
Abstract
Background:
Vitreous floaters are a common and inconvenient phenomena. This study aims to examine the efficacy and safety in treating vitreous floaters using Nd:YAG laser vitreolysis.
Methods:
In this prospective double-blinded randomized clinical trial 24 eyes of twenty-four patients were randomized into intervention with YAG laser vitreolysis and control groups. Primary outcomes were visual disturbance on a 10-point scale, qualitative changes in a 4-level scale, contrast sensitivity measured with the Pelli-Robson table and the National Eye Institute Visual Functioning Questionnaire 25 (NEI VFQ-25). Secondary results included objective change in vitreous opacities, best-corrected visual acuity (BCVA), variation in intraocular pressure (IOP) and other adverse events.
Results:
Twenty-one patients (21 eyes; 5 male, 16 female) were enrolled in this study (mean age 62 ± 7.9 years), three were lost during follow-up. In the YAG laser group, the 10-point visual disturbance score improved a mean of 4.7 points (p < 0.001) compared to the control group that improved 2.1 (p = 0.09). The YAG laser group reported greater subjectively symptomatic improvement (77%) than controls (25%). NEI VFQ-25 revealed improved general vision (75.8 versus 59.2; p = 0.037) and in mental health at 6 months (84.3 versus 70.3; p = 0.048). There was no significant difference in contrast sensitivity (p = 0.848) and in IOP (p = 0.505). No differences in adverse events between groups were identified.
Conclusion:
Vitreolysis with Nd:YAG laser improves visual results in patients with symptomatic vitreous floaters, without adverse events considered clinically relevant. Other trials with a larger number of participants are required to corroborate these results.
Introduction
Floaters are visual phenomena caused by vitreous opacities often as a result of posterior vitreous detachment (PVD). 1 While most patients get used to the visual interference related with Weiss rings and other vitreous opacities, many find that they are extremely inconvenient. Studies published recently indicate that floaters can have a remarkably negative impact on quality of life.2,3
Once diagnosed, patients are generally managed conservatively. However, interventions aimed to improve floaters are progressively being take into consideration. These includes two procedures: vitrectomy, particularly small-gauge limited vitrectomy; and vitreolysis with Nd:YAG (neodymium-doped yttrium aluminum garnet) laser.
In addition to usual Nd:YAG laser indications, such as posterior capsule opacity or peripheral iridotomy, this method has also started to be used to vaporize vitreous opacities. 4 Unlike vitrectomy, it’s a less invasive procedure, avoiding the risk of endophthalmitis. Also, a vitrectomy-only procedure presents with a high-risk of cataract development 5 risk of which is lower in the laser procedure. This might be beneficial especially in younger patients willing to preserve their accommodation.
The mechanism of laser vitreolysis is a photodisruption of the vitreous aggregates, followed by displacement outside the visual axis. A prospective randomized study analyzed a series of 36 eyes submitted to vitreolysis with Nd:YAG laser and compared them with eyes submitted to a simulated laser vitreolysis procedure. A 54% improvement in the symptomatology of patients undergoing the real procedure was demonstrated, with no difference in side effects between the two groups. 6
Vitreolysis with Nd:YAG laser may represent an option with possible lower financial costs for the patient or the health system, less time consuming for not requiring hospitalization and less emotional wear on the patient due to the shorter overall process.
The present study aims to compare the effects of vitreolysis with Nd:YAG laser for the treatment of vitreous opacities comparing to a placebo procedure, analyzing the symptoms reported by the patient and signs observed by the researcher.
