
Abstract
Purpose:
To assess the morphological and functional outcome of oral eplerenone for treatment of patients with chronic central serous chorioretinopathy (CSC) in a real life experience.
Patients and methods:
In this retrospective study, we reviewed the clinical files of 30 patients with chronic CSC. All patients were treated with eplerenone for a period of 6 weeks or 3 months depending on the clinical response. Main outcome measures included: best corrected visual acuity (BCVA), central macular thickness (CMT) and height of the subretinal fluid (SRF). Comparisons between responders and non-responders were performed to identify factors that were predictive of the treatment response.
Results:
All patients were treated with eplerenone 18 ± 20 weeks after onset of the first symptoms. BCVA (LogMAR) improved from 0.2 ± 0.2 to 0.13 ± 0.18 at 6 weeks (p = 0.01) and to 0.09 ± 0.15 at 3 months (p = 0.01). Mean CMT decreased from 409 ± 136 to 323 ± 87 µm at 6 weeks (p = 0.001) and to 298 ± 98 µm at 3 months (p = 0.01). Mean height of SRF decreased from 153 ± 126 to 73 ± 79 µm at 6 weeks (p = 0.001) and to 49 ± 88 µm at 3 months (p = 0.005). Complete resolution of SRF was achieved in 20 patients after 3 months (67%). Reported stress in the medical history was the only statistical significant predictive factor associated with a positive treatment response.
Conclusion:
This study showed a statistically significant improvement of the best corrected visual acuity and a significant reduction of macular thickness and subretinal fluid in patients with chronic CSC treated with oral eplerenone, especially in patients under stress.
Keywords
Introduction
Central serous chorioretinopathy (CSC) is a chorioretinal disorder characterised by a serous detachment of the neurosensory retina, frequently involving the macula. CSC has an incidence of 1/10.000 in the Caucasian population and is supposed to be the fourth most common nonsurgical retinopathy after age-related macular degeneration, diabetic retinopathy and branch retinal vein occlusion. CSC typically affects young male patients during the third or fourth decade of life, with a peak around 40 to 45 years. It is more rarely seen in women, presenting male-to-female ratios of up to 6:1.1–3
CSC can occur in an acute or chronic form. Up to 30% to 50% of cases of acute CSC develop into a chronic form with retinal pigment epithelium (RPE) defects associated with variable photoreceptor degeneration. Secondary choroidal neovascularisation (CNV) can develop in some cases.1,3
CSC usually occurs unilaterally. However, bilateral cases have been described in older patients. Typical symptoms include metamorphopsia, micropsia, mild dyschromatopsia and reduced contrast sensitivity.1,3 The exact pathogenesis remains unclear despite advances in imaging techniques and numerous studies of the disease. Hyperpermeability of the choroidal vessels with a consecutive alteration of the RPE seem to play a key role for the subretinal fluid accumulation with resulting detachment of the neurosensory retina. The continual development in choroidal imaging has led to a better understanding of many chorioretinal disorders as well as a new spectrum of pachychoroid-related macular disorders. The term ‘pachychoroid’ is defined as an abnormal and permanent increase in choroidal thickness, which is typical in CSC, particularly when involving the Haller’s layer.2–5
A clear association between CSC and increased levels of endogenous and particularly exogenous corticosteroids has been shown in several studies.6,7 Corticosteroids seem to alter the permeability of the RPE, Bruch’s membrane and choriocapillaris and have been proven to be a clear risk factor for developing CSC. 8 Stress, pregnancy, alcohol consumption, autoimmune diseases, untreated hypertension, gastroesophageal reflux, use of psychopharmacologic medications and infections with Helicobacter pylori have been identified as further risk factors.8,9
According to the literature, the spontaneous remission of SRF in acute cases is up to 68% within 4 months and 84% within 6 months after the initial diagnosis. 1 Therefore, according to the recommendations of the DOG (Deutschen Ophthalmologischen Gesellschaft) and BVA (Berufsverband der Augenärzte Deutschlands) no therapy should be given within the first 4 months in acute cases of CSC. On the other hand, if the SRF persist longer than 4 months, without any sign of spontaneous regression, the DOG and BVA recommend to start a treatment with a mineralocorticoid-receptor antagonists, such as eplerenone. 1 So far, there is no clear consensus for the treatment and management of chronic CSC, but several treatments have been proposed, such as mineralocorticoid-receptor antagonists, half-dose PDT-Laser or Nanosecond Laser.10,11 Eplerenone is a highly selective aldosterone-receptor antagonist and potassium-sparing diuretic developed in 2003 in the United States. It possesses a higher selectivity and affinity compared to spironolactone and, therefore, fewer side effects. It has shown promising results in the treatment of patient with chronic CSC.12,13
The purpose of this study was to assess the morphological and functional outcome of oral eplerenone for treatment of patients with chronic central serous chorioretinopathy.
