
Abstract
Purpose:
Indocyanine green angiography (ICGA) is a major diagnostic modality but the clinical implications of specific staining patterns in active myopic choroidal neovascularization (mCNV) are unclear. We examined the associations of ICGA cyanofluorescence patterns with disease characteristics and response to an as-needed intravitreal ranibizumab (IVR) treatment regimen among active mCNV patients.
Methods:
Twenty-four subjects with active mCNV treated by IVR were enrolled in this retrospective cohort study. Information from medical records were reviewed, including best corrected visual acuity (BCVA), fluorescein angiography (FA) findings, ICGA cyanofluorescence patterns, and spectral-domain OCT (SD-OCT) results. The CNV lesion size, CNV thickness, and central retinal thickness (CRT) were measured from these images.
Results:
Two staining patterns were identified on late-phase ICGA images, hypercyanescence (9/24, 37.5%) and non-hypercyanescence (15/24, 62.5%). There were no differences in baseline BCVA, CNV thickness, and CRT between ICGA pattern groups; however, the hypercyanescence group demonstrated a larger CNV lesion size (p = 0.035) and required more IVR injections than the non-hypercyanescence group (2.67 ± 1.58 vs 1.07 ± 0.27, p = 0.016), while the non-hypercyanescence group demonstrated better final BCVA improvement (p = 0.041). Hypercyanescence could be divided into two types, a uniform type and rim type. A pseudopodia-like protrusion of CNV enlargement with a rim-enhanced type hypercyanescence at the protrusion rim was predictive of required retreatment.
Conclusions:
Hypercyanescence on late-phase ICGA may assist in identifying more active mCNV requiring intensive treatment.
Keywords
Introduction
Pathologic myopia is one of the three most frequent causes of blindness worldwide, which is particularly common in Asia.1,2 Choroidal neovascularization (CNV) is one of the most common vision-threatening complication of pathologic myopia.3,4 The prognosis of CNV is generally poor without proper treatment. 5 Clinical trials and various preclinical studies have demonstrated that intravitreal anti-vascular endothelial growth factor (VEGF) agents are safe and effective for mCNV treatment, with several trials reporting stable improvement in visual acuity for 2–5 years after diagnosis. A single injection of anti-VEGF agent followed by pro-re-nata (PRN) dosing are generally administered as many mCNV patients require multiple treatments.5,6 Several studies have identified factors predictive of retreatment, including the absence of a dark rim on indocyanine green angiography (ICGA), 7 longer follow-up, larger baseline CNV size, and lower choroidal thickness at baseline.6,8–10
Indocyanine green can provide more information on choroidal vessels in CNV than sodium fluorescein because of its longer wavelength fluorescence and limited diffusion from choriocapillaries. 11 During the choroidal arterial and venous phases, ICGA may detect a focal hypercyanescent area that fades with dye washout. During the late phases, this focal area may remain mildly hypercyanescent in advanced lesions, while in other cases, the intensity at the CNV lesion fades to the intensity of the choroidal background but remains detectable because of a surrounding dark rim. 12 Still other active mCNV cases will show no late-phase hypercyanescence on ICGA.4,13 Therefore, the clinical significance of these specific ICGA patterns is unclear.
We performed this retrospective study to identify clinical characteristics associated with different ICGA patterns in active mCNV, including response to ranibizumab.
Methods
Study design
This retrospective observational comparative study was performed in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Beijing Friendship Hospital (Beijing, China). Informed consent was obtained from all patients after full explanations of the intravitreal ranibizumab injection (IVR) and diagnostic procedures. Ranibizumab (Lucentis) was obtained from Genentech (San Francisco, CA, USA).
Patients
Twenty-four eyes from 24 patients diagnosed with active mCNV at Beijing Friendship Hospital from 1 September 2013 to 30 November 2019, were enrolled. All patients were treated with one IVR injection followed by pro-re-nata (1+prn) treatment. Diagnostic criteria for active mCNV were spherical equivalent refractive error >–6.0 diopters and an axial length >26 mm associated with degenerative fundus changes as revealed by optical coherence tomography (OCT), fluorescein angiography (FA), and indocyanine green angiography (ICGA). Typical active mCNV exhibits a dome-shaped hyper-reflective elevation above the retinal pigment epithelium with subretinal exudation on OCT, a hyperfluorescence from early phase to late phase with significant dye leakage in late phase on FA, and a well-defined CNV on early-phase with or without hypercyanescence on late-phase ICGA images.
Patients were excluded from this study for any one of the following: a history of photodynamic treatment, macular area photocoagulation, intraocular trauma, inflammation, glaucoma, or retinal detachment; severe cataract interfering with OCT, FA and ICGA examination; myopic retinoschisis; maculopathy associated with tractional changes; uncontrolled systemic diseases.
Examination and follow-up
Comprehensive ophthalmic evaluations, including best corrected visual acuity (BCVA), slit-lamp, non-contact intraocular pressure, dilated funduscopic, and spectral domain (SD) OCT examinations, were performed at baseline and during every visit. Refraction and axial length measurements, FA, and ICGA were performed at baseline. Monthly visit was performed for the first 3 months or until CNV stabilization. Follow-up of stabilized CNV was then continued every second month for the next three visits, every third month for the next three visits, and then every 6 months. Monthly visit was reinitiated if recurrent CNV was observed by OCT.
OCT was performed using a Spectralis OCT system (Heidelberg Engineering, Heidelberg, Germany) with the following image acquisition settings: 20°×20°, 49-line, high-speed macular cube, high-resolution scans with a horizontal single line passing through the foveal centralis, and enhanced depth imaging of each horizontal line. Fundus angiography and ICGA were performed using a Heidelberg Retina Angiograph 2 (Heidelberg Engineering, Heidelberg, Germany). Two main ICGA patterns were observed, hypercyanescence during the late phase of ICGA (Figure 1(a)) and non-hypercyanescence (Figure 1(b, c)). Intense dye leakage was considered as hypercyanescence (Figure 1(a)), while hypocyanescence (Figure 1(b)), moderate staining as the intensity of background equivalence (Figure 1(c)) were classified as non-hypercyanescence.