Methods
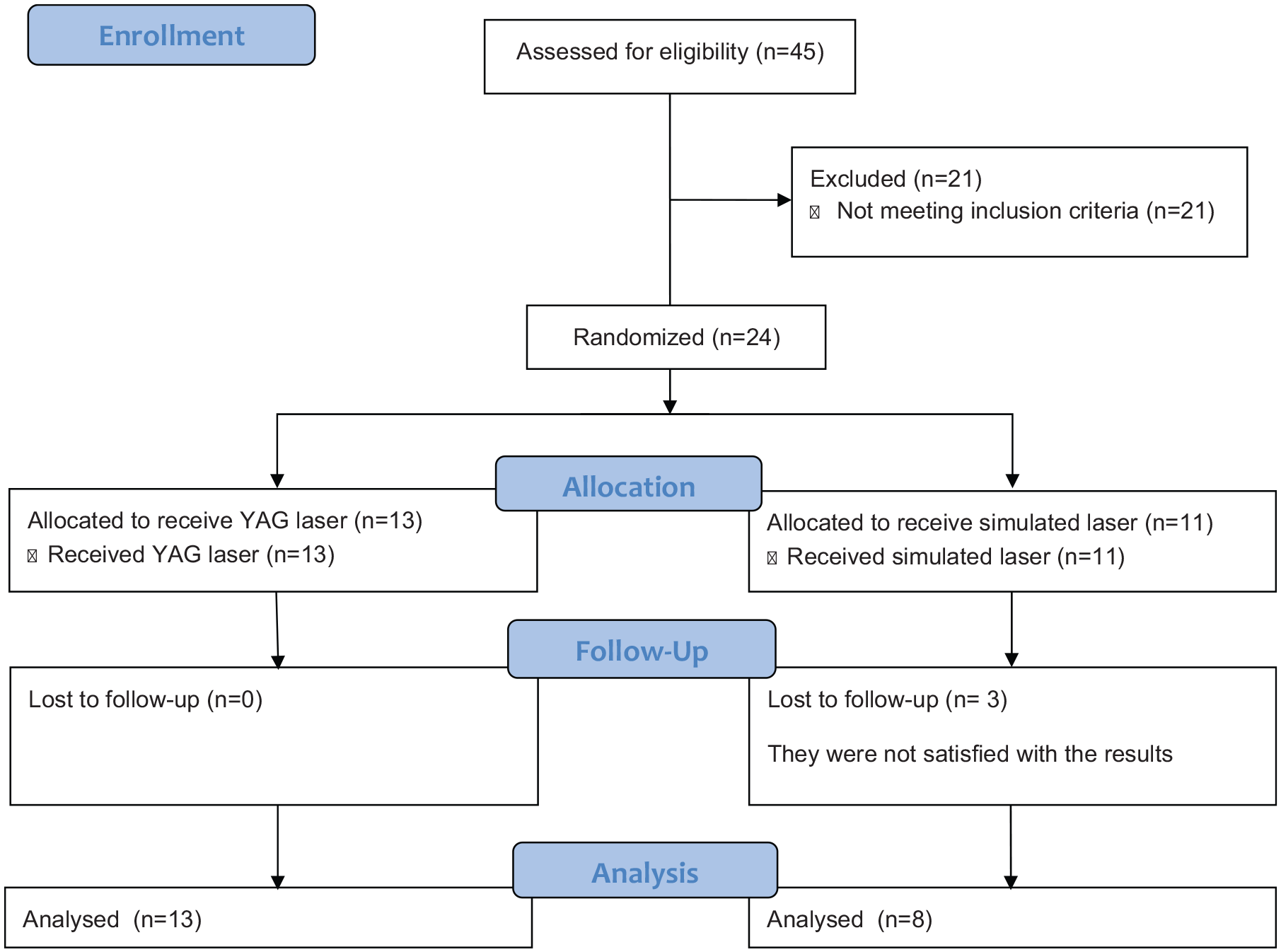
CONSORT flow diagram.
The following inclusion criteria were applied: symptomatic vitreous opacities due to PVD, including Weiss rings, symptoms for at least 6 months, posterior vitreous detachment reported in clinical examination and ocular ultrasound (B-scan), vitreous opacity located at least 5 mm from the lens, if phakic and 3 mm from the retina, and a visual discomfort of at least 4 on a scale of 0 to 10 points, with 0 being asymptomatic and 10 indicating impairing symptoms.
The study excluded patients with visual acuity worse than 0.4 logMAR in the fellow eye, history of retinal detachment, retinal tear, uveitis, glaucoma using two or more drugs, previous macular edema and aphakia, or other associated diseases that may compromise data analysis and patients that refused to sign the informed consent form.
All patients were followed for 6 months, except for three patients of the control group that were lost in follow-up due to dissatisfaction of the results. The primary outcomes measured at that time were visual disturbance score of 10 points, as described by Singh, 7 qualitative 4-level scale, described by Delaney et al., 4 contrast sensitivity measured with the Pelli-Robson table and the National Eye Institute Visual Functioning Questionnaire 25 (NEI VFQ-25) adapted to Portuguese. 8 Of these, the NEI VFQ-25 is the only validated method. Secondary results included best-corrected visual acuity (BCVA), objective changes in vitreous opacities, based on the masked classification of fundus photography, variation in intraocular pressure (IOP) and other adverse events.