Patients and methods
Design
This retrospective single-centre study was conducted at the Department of Ophthalmology, Saarland University Medical Center in Homburg/Saar (UKS), Germany.
Patients
In this study, we reviewed the clinical files of 30 patients with chronic CSC. All patients showed clear retinal pigment epithelial (RPE) defects in the optical coherence tomography (OCT) (Heidelberg Spectralis, Heidelberg, Germany), the fundus autofluorescence (FAF) images and the ophthalmoscopy and were, thus, diagnosed with a chronic form of CSC. Exclusion criteria were the presence of any other retinal disease, including age-related macular degeneration, diabetic retinopathy, retinal vessel occlusion, high myopia and history of CSC treatment, including laser, PDT and anti–VEGF therapy.
Study protocol
Patient medical records and imaging data were reviewed at baseline, 6 weeks and 3 months, including best corrected visual acuity (BCVA), spectral-domain OCT, dilated fundus biomicroscopy and fundus autofluorescence.
Main outcome measures included: best corrected visual acuity (BCVA) converted into logMAR scale, central macular thickness (CMT) and height of the subretinal fluid (SRF). We also reviewed the proportion of eyes achieving complete resolution of SRF.
The response to treatment was defined by a decrease of more than 50% in SRF height after start of the treatment. 14 Comparisons between responder and non-responder groups were made to identify factors that might be predictive of the treatment response.
Treatment protocol
All 30 patients were treated with eplerenone orally 25 mg daily for 1 week, then 50 mg daily for a period of 6 weeks or 3 months depending on the clinical response. The off-label prescription and the potential benefits and risks of the treatment were discussed with all patients and an informed consent was obtained. All medical contraindications were excluded before treatment. All patients underwent a potassium serum level control every 2 weeks to exclude a hyperkalaemia (>5.5 mmol/l), which could cause cardiac arrhythmias.
Statistical analysis
Comparisons between variables at baseline, 6 weeks, and 3 months were performed using the Wilcoxon paired, Mann-Whitney U or chi-square tests as appropriate. Data were presented as mean ± standard deviation. Results were considered statistically significant if p-values were ⩽0.05.
Data were analysed using SPSS 20.0 for windows (SPSS, Inc., Chicago, IL).
Results
All patients were diagnosed with chronic CSC and were treated with eplerenone 18 ± 20 weeks after onset of the first symptoms of the CSC. Mean age of patients was 52.6 ± 6.4 years; 36% were female. BCVA (LogMAR) improved from 0.2 ± 0.2 to 0.13 ± 0.18 at 6 weeks (p = 0.01) and to 0.09 ± 0.15 at 3 months (p = 0.01) (Figure 1).
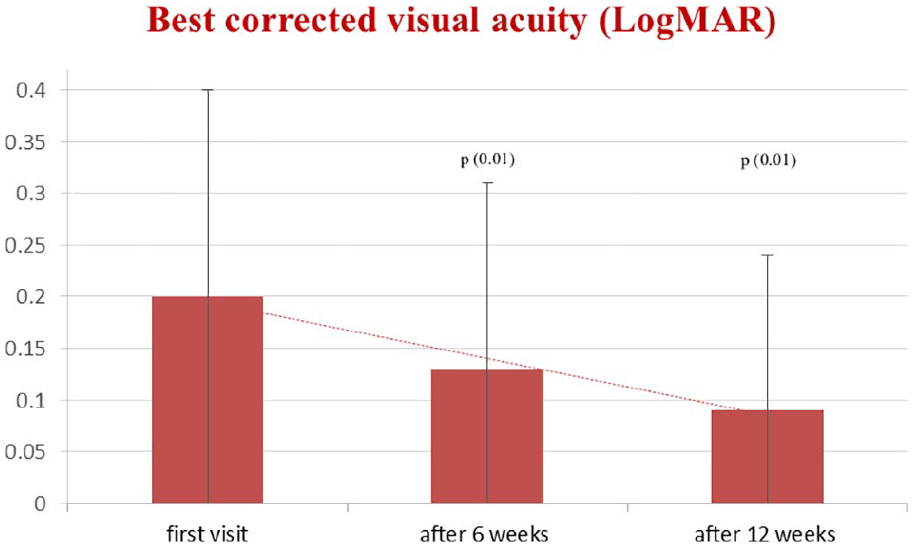
Best corrected visual acuity (BCVA) after 6 and 12 weeks of treatment. Results are given as means ± standard deviation; p-value refers to statistical differences between baseline values, values after 6 and 12 weeks of treatment.