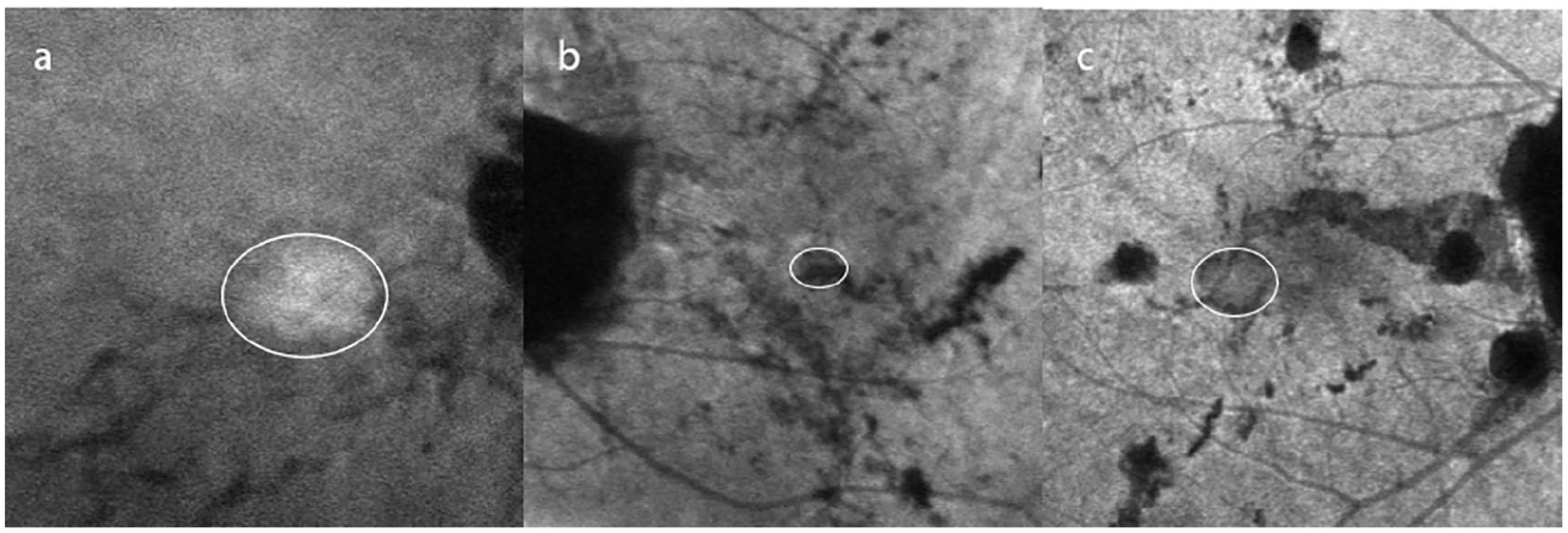
Two distinct late-phase indocyanine green angiography (ICGA) staining patterns (encircled) were observed in eyes with myopic choroidal neovascularization (mCNV) secondary to pathologic myopia, (a) hypercyanescent and (b, c) non-hypercyanescent (either hypocyanescent as in b or mildly hypercyanescent or equivalent to background emission as in c).
Active mCNV lesion size was defined as the largest linear diameter on early-phase ICGA images, CNV thickness as the greatest distance between the hyper-reflective CNV border and retinal pigment epithelium (RPE), and central retinal thickness (CRT) as the distance between the internal limiting membrane and RPE at the fovea. All these parameters were measured manually by two retinal specialists with no knowledge of ICGA pattern classification. The means of the two observer values were used in the final analysis.
Intravitreal injection of ranibizumab
Ranibizumab (0.5 mg/0.05 ml) was injected using a 30-gage needle positioned 4-mm inferotemporal limbus. The injection procedure strictly complied with sterile requirements of intraocular surgery. Active mCNV was diagnosed by agreement of the two authors, who were blinded to patient information. Initial IVR was administered to all active mCNV patients. If CNV activity was resolved according to the next (monthly) follow-up OCT, no further injection was administered unless recurrence was observed by OCT. If CNV activity remained, additional monthly injections were given until CNV stabilization was achieved.
Statistical analysis
The Statistical Package for Social Sciences version 20.0 for Mac (IBM, SPSS Incorporation, Chicago, IL, USA) was used for all statistical analyses. The BCVA was converted to logarithm of minimum angle of resolution (logMAR) values. Continuous variables were compared by paired Student t-test if normally distributed or by Mann–Whitney test if non-parametrically distributed according to the Kolmogorov–Smirnov test, and categorical variables were compared by χ2 tests. A p < 0.05 (two-tailed) was considered significant for all tests. The concordance of ICGA pattern classification between the two retinal specialists was assessed by inter-rater agreement (K) analysis.
Results
Comparison of demographic and baseline clinical data between hypercyanescent and non-hypercyanescent groups
Baseline features of mCNV patients exhibiting the hypercyanescence pattern or the non-hypercyanescence pattern on late-phase ICGA images are summarized in Table 1. A total of 24 eyes from 24 patients of Chinese Han ancestry (4 males and 20 females; mean age 53.83 ± 13.46 years) presenting with active mCNV were analyzed, among which there were 19 cases of subfoveal mCNV and five of juxtafoveal mCNV. The patients were followed-up for 34.26 ± 15.01 months. There were no significant differences in age, sex ratio, spherical equivalent refractive error, BCVA, and mean CRT between the hypercyanescence and non-hypercyanescence groups. Baseline CNV height was greater in the hypercyanescence group but the difference did not reach significance (p = 0.090). However, baseline CNV size was significantly greater in the hypercyanescence group. Of 9 eyes in hyper-group and 15 eyes in non-hyper-group, intraretinal cysts were observed in 55.6% and 53.3%, subretinal fluid in 44.4% and 33.3%, respectively (Figure 2). The agreement between the two retinal specialists in determining the absence or presence of hypercyanescence on late-phase ICGA images was as high as K = 1.0.
Demographic and clinical characteristics of mCNV patients with hypercyanescent (Hyper) or non-hypercyanescent (Non-hyper) late-phase ICGA patterns.