Patient age, sex, lens status, BCVA and contrast sensitivity were recorded. B-scan ocular ultrasonography (VuPad Ophthalmic Ultrasound, SonomedEscalon, Lake Success, NY), color retinography (Visucam 524 Fundus Imaging, Zeiss Meditec, Dublin, CA), optical coherence tomography (Cirrus 4000 HD OCT, Zeiss, Dublin, CA), slit lamp examination, indirect ophthalmoscope examination and applanation tonometry were performed.
Control group participants received matching treatment; the same lens was positioned, however, a paper filter was placed on the surface to prevent the laser energy from passing through the lens. The YAG laser energy was at its lowest setting of 0.1 mJ.
BCVA and contrast sensitivity were measured, color fundus photography, optical coherence tomography, slit lamp examination, indirect ophthalmoscopy and applanation tonometry were performed again in the sixth month after the procedure. A blinded evaluator rated the fundus photography for the presence of floaters using the same qualitative 4-level scale used by patients to report their postoperative symptoms compared to the baseline. The following percentages were used to quantify the level of improvement: 0% or worse; limited success, 30% to 50%; pronounced success, 50% to 70%; and total success, 100%. 4
The normality of the variables was tested using the Shapiro Wilk test. The evaluated variables were presented in tables with absolute and relative frequency distribution. Associations were tested using Pearson’s Chi-square test or Fisher’s exact test, when necessary. The statistical significance of the differences in means between the quantitative variables were verified using the paired and unpaired t-Student test. The differences in variances were verified through analysis of variance (ANOVA) with repeated measures, used to evaluate the different times within a group. All analyzes were performed with a significance level of 5%, therefore, the results considered statistically significant are those whose p value was less than 0.05, always considering two-tailed alternative hypotheses.
Results
Study population characteristics.
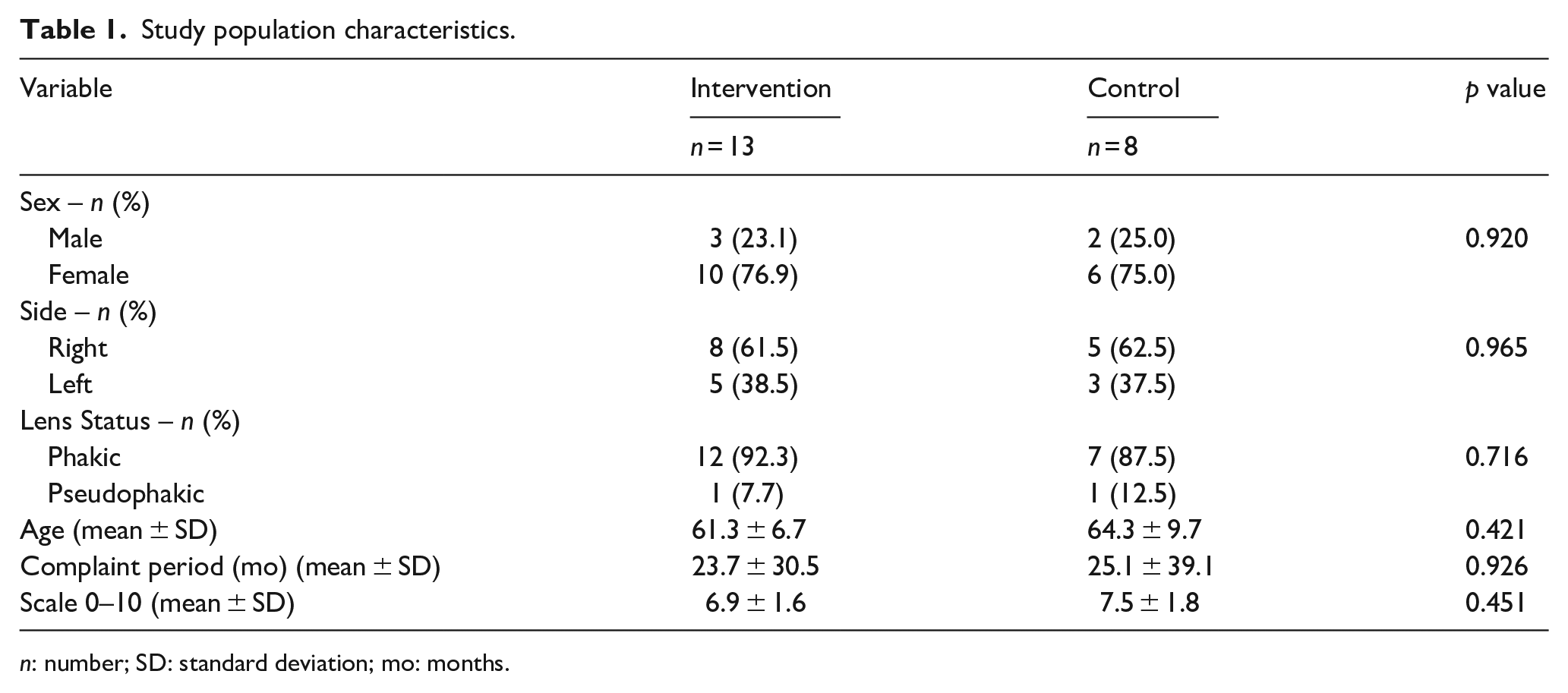
n: number; SD: standard deviation; mo: months.