Mean CMT decreased from 409 ± 136 to 323 ± 87 µm at 6 weeks (p = 0.001) and to 298 ± 98 µm at 3 months (p = 0.01) (Figure 2).
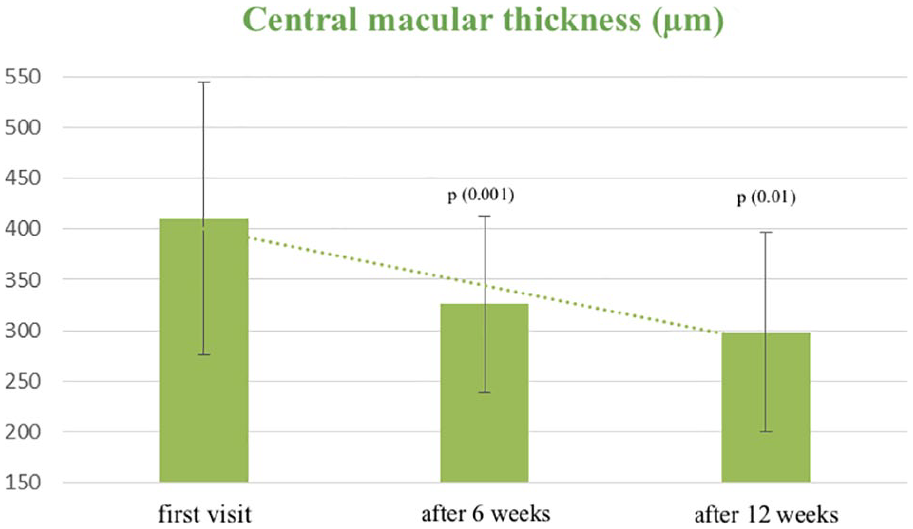
Central macular thickness (CMT) after 6 and 12 weeks of treatment. Results are given as means ± standard deviation; p-value refers to statistical differences between baseline values, values after 6 and 12 weeks of treatment.
Mean height of SRF decreased from 153 ± 126 to 73 ± 79 µm at 6 weeks (p = 0.001) and to 49 ± 88 µm at 3 months (p = 0.005) (Figure 3).
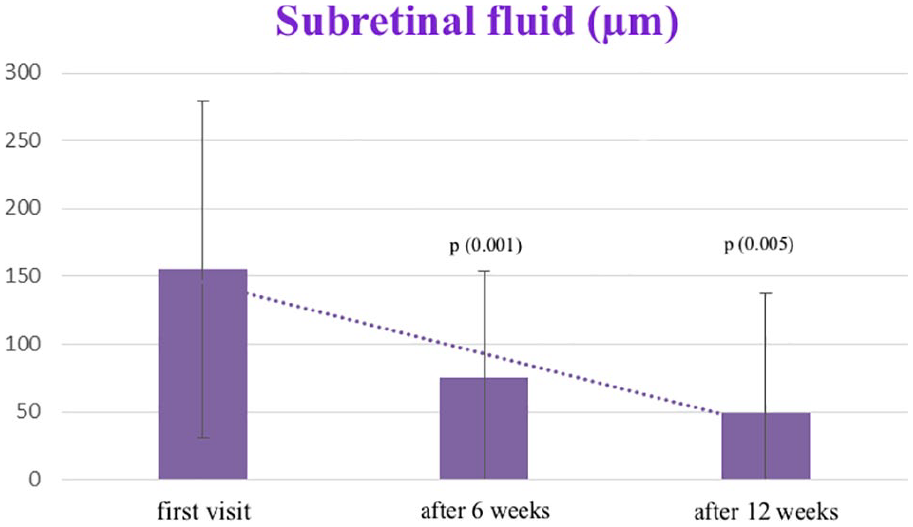
Subretinal fluid (SRF) after 6 and 12 weeks of treatment. Results are given as means ± standard deviation; p-value refers to statistical differences between baseline values, values after 6 and 12 weeks of treatment.