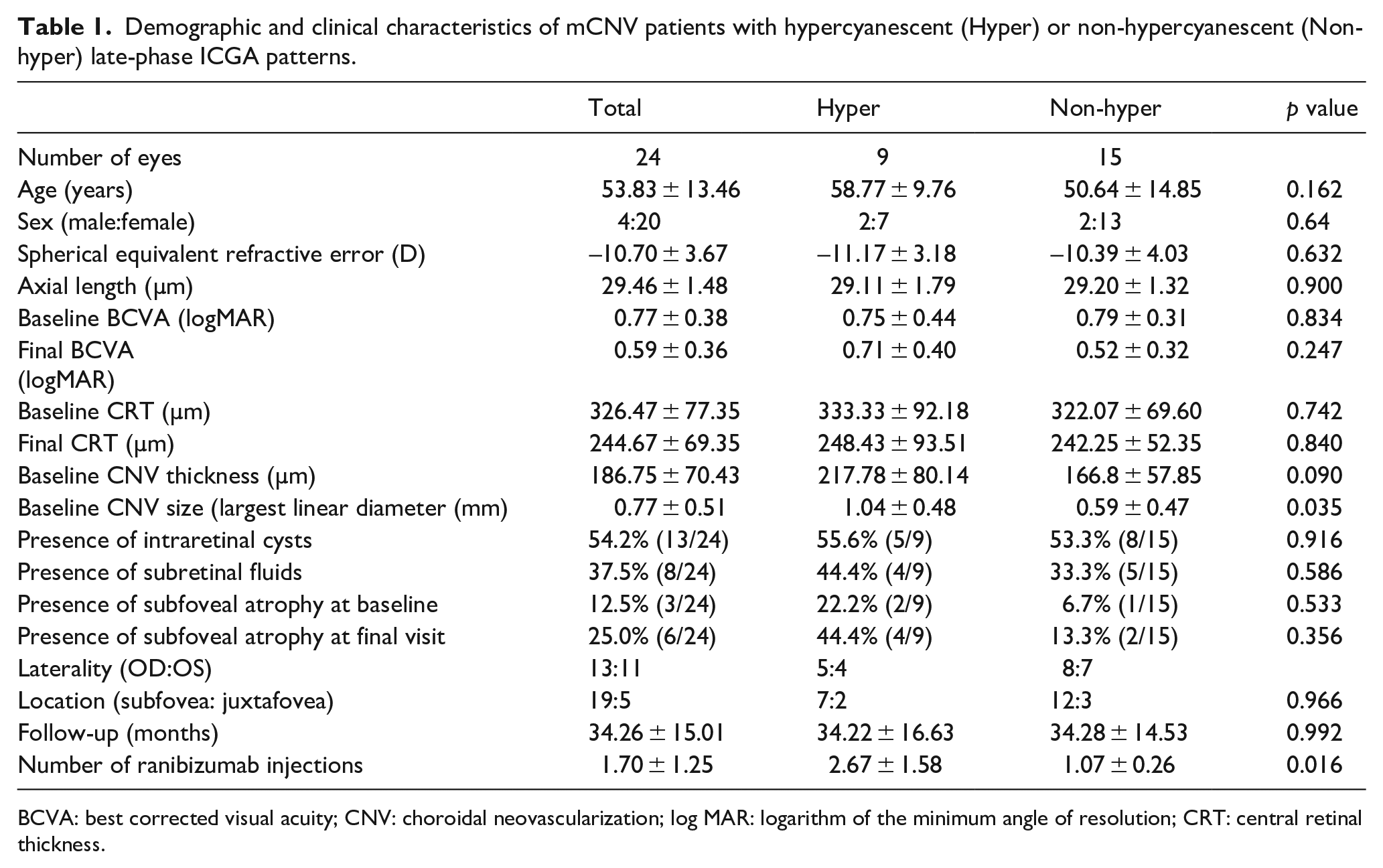
BCVA: best corrected visual acuity; CNV: choroidal neovascularization; log MAR: logarithm of the minimum angle of resolution; CRT: central retinal thickness.
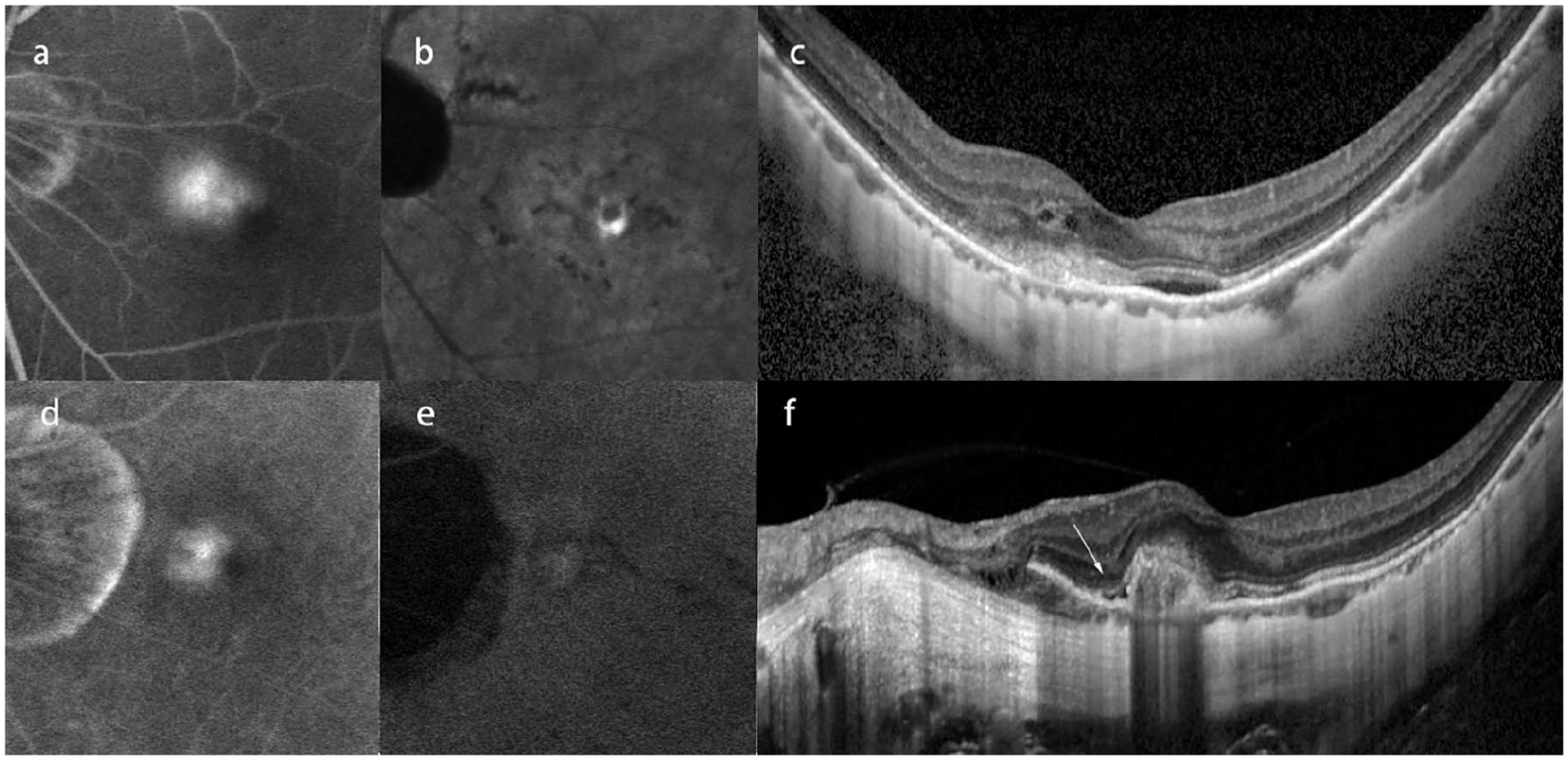
OCT findings in different ICGA patterns of myopic CNV. CNV with profuse leakage in FFA (a) and hypercyanescence in late-phase of ICGA (b). OCT scan showed subretinal hyper-reflective material with fuzzy border, intraretinal cysts and subretinal fluid (c). CNV with profuse leakage in FFA (d) and non-hypercyanescence in late-phase of ICGA (e). OCT scan showed subretinal hyper-reflective material with fuzzy border and subretinal fluid (arrow) (f).
Comparison of visual outcomes
Visual outcomes are also summarized in Table 1. Final BCVA was significantly improved in the non-hypercyanescence group compared to baseline (p = 0.041) but not in the hypercyanescence group (p = 0.817).
Retreatment
