
Abstract
Purpose:
We describe the characteristics of an isolated retinal cavernous hemangioma in a young female patient using multimodal imaging.
Case description:
Fundus examination of the right eye showed a large vascular mass, composed by clusters of dark red and dilated saccular angiomatous formations with superficial whitish fibroglial tissue and hemorrhages, located in the inferonasal peripheral retina, along the vascular arcade. On green-light fundus autofluorescence the lesion appeared hypoautofluorescent, with moderately hyperautofluorescent areas. On multiColor imaging it showed mainly a green pseudocolor, with knobby surface and well-defined irregular margins. Fundus fluorescein angiography showed early hypofluorescence within the tumor mass and late incomplete staining, without leakage. Ocular ultrasonography documented an elevated well-defined hyperechogenic lesion, with high internal reflectivity, without choroidal excavation, retinal detachment, or acoustic shadowing. Swept source optical coherence tomography showed multilobulated cavernous formations, varying in size, containing for the greatest part hyperreflective material, within an interconnecting fibrous scaffold and with an overlying partially adherent epiretinal membrane. Optical coherence tomography angiography documented a few highly reflective, tortuous and abnormal branching veins extending into the tumor mass, with a root-like appearance, and surrounding nodular changes, corresponding to the angiomatous formations.
Conclusions:
Different imaging modalities can be used in combination for a better evaluation of the pathological features of this rare vascular tumor.
Introduction
Retinal cavernous hemangioma (RCH) is a rare benign vascular tumor composed of grapelike clusters of thin-walled saccular angiomatous lesions located in the inner retina. 1 RCHs may occur most frequently in isolation or as part of an autosomal dominant hereditary disease, associated with similar intracranial and skin lesions.1,2 RCHs may vary in size and location and are mostly located along the course of a major retinal vein. Peripheral lesions are usually asymptomatic; loss of vision may occur in case of macular involvement, vitreous hemorrhage, or pre-retinal traction. 2 The diagnosis is based on clinical examination and is confirmed by retinal imaging. 2 Herein, we describe the features of a RCH case using a multimodal imaging approach.
Case report
A 15-year-old girl was referred to our Ocular Oncology Unit for a suspected retinal vascular lesion in her right eye (RE). She was in good general health condition and her past ocular history was unremarkable. She had no family history of ocular or neurological disorders. Routine blood tests with renal and hepatic function were normal. Best-corrected visual acuity was 20/20 in both eyes on Snellen chart. Anterior segment and intraocular pressure were normal bilaterally. Dilated fundus examination of the RE showed a large vascular mass in the inferonasal peripheral retina, along the vascular arcade. The lesion was composed by clusters of dark red and dilated saccular angiomatous formations with superficial whitish fibroglial tissue and hemorrhages. Dot-and-blot hemorrhages were visible on the surrounding retina, while there were not evident lipid exudates. The optic nerve, the posterior pole and the retinal vasculature were normal. The clinical aspect of this vascular lesion was compatible with a RCH. There were no significant findings in the fellow eye. The aspect of the lesion on ultra-wide-field fundus imaging (Daytona Optos, Marlborough, MA, USA) and color fundus photography (DRI Swept Source OCT Triton, Topcon Corporation) are shown in Figure 1(a) and (c). On MultiColor imaging (Heidelberg Spectralis HRA OCT, Heidelberg Engineering, Heidelberg, Germany) the lesion showed mainly a green pseudocolor, corresponding to the whitish fibroglial tissue observed on color fundus photography, with well-defined irregular margins (Figure 1(d)). Multicolor image modality highlighted the knobby surface of the lesion and allowed us to appreciate the tumor elevation thanks to a pseudo-three-dimensional visualization. On green-light fundus autofluorescence (FA) (Daytona Optos) the RCH appeared as a hypofluorescent lesion with moderately hyperautofluorescent areas, corresponding to the overyling fibroglial tissue, while the surrounding retina appeared normally isoautofluorescent, except for an area below the lesion which showed hyperautofluorescent spots (Figure 1(b)).