In the intervention group, the 0 to 10 pre-procedure scale was 6.9 ± 1.6 points and, after 6 months, it was 2.2 ± 2.2, showing a significant reduction (p < 0.001). The control group went from 7.5 ± 1.8 to 5.4 ± 2.8, showing no relevant reduction (p = 0.09). The difference between the groups, in sixth month evaluation, was -3.2 (p = 0.011).
The changes observed in BCVA and in contrast sensitivity were not relevant in any of the groups, as shown in Table 2.
Best-corrected visual acuity and contrast sensitivity measurements.
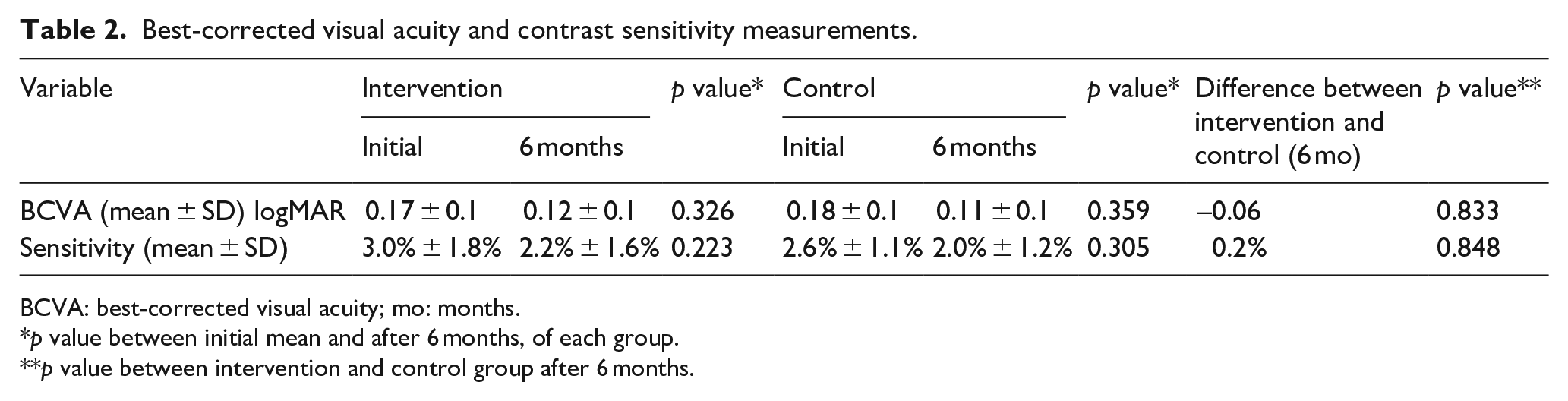
BCVA: best-corrected visual acuity; mo: months.
p value between initial mean and after 6 months, of each group.
p value between intervention and control group after 6 months.
Figure 2 shows that most patients in the intervention group subjectively reported a pronounced improvement (46.2%), followed by a complete improvement (30.8%), while most of the control group reported a limited improvement (50.0%). The blinded evaluator graded 53.3% of the intervention group patients with a pronounced improvement and in the control group 62.5% with limited improvement.