Of the 24 eyes, 15 demonstrated complete resolution of CNV activity after only one injection (62.5%), the majority of which were in the non-hypercyanescence group (86.7% vs 22.2%). Moreover, hypercyanescent eyes required a significantly greater number of ranibizumab injections for clinical stability (2.67 ± 1.58 vs 1.07 ± 0.27, p = 0.016).
Locations of mCNV
Fifteen eyes exhibited lacquer cracks on ICGA (62.5%) with higher incidence in the hypercyanescence group (77.8% vs 46.7%). Among these, only five cases of lacquer cracks were also observed on FA (20.83%), again with higher incidence in the hypercyanescence group (44.44% vs 6.7%). The CNV area was located at the tip of these lacquer cracks (Figure 3(a)) or at the center (Figure 3(b)).
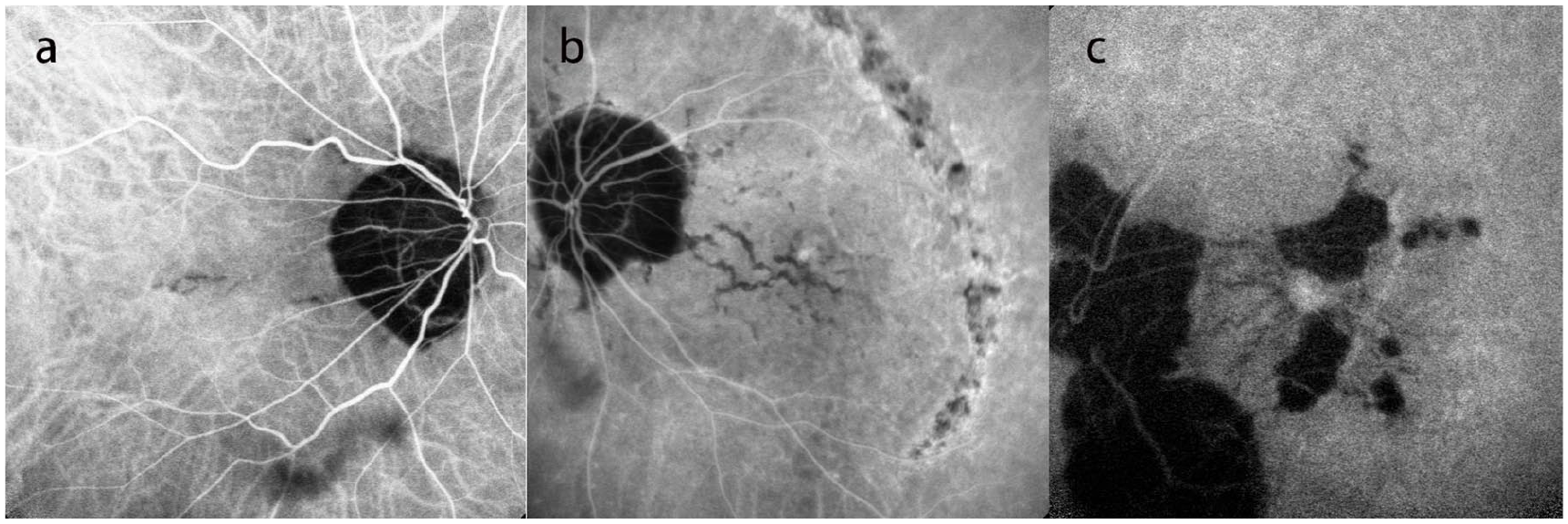
Locations of mCNV lesions. Myopic CNV lesions were located either on the tips of lacquer cracks (a) or at the center of lacquer cracks (b). (c) In some cases, mCNV lesions were located in the center of lacquer cracks within the perfused chorocapillary area at the border of atrophy regions, and radical-pattern lacquer cracks were centered on the macular fovea.
