 h) 1 to 6 months following refractive surgery. However, in the previously mentioned studies, SCL discontinuation less than 24 h was not examined.
In this study, we also found that, the visual results after refractive surgery are not compromised if SCL are discontinued for at least 24 h, but these results are less favorable when discontinuing SCLs for less than 24 h before surgery, specifically for PRK. This could be related to incorrect preoperative refractive measurements caused by the contact lenses wear. In this case, we would not expect a lower safety index; rather we would expect a significant deviation from target refraction that was not found in this study. Our results could be related to lens induced corneal irregularity in those who discontinued the lenses for less than 24 h, leading to higher order aberrations affecting the visual outcomes and leading to lower safety and efficacy indexes in this group.
This study has several limitations. The main ones being the short follow-up time and its retrospective nature. Furthermore, assessment of high order aberrations in the different groups was not assessed. A prospective study, comparing corneal regularity and high order aberrations 24 h after contact lens removal compared to longer discontinuation times could reveal the explanation to our results. In addition, it lacks data on types of SCLs used before surgery. Nevertheless, the findings of this study support routine discontinuation of contact lenses for at least 24 h before keratorefractive surgery final evaluation. In addition, it seems that surgery can be safely performed if the candidate is free of soft contact lenses for 24 h and longer discontinuation time may be redundant.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.