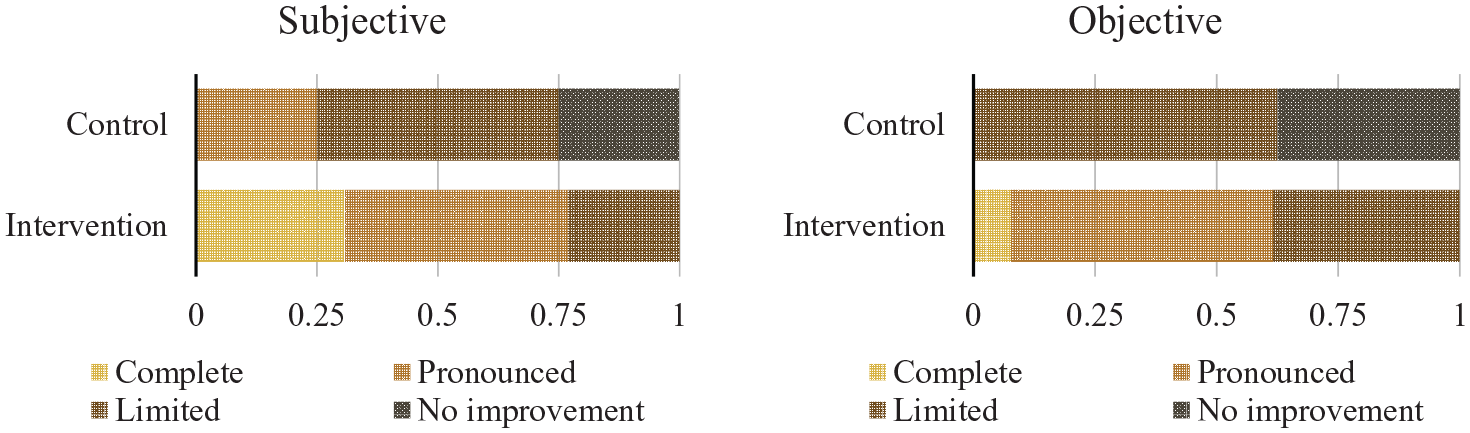
Subjective and Objective grading of floaters 6 months after procedure.
IOP comparison between groups.
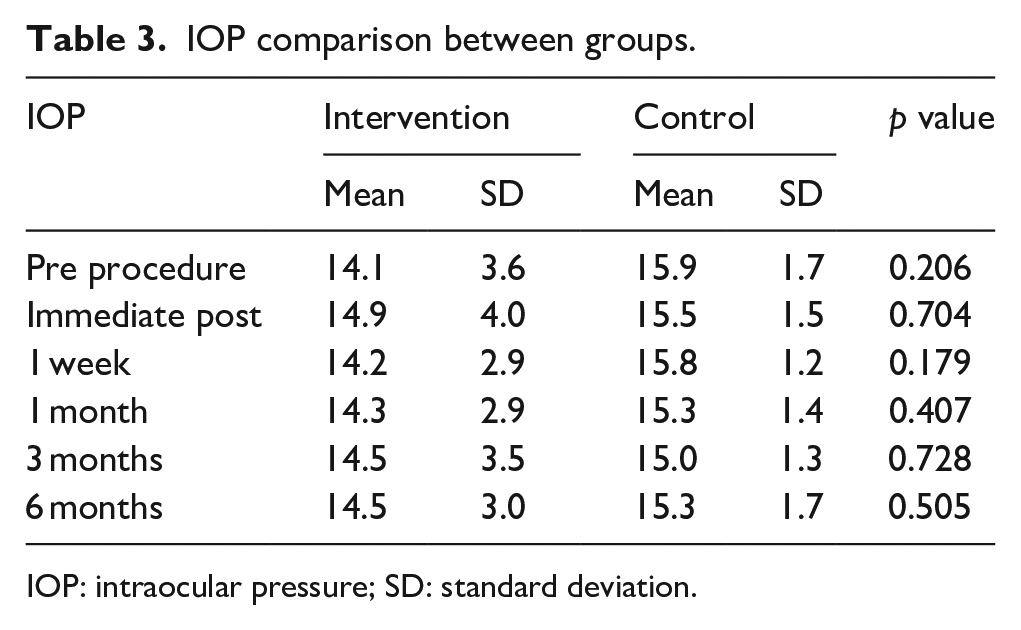
IOP: intraocular pressure; SD: standard deviation.