Ten eyes also exhibited choroidoretinal atrophy, four in the hypercyanescence group (26.7%) and six in the non-hypercyanescence group (66.7%), of which five involved macular area. Among these eyes with choroidoretinal atrophy, CNV extended into the perfused choriocapillary area at the border of the atrophic region (Figure 3(c)). All eyes exhibited lacquer cracks or choroidoretinal atrophy, and one exhibited both lacquer cracks and choroidoretinal atrophy.
CNV progression
Of the nine eyes requiring retreatment (37.5%), the majority were in the hypercyanescent group (seven eyes or 77.8% vs two eyes or 13.3%). In one subject, both occurrence and progression of CNV were observed. Four months before active mCNV onset, a hypercyanescence spot was detected by ICGA in the middle of a horizontally oriented linear lacquer crack, but with no evidence of fluorescein leakage on FA (Figure 4(a)). Diffuse fluorescein leakage and a CNV lesion (hyperfluorescence) appeared upon active mCNV onset (Figure 4(b)). Nine months after single IVR injection, a larger scale hypercyanescent CNV lesion appeared at the primary lesion site in the middle of a larger lacquer crack (Figure 4(c’)). Three months after a second injection of IVR, an enlarged CNV lesion reemerged with a pseudopodia-like protrusion at the inferior temporal margin (Figure 4(d’)). The main part of the CNV region had a cyanescence intensity similar to background, while the protrusion showed intense hypercyanescence, especially at the rim of the CNV protrusion (Figure 4(d”)).
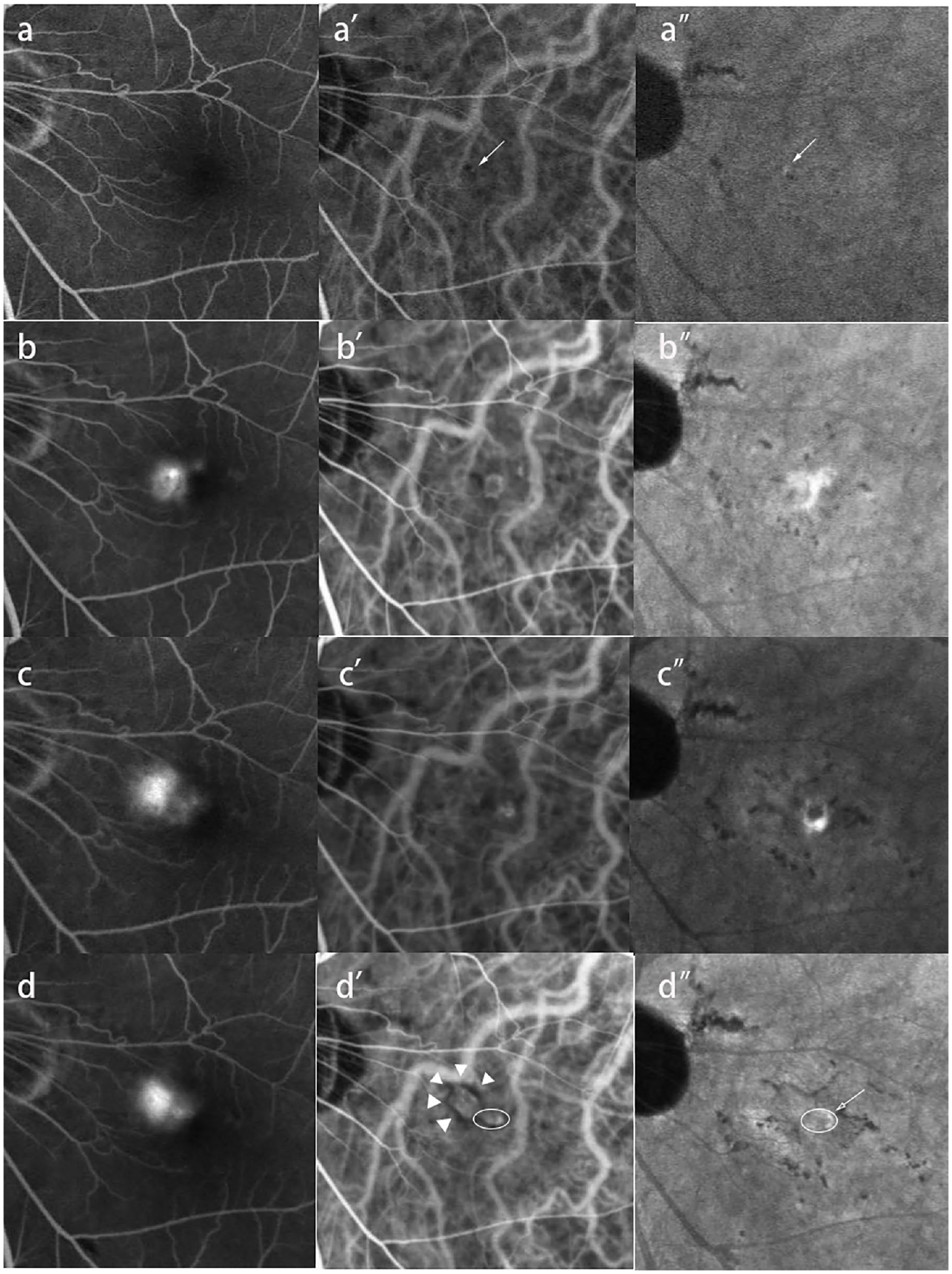
Progression of mCNV. (a, a’, a”) Four months before active CNV onset. No obvious fluorescence leakage, fluorescein staining, or window defect was observed on fluorescein fluorescence angiography (FFA). A hypercyanescent spot (arrow) in the middle of a short lacquer crack was observed 5 minutes post-injection on ICGA (a’), which was maintained throughout the late phase of ICGA (a”). (b, b’, b”). Active mCNV. Diffuse fluorescein leakage was observed on FFA (b), and a subfoveal CNV lesion appeared on a 5-minute ICGA image (b’) that progressively increased in cyanescence intensity with time (b”), especially at the inferior temporal rim of the CNV lesion (arrow). In addition, lacquer cracks were more numerous and longer compared to before onset. No dark rim was observed around the CNV lesion. (c, c’, c”) First active mCNV recurrence 9 months after the first (loading) IVR injection. Diffuse fluorescein leakage was observed again on FFA images (c). A subfoveal CNV lesion at the same location as the first occurrence appeared on the 5-minute ICGA image (c’) and a progressively intense hypercyanescent lesion was observed by ICGA (c”). This hypercyanescent region was more intense at the inferior temporal rim of the CNV lesion. Compared to the first occurrence, lacquer cracks were longer and the CNV lesion moderately larger. No obvious dark rim was observed around the CNV lesion. (d, d’, d”) Second active CNV recurrence. Two months after the second single IVR injection, diffuse fluorescein leakage was observed on FFA (d). A larger subfoveal CNV lesion appeared at the first occurrence site on the 5-minute ICGA image (d’), and a pseudopodia-like protrusion was observed at the inferior temporal margin (d”, circled by the oval). A dark rim was observed around the main part of the original CNV lesion (d’, arrow head), whereas no dark rim was observed around the newly arising protrusion. Intense cyanescence was observed at the margin of the protrusion (d”, arrow); however, the cyanescence intensity at the main CNV lesion site was similar to the background emission.