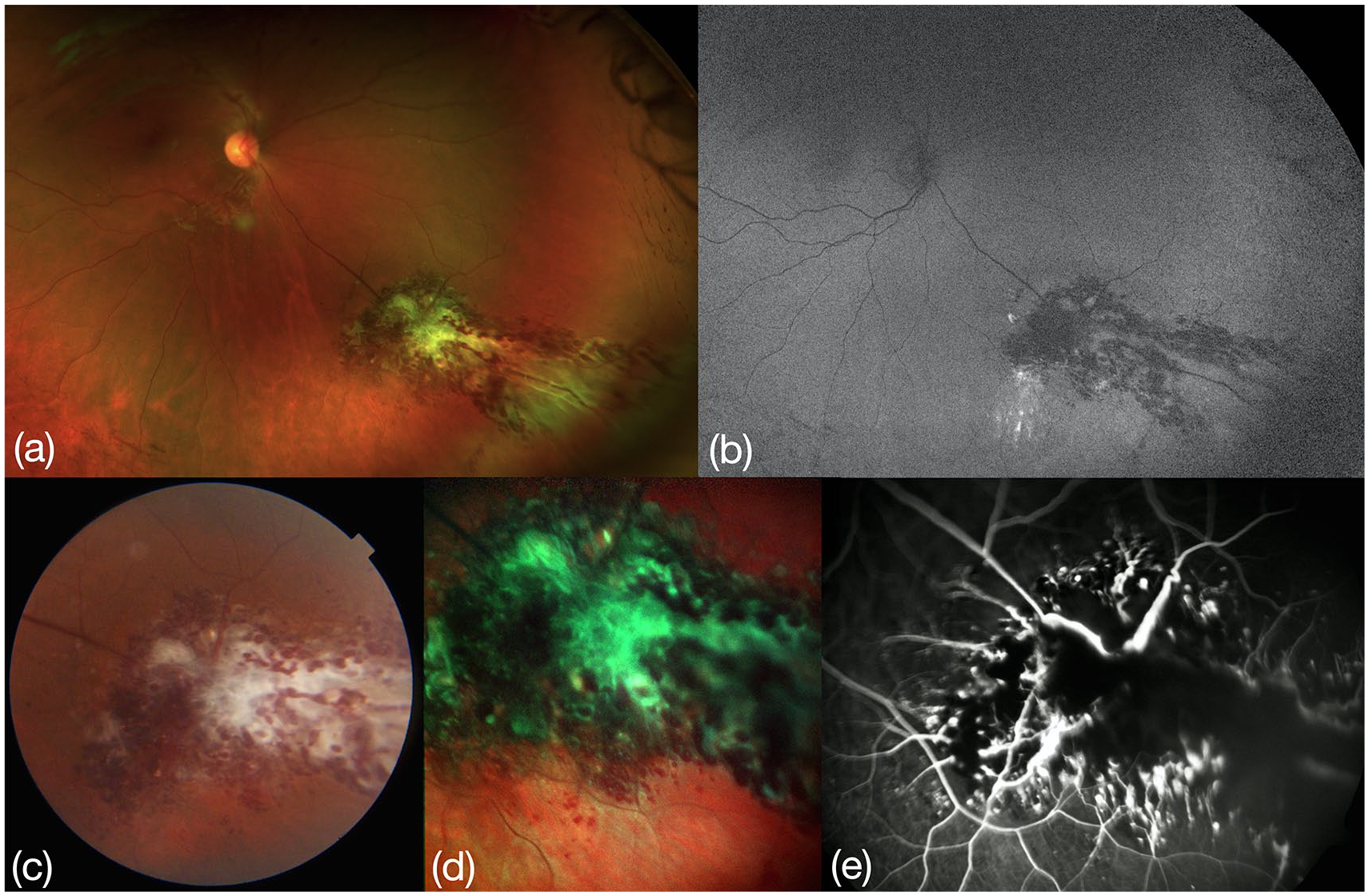
(a) Ultra-wide field fundus imaging (Daytona Optos, Marlborough, MA, USA), (b) fundus autofluorescence imaging (Daytona Optos), (c) color fundus photography (DRI Swept Source OCT Triton, Topcon Corporation), (d) MultiColor imaging (Heidelberg Spectralis HRA OCT, Heidelberg Engineering, Heidelberg, Germany), and (e) fundus fluorescein angiography (FF450 Retinograph, Carl Zeiss Meditec, Jena, Germany).
Fundus fluorescein angiography (FFA) (FF450 Retinograph, Carl Zeiss Meditec, Jena, Germany) showed early hypofluorescence within the tumor mass due to the slow filling of the angiomatous lesions, and late incomplete staining, without leakage; the surrounding retina appeared normally perfused (Figure 1(e)).