Differences between 6 and 12 weeks were not significant for all parameters (BCVA: p = 0.39; Mean CMT: p = 0.31; Mean Height of SRF: p = 0.29).
The improvement of BCVA (decimal as supplementary data) was 0.15 ± 0.28 after 6 weeks and 0.20 ± 0.23 after 12 weeks. The reduction of SRF height was 0.79 ± 134 µm after 6 weeks and 135 ± 170 µm after 12 weeks. The reduction of CMT was 86 ± 136 µm after 6 weeks and 129 ± 168 µm after 12 weeks (Table 1).
Improvement of best corrected visual acuity (BCVA), reduction of subretinal fluid (SRF) height and central macular thickness (CMT) after 6 and 12 weeks of treatment.

Complete resolution of the SRF was achieved in six patients after 6 weeks (20%) and an additional 14 patients after 3 months (47%), making a total of 67% at 3 months.
One patient was excluded due to high potassium blood levels. Three patients were treated with micropulse (Nanosecond) laser after 3 months and three patients developed secondary choroidal neovascularisation and were treated with vascular endothelial growth factor inhibitors.
Based on the response, patients were divided into two study groups: a responder group and non-responder group. Patients without SRF or with a decrease of more than 50% in SRF height after 12 weeks were considered responders. Patients with a decrease of less than 50% in SRF height after 12 weeks were considered non-responders. Comparisons between responder and non-responder group were performed to identify factors that were predictive of the treatment response. There were no statistical significant differences in age, sex ratio, BCVA at baseline, SRF height at baseline and rate of secondary CNV. Reported stress in the clinical history was the only statistically significant factor (p = 0.01) associated with a better treatment response. 40% of the patients in the response group reported having stress (Table 2).
Comparison between the responder group and non-responder group treated with epleronone with chronic CSC. Results are given as means ± standard deviation; p-value refers to statistical differences between responder and non-responder groups.
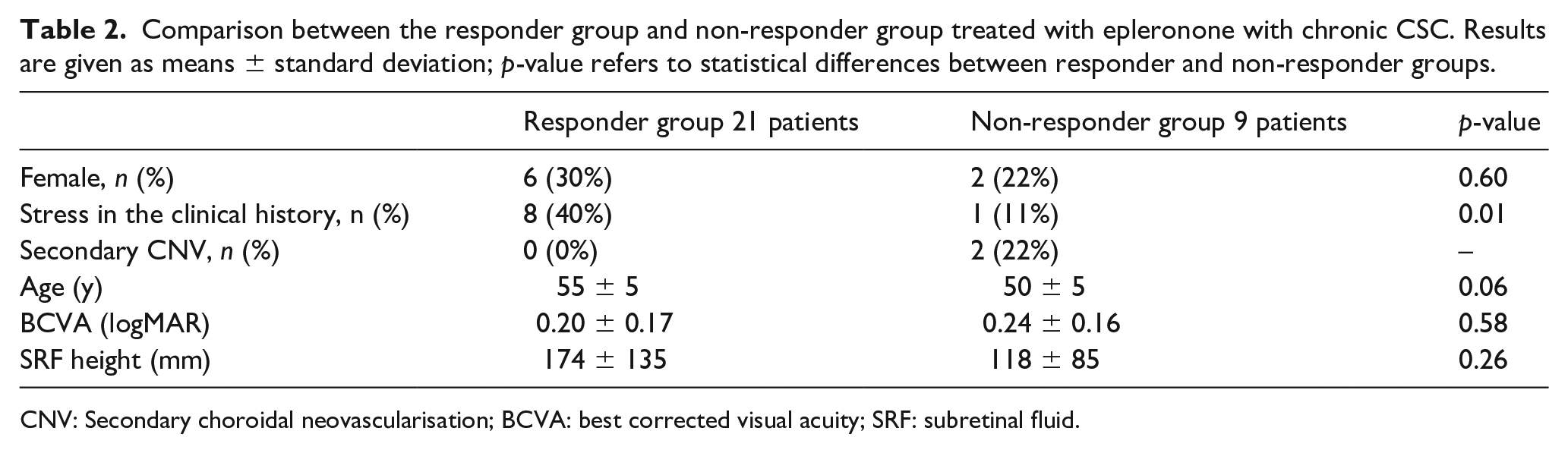
CNV: Secondary choroidal neovascularisation; BCVA: best corrected visual acuity; SRF: subretinal fluid.