Hypercyanescence types
In the hypercyanescence group, two distinct patterns of hypercyanescence were observed, a uniform type (seven of nine subjects, 77.8%) and a rim-enhanced type (two of nine subjects, 22.2%). In the uniform type, the CNV lesion showed relatively uniform hypercyanescence intensity on late-phase ICGA images (Figure 5(a)), while in the rim-enhanced type, the periphery of the CNV lesion exhibited much more intense cyanescence than the main CNV area (Figure 5(b)).
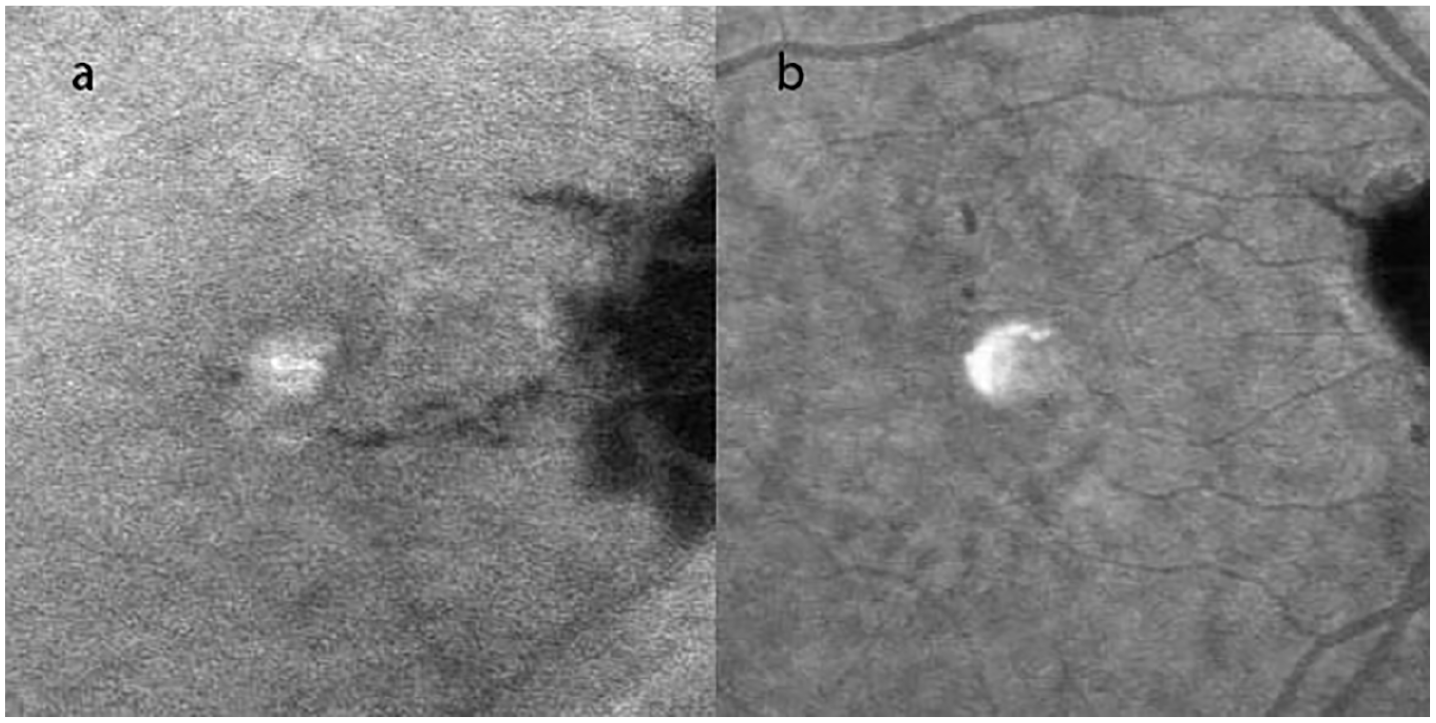
Two distinct hypercyanescence patterns on ICGA, uniform type (a) and rim-enhanced (b). In the uniform type, late-phase ICGA images showed lesions with uniform hypercyanescence. In the rim-enhanced type, the superior temporal rim of the CNV lesion showed a greater cyanescence intensity than the main lesion.
Intravitreal injection complications
No systemic intravitreal Ranibizumab-related complications were observed in any patients. Mild subconjunctival hemorrhage at injection location was found once in two seperate patients. No severe ocular complications, including intraocular inflammation, endophthalmitis, glaucoma, cataract, or retinal detachment, was observed during follow-up period. Two eyes in hyper-group and one eye in non-hyper-group showed a novel subfoveal macular atrophy (Figure 6).