Ocular ultrasonography (Aviso S, Quantel Medical, Paris, France) documented an elevated well-defined hyperechogenic lesion, with high internal reflectivity on A-scan, measuring 6.2 × 7.0 mm in basal diameters and 4.4 mm in thickness. No choroidal excavation, retinal detachment or acoustic shadowing were observed on B-scan ultrasonography (Figure 2(a)). The ultrasound biomicroscopy (Aviso S) showed the more anterior component of the lesion, in which the morphological features of RCH, such as the irregular surface and the cystic spaces, were well appreciable (Figure 2(b)).
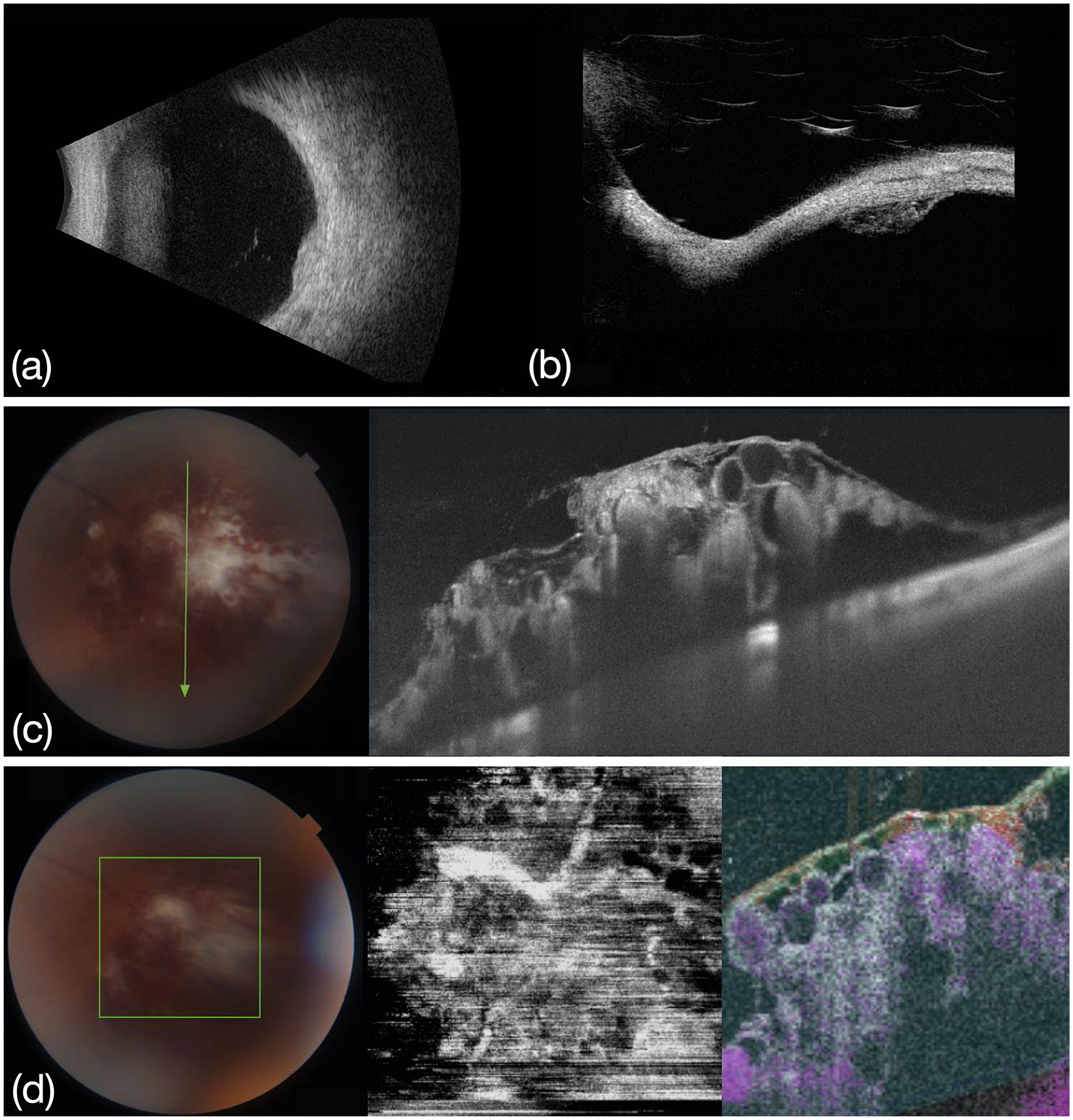
(a) B-scan ocular ultrasonography (Aviso S, Quantel Medical, Paris, France), (b) ultrasound biomicroscopy (Aviso S, Quantel Medical, Paris, France), (c) SS-OCT scan (DRI SS-OCT Triton), and (d) SS-OCTA en face 6 × 6 mm scan (at the center) and cross-sectional scan (on the right) (DRI SS-OCT Triton).