Fifteen patients (71.4%) of the responder group had no recurrence during the follow-up period of 1 year. One patient had a recurrence after 4 months of treatment, one after 6 months and one after 8 months of treatment. Four patients had a recurrence during the second year of the follow-up period.
Discussion
Two forms of central serous chorioretinopathy (CSC) are currently distinguished: an acute or chronic form. These two forms differ in symptom duration and integrity of the retinal pigment epithelium (RPE). The acute form typically presents subretinal fluid (SRF) with one or multiple circumscribed RPE detachments without any associated RPE defects. Up to 30% to 50% of cases of acute CSC recurs and may transform into a chronic form.1–3 The chronic form, initially called ‘diffuse retinal epitheliopathy’, was described as a variant of CSC and acquires RPE defects associated with variable photoreceptor degeneration responsible for permanent functional impairments.
Fundus autofluorescence (FAF) images should be used to determine the presence and severity of these RPE lesions and provide information as to whether the disease has already taken a chronic course.1,4,5 In the present study we selected patients with chronic CSC showing clear RPE lesions in the OCT, FAF images and ophthalmoscopy.
In 2012 Zhao et al. identified mineralocorticoid receptor (MR) activation as a potential pathological pathway underlying the vascular choroidopathy observed in CSC.15,16 The first publication on the therapeutic principle ‘Mineralocorticoid-receptor antagonists as treatment option for acute and chronic central serous chorioretinopathy’ was published in 2014 by Maier et al. discussing the use of spironolactone, a nonselective aldosterone blocker, in the treatment of CSC. 17 Spirinolactone was initially developed in 1959 for the treatment of hypertension and heart failure. Unfortunately, spirinolactone has multiple progestational and antiandrogenic side effects due to its indistinguishable binding to other steroid receptors. Therefore, a new highly selective MR antagonist was developed and approved in 2003 in the United States, called eplerenone. Eplerenone has a higher selectivity and affinity compared to spironolactone and presents, therefore, fewer side effects. 18
Since then numerous new studies have been published on the topic debating the effectivity of oral MR antagonist in treatment of acute and chronic CSC.19–35
In 2018 Chatziralli et al. reviewed the literature until 2017 discussing the role of eplerenone in the treatment of CSC. They concluded that most of studies showed the effectiveness of eplerenone in the improvement of BVCA and a more rapid resolving of SRF, especially in the chronic stages. However, all those studies were retrospective with a short-term follow-up and small sample size. 21
Petkovsek et al. examined in 2019 the efficacy of eplerenone in the treatment of 83 patients with chronic CSC over a period of 3 years. Their primary outcome measure was the reduction in central subfield thickness. They showed that the primary beneficial effect of eplerenone occurred within the first year and that only a minority of patients had a complete resolution of SRF. They concluded that eplerenone was a well-tolerated, alternative treatment in selected patients, such as those who are not candidates for PDT. They believe that further studies are necessary to identify anatomical predictors of success in patients treated with eplerenone. 22
Bousquet et al. tried to identify factors that are predictive of the treatment response in patients with nonresolving CSC treated with spironolactone or eplerenone. They suggested that a thicker baseline choroid (>515 mm) was the only predictive factor associated with a more favourable treatment response. 14 Unfortunately we used the SD-OCT without the Enhanced Depth Imaging (EDI-OCT), which is needed to measure the choroidal thickness and, therefore, we were not able to confirm their results.