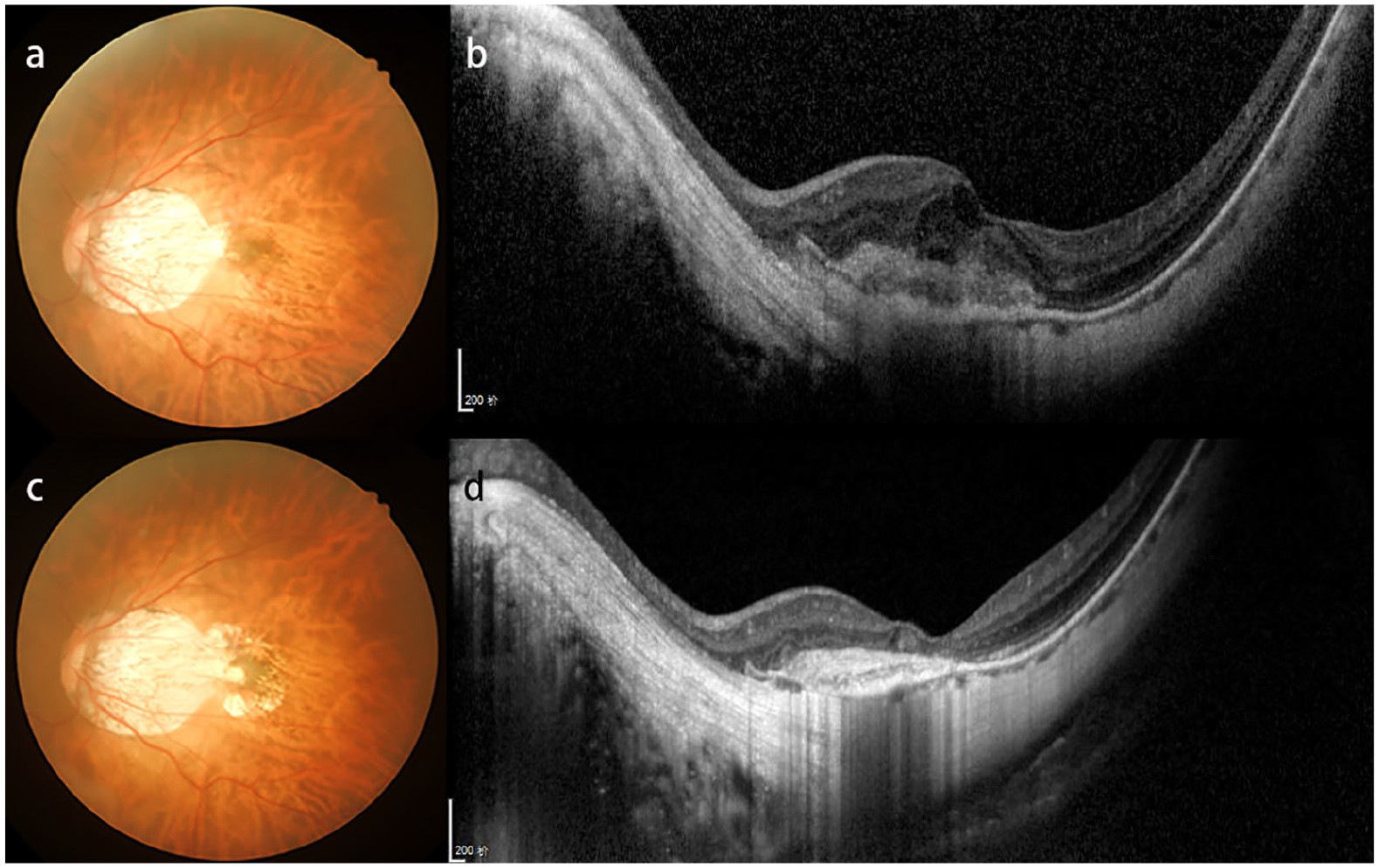
A 53-year-old woman in hyper-group complaint of metamorphopsia with visual loss in her left eye. Fundus examination revealed a myopic conus extended to parafoveal area, and subtle subfoveal grayish lesion with no hemorrhage noticed (a). The baseline SD-OCT scan showed subretinal hyper-reflective material with fuzzy border and intraretinal cyst (b). The final visit fundus examination 26 months later revealed a grayish membrane with macular atrophy (c). An SD-OCT scan showed a reduced subretinal hyper-reflective material without fuzzy border, intraretinal cysts or subretinal fluids (d).
Discussion
Indocyanine green angiography is an important modality for the differential diagnosis of mCNV,14,15 as it can reveal well-defined neovascularization and lacquer cracks around the lesion.16,17 However, FA is generally considered the gold standard because not all mCNV cases exhibit hypercyanescence.4,13,18 In this study, we retrospectively divided 24 active mCNV eyes into two groups according to the appearance of hypercyanescence on late-phase ICGA images, and we examined differences in ranibizumab treatment response and various clinicodemographic characteristics to assess the clinical significance of these ICGA patterns. Baseline CNV area was significantly larger in the hypercyanescence group, indicating greater disease activity. Further, the hypercyanescence group required more IVR injections to reach stability, in accord with previous studies reporting that CNV size predicts the need for additional treatments to control subfoveal mCNV.6,8,9,19
In our study, the two groups had no statistically significant difference in the percentage of patients with intraretinal cysts or subretinal fluids on SD-OCT (Table 1). The possible reason is that all mCNV enrolled in our study was active with a profuse leakage in FFA (Figure 6). And our results are similar to previous studies about morphologic features of OCT in association with fluorescein angiography.8,20,21 These SD-OCT features related to the exudative manifestations do not help recognize the CNV subtype. 8 Relationship between OCT features in association with ICGA would be evaluated in further studies, and assessment of ICGA dye leakage at baseline may provide a precise characterization of mCNV with clinical relevance.
As in previous studies,12,18 only a subgroup of patients exhibited hypercyanescence, while one study found no hypercyanescence on ICGAimages. 13 Degenerative myopia is associated with severe circulatory disturbances as evidence by delayed blood flow in the choroidal vessels and diffusely thinned choriocapillaries with less choroidal stroma and obliteration of choroidal vessels. 22 Thus, the absence of hypercyanescence in mCNV may be caused by low choriocapillaris perfusion. Choroidal thinning is believed to be involved in mCNV pathogenesis, and baseline choroidal thinning was associated with recurrence and incomplete resolution after anti-VEGF treatment.9,10 A subsequent study found that choroidal thickness increase after anti-VEGF treatment was associated with recurrence. 23 Moreover, mCNV growth was more common in eyes with less advanced staphyloma. Therefore, a preserved choriocapillaris is theoretically required for mCNV to develop. 13 Alternatively, relatively affluent choriocapillaris perfusion may explain the appearance of hypercyanescence in some patients with larger lesion size. Myopic CNV frequently extended into the perfused choriocapillaris area rather than into the region of atrophy (Figure 3(c)), similar to retinal neovascularization arising from a choriocapillaris perfusion area adjacent to a nonperfusion area in retinal vascular diseases. Based on these findings, we speculated that hemodynamic changes may be a cardinal mechanism for mCNV growth.