Swept source optical coherence tomography (SS-OCT) (DRI Swept Source OCT Triton) showed multilobulated cavernous formations, varying in size, corresponding to thin-walled vascular structures, containing for the greatest part hyperreflective material, within an interconnecting fibrous scaffold and with an overlying partially adherent epiretinal membrane with traction (Figure 2(c)). Some vesicle formations were empty and showed very low reflectivity. Swept source optical coherence tomography angiography (OCTA) (DRI Swept Source OCT Triton) en face scan documented a few highly reflective, tortuous and abnormal branching veins extending into the RCH, with a root-like appearance, and surrounding nodular changes, corresponding to the angiomatous formations (Figure 2(d)). Cross-sectional OCTA scans showed low flow blood circulation inside the lesion. The lesion remained stable during a 15 months follow-up, without documented growth or ocular complications. In the meantime, the patient underwent magnetic resonance imaging of the brain and complete ultrasound examination of the abdomen which were negative for extraocular lesions.
Discussion
RCH is a rare vascular hamartoma, mostly found in female patients, which appears as a grapelike clusters of blood-filled saccular aneurysms with interconnecting fibroglial tissue.1,2 RCHs are generally non-progressive and do not require treatment.2,3 Diagnosis of RCH can be made from the characteristic fundoscopic aspect combined with the imaging findings. 3 In our case the ocular ultrasonography showed a well-defined hyperechogenic lesion with high internal reflectivity, which was consistent with the published literature. 3 The lack of acoustic shadowing or choroidal excavation on ultrasonography allows to differentiate these lesions from malignant ones, like melanomas and retinoblastomas. 4 FFA is the most commonly used ancillary exam to support the diagnosis of RCH. RCH appears on FFA as a hypofluorescent lesion in the early phase, with delayed incomplete perfusion in the mid and late phases and no evidence of leakage. This appearance reflects the stagnant blood flow and the plasma–erythrocitic separation within the aneurysms, which are isolated from the retinal circulation.2,5 The absence of fluorescein leakage is helpful to differentiate RCH from other retinal vascular lesions. 3 The SS-OCT scans of RCH show multiple hyporeflective saccular formations within hyperreflective material, corresponding to the separation of the plasma from the blood cells and involving the inner retinal layers. 6 The angiomatous lesions are isolated and show no blood vessel connections to the retina. Furthermore, OCT generally shows a dense fibrous tissue membrane covering the tumor surface and the space between the vascular lesions, as an interconnecting scaffold. It has been hypothesized that this superficial membrane causes multiple adhesion tractions leading to retinal tortuosity and dilatation, and even hemorrhagic complications in absence of vitreous detachment. 7 The increased surface gliosis may be consequent to spontaneous thrombosis. 8 The superficial fibroglial component appeared as moderately hyperautofluorescent on FA imaging and it showed mainly a greenish color on MultiColor imaging.
OCTA findings in RCH are described in few reports.6,7,9,10 OCTA shows characteristic vascular changes of RCH ad has good correspondence with fundus imaging and FFA findings; moreover, OCTA image is less affected by glial fibrosis compared with other imaging examinations. 9 In our case, OCTA confirmed the low flow circulation inside the angiomatous lesions, suggesting the independence between the blood flow inside the lesion from the normal retinal blood flow.
Conclusion
We described the multimodal imaging analysis of an isolated RCH in a young female patient. The different imaging modalities provide complementary information and can be used in combination for an accurate and detailed evaluation of the pathological features of RCHs.
Footnotes
Authors’ note
The manuscript has not been presented at any meeting.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
The patient parents gave their consent for the publication of this case.