In 2019, Wang et al. published a meta-analysis, comparing the effect of MR antagonists (eplerenone or spironolactone) versus observation or placebo in the treatment of CSC. A total of 145 eyes of patients were included. The results were very promising and showed that MR antagonists significantly improved the BCVA in CSC patients. 23
We compared the results of the present study with five previous papers in Table 3. All papers confirmed the efficacy and clinical value of eplerenone for the treatment of patients with non-resolving CSC. They showed a significant reduction in central macular thickness (CMT) as well as in the mean height of subretinal fluid (SRF). Nevertheless, all agree that additional prospective, controlled studies in larger cohorts are needed to confirm these results and further explore the predictive factors to treatment response.14,22,25,31,34
Comparison of the clinical results with similar studies.
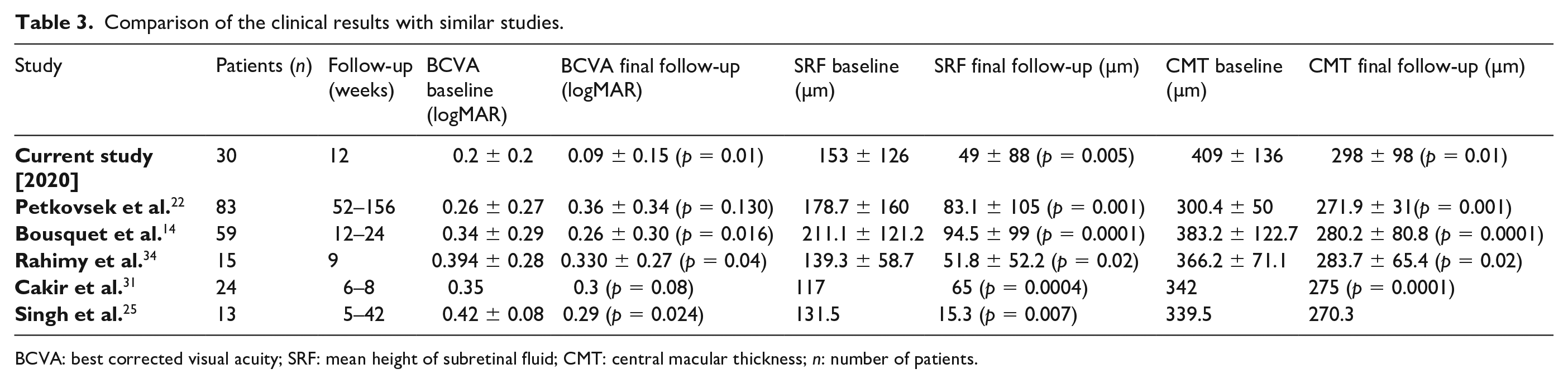
BCVA: best corrected visual acuity; SRF: mean height of subretinal fluid; CMT: central macular thickness; n: number of patients.
In this present study, eplerenone seems to be an effective treatment for patients with chronic CSC, especially those reporting having stress. Those results make sense, since cortisol is known to be the primary stress hormone and CSC has been clearly associated with increased levels of endogenous corticosteroids in the literature. 36 We believe future studies analysing stress with objective scales in collaboration with the psychological department could be interesting to further explore the complex physiopathology of CSC.
Main potential limitations
Main potential limitations of our study were the retrospective nature of the work. The variability of the single measures causes a statistical bias, because of the small patient cohort. This bias was corrected by using statistical formulas for small cohorts (non-Gaussian samples). Further studies with larger cohorts are eventually necessary to confirm our results and further explore possible predictive factors in the better treatment response of patients with chronic CSC.
Furthermore ‘stress’ was documented when asked during anamnesis, but we did not use molecular and/or survey tools to measure ‘stress’ objectively. Furthermore there were only nine patients in our non-responder group and therefore the significance is limited.
Conclusion
This study showed a statistically significant improvement of best corrected visual acuity and a significant reduction of macular thickness and subretinal fluid in patients with chronic CSC treated with oral eplerenone. This makes us assume that oral eplerenone is an effective treatment for patients with chronic central serous chorioretinopathy, especially in patients under stress. Further prospective studies are underway.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
This article does not contain any studies with animals performed by any of the authors.
Presentation
This study has been presented at:
1). DOG, Berlin, Germany, September 2019
2). SFO, Paris, France, May 2020