Hypercyanescence on late-phase ICGA images was classified into two types, uniform and rim-enhance type (Figure 5(a) and (b)). Only two subjects showed the rim-enhance type, both in the hypercyanescence group. One of these subjects demonstrated complete resolution of CNV activity after a single IVR injection, and this case remained stable for 51 months (Figure 5(b)), while the other one has recurred twice since diagnosis. At initial CNV onset, an inferior temporal rim-enhancement type hypercyanescence was observed by ICGA (Figure 4(b’) and (b”)) that persisted for two recurrences. On the second recurrence after single IVR injection, an enlarged CNV appeared at the first occurrence site with a pseudopodia-like protrusion at the inferior temporal margin (Figure 4(d’) and (d”)), and a dark rim was seen around the main CNV site arising from the original lesion. However, no dark rim was observed around the new protrusion. Intense hypercyanescence was observed at the margin of the protrusion, whereas the cyanescence intensity of the main lesion was similar to the background emission (Figure 4(d”)).
Choroidal neovascularization was once considered a nonspecific wound repair response to specific stimuli based on observations of surgically excised and postmortem tissue. 24 However, new imaging modalities have revealed CNV growth as a dynamic process that can be divided into three stages, initiation, active growth, and involutional. The initiation stage is considered an active inflammation phase driven by large amounts of inflammatory cytokines involved in angiogenesis and vasculogenesis. 25 This inflammation causes hypercyanescence in ICGA. Therefore, the intense hypercyanescent rim may be the active growth area or the head of CNV extension initiated by inflammation, and the CNV growth type may be divided into cases enlarging evenly and those with lateral extension. From the active CNV growth stage onward, fibrinogenesis leading to a fibrin scaffold for CNV growth progressively develops to collagenization of CNV. 25 During the active CNV growth stage, RPE cells produce transforming growth factor beta (TGFβ), which appears to limit the extent of the CNV, 26 presumably at the margins, followed by CNV stabilization. During the involutional stage, hyperplasia and migration of RPE cells and macrophages to CNV tissue have been observed in histopathological studies. Multilayered proliferating RPE cells surrounding the CNV may manifest as a dark rim on ICGA. Kim et al. suggested that the dark rim may have strong regenerative potential 27 ; moreover, we speculate that the dark rim represents active CNV growth but tending toward stability, as it surrounds a mildly hypercyanescent main CNV region with only background cyanescence intensity (Figure 4(d”)).
Intravitreal anti-angiogenesis therapy targeting VEGF, a key initiator of angiogenesis and a principal cause of vascular leakage, 28 is now the first-line treatment for mCNV with proven efficacy for visual improvement. With treatment, regression of the most recently formed vascular elements is possible, but more established vessels generally do not regress. Multivariate analysis showed that BCVA was correlated with central retinal thickness and vessel density; thus, cases with CNV lesions of greater vascularity achieved better visual acuity. 29
In international classification of myopic maculopathy proposed by Ohno-Matsui et al., myopic maculopathy was classified into five different categories based on atrophic changes. 30 And CNV was described as a “plus” lesions coexisted across the categories. Macular atrophy (category 4) is associated with a progressive decrease in BCVA, which is considered either as the primary consequence of myopic choroidopathy or as an outcome of neovascularization. 13 In hyper-group in our study, there was two patients (22.2%) with macular atrophy at baseline, which number was increased to four (44.4%) at final visit. In non-hyper-group, the number was 6.7% and 13.3% separately at baseline and final visit. The increase of percentage of macular atrophy in hyper-group may be an outcome of recurrence of CNV, which may be the reason of impediment BCVA improvement at final visit in hyper-group as well.
In our study, patients required a mean number of 1.70 ± 1.25 injections, with a significantly greater number required for patients with hypercyanescence (2.67 ± 1.58 vs 1.07 ± 0.27 in the non-hypercyanescence group). In the RADIANCE study, the anti-VEGF treatment required a mean of two ranibizumab injections by month 12 post-onset, 31 while in the BRILLIANCE study, patients required nearly double this number (mean of 4.6 and median of 4.0 in Group I, 3.9 and 3.0 in Group II). 32 In the post-RADIANCE study, acceptable VA was generally retained over the 4-year follow-up period with an average of 5.0 ± 5.94 injections. 33 Based on these data, prompt treatment with one loading intravitreal anti-VEGF dose followed by PRN dosing is recommended.
Our study has some limitations. First, three subjects received anti-VEGF injections before enrollment, one in the non-hypercyanescence group and two in the hypercyanescence group, so baseline FA and ICGA imaging features may be different from treatment-naïve subjects. The retreatment criterion adopted was new onset visual impairment attributable to intraretinal or subretinal fluid or active leakage secondary to myopic CNV; therefore, not all FA or ICGA images during follow-up were recorded before IVR. Finally, the non-associations among certain factors such as recurrence of CNV, BCVA improvement, and number of injections may result from the small sample size.
In conclusion, our study identified two distinct late-phase ICGA manifestations of mCNV, hypercyanescent and non-hypercyanescent. In the hypercyanescent group, CNV was characterized by larger lesions and a requirement for additional intravitreal ranibizumab injections. Hypercyanescence on late-phase ICGA images be a specific feature of active mCNV. Therefore, this imaging sign provides information on disease severity and prognosis.
Supplemental Material
supplementary_material-figures_detail – Supplemental material for Late-phase hypercyanescence during indocyanine green angiography for assessment of myopic choroidal neovascularization
Supplemental material, supplementary_material-figures_detail for Late-phase hypercyanescence during indocyanine green angiography for assessment of myopic choroidal neovascularization by Taoran Zhang, Wei Wang, Mingming Li and Yingxiang Huang in European Journal of Ophthalmology
Footnotes
Acknowledgements
The authors thank Fan Zhang, Hui Miao, Xiumei Ma for their expert assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the High-level Technical Personnel Training Program of Municipal Health System, CHINA (No. 2014-3-007).
Supplemental material
Supplemental material for details of figures in this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.