Discussion
The present study reported a significant improvement in floaters symptoms after a single laser YAG session. With 77% of the patients in the intervention group reporting a pronounced or complete improvement, when compared with only 25% in the control group. These data are aligned with the findings by Shah et al. that achieved 53% significant or complete improvement in a similar study with 36 patients.
These results seem to show better effectiveness of the procedure than those presented in an analysis of 39 patients treated by Delaney et al. In this study, a maximum pulse energy of 1.2 mJ with a total mean power of 510 mJ were used. Only 38% of patients reported moderate or significant benefit from treatment and none reported complete improvement. This fact can be explained by the power used in the procedure. The mean total energy in the present study and in the study by Shah et al. was 0.8 J and 1.3 J respectively, and the maximum energy per pulse was 7.2 mJ and 7.0 mJ, well above the 1.2 mJ used by Delaney et al. In the control group, a limited improvement (30-50%) was reported in 50% of the cases, suggesting a placebo effect by the simulated procedure or a neuroadaptation over time.
On the symptoms scale of 0 to 10, there was a considerable improvement in the intervention group, improving 4.7 points on average. The control group achieved an improvement of 2.1 points, which can also be explained by a placebo effect. Again, these data are in line with those previously demonstrated by Shah et al., that obtained an improvement of 3.1 points on average in the intervention group.
Two variables were added that were not described in the study by Shah et al., the intraocular pressure variation and the contrast sensitivity measure. There was no persistent increase in IOP in patients undergoing vitreolysis with Nd:YAG laser compared to the control group, suggesting that this is a rare adverse effect of the procedure and that there is no need to use eye drops prophylactically for the purpose of controlling the IOP after performing it. There was also no difference in contrast sensitivity before and after treatment, this being one of the measures suggested by Lim, JI in a commentary on the study by Shah et al., 10 since it was described that the contrast sensitivity is reduced in patients with vitreous opacities at the pre-macular region. 11 Although there are studies showing increase in contrast sensitivity after YAG laser. 7
Two variables of the NEI VFQ-25 showed improvement: the general vision and the mental health. In accordance with other studies that showed a relationship between vitreous opacities and their negative impact on quality of life.2,3
During the study, there was a slight discrepancy between the subjective evaluations of the patients and the objective evaluation through fundus photography. Where 30.8% of patients in the intervention group reported complete improvement. Only 7.7% of the photographs evaluated obtained this assessment, suggesting that the simple dispersion of the vitreous opacities, without their complete extinction, already improves the symptoms reported by the patient. These data may vary according to the population studied, the degree of demand and the expectations created around the procedure.
No significant adverse effects were reported during the 6-month follow-up period, including no cystoid macular edema or macular hole after careful OCT evaluation, pre and post procedure. Only five patients in the intervention group reported slight visual turbidity during the first hours after the procedure, with spontaneous resolution. Due to the limited number of patients in the study and limited follow-up period, it cannot be said that it is a procedure without adverse effects, but that the careful selection of patients and the correct use of the technique significantly reduce these risks. A recent study analyzing a long-term follow-up of patients submitted to YAG vitreolysis reported three cases of retinal tear after 1.4 to 2.8 years of the procedure. 12 A longer follow-up of these patients would optimize the safety profile of this procedure.
This study has some limitations, including the small sample size and short follow-up. However, the dissemination of the technique and safety assessment allow new studies to be conducted and more robust data to be presented. Thus, as the study by Shah et al., only one laser session was performed, however, in a real-life scenario, it may be necessary to carry out more sessions for the complete resolution of opacities, which, theoretically, would further increase its effectiveness.
Conclusion
The present study suggests that vitreolysis with YAG laser improves visual results without adverse events considered clinically relevant during a 6-month follow-up. It may be suited for patients with relevant floaters symptoms, due to complete posterior vitreous detachment, clinically and ultrasound (B-scan) confirmed.
Footnotes
Authors’ note
The authors have not presented this article in a meeting or conference.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Clinical Trial Registration
The authors have registered this clinical trial at the Brazilian Registry of Clinical Trial under the code: RBR-2jq3v.
Ethical approval
This research was approved by the Ethics Committee of Hospital do Servidor Público Estadual under the number: 2.755.274