
Abstract
Background:
To investigate the long-term effect of serous choroidal detachment on the success of trabeculectomy in glaucoma patients.
Methods:
In this case-control study, 17 patients who underwent trabeculectomy and developed choroidal detachment, and completed at least 3 years of follow-up were included. The controls were matched based on age, sex, preoperative intraocular pressure, and glaucoma type, and lack of choroidal detachment. Surgical success was defined based on two definitions of 5 < IOP < 16 and 20% reduction from the baseline and no need for further glaucoma surgery and all the same but 5 < IOP < 22.
Results:
The mean estimated duration of survival ±SD was 2.73 ± 0.35 years (CI 95% 2.1, 3.4), which was significantly shorter than 3.98 ± 0.38 years (CI 95% 3.3, 4.7) in the control group. (LogRank = 5.03 p = 0.02). Cumulative probability of success was 76.5%, 52.9%, 29.4%, 17.6%, and 11.8% in year 1, 2, 3, 4, and 5 in the case group, respectively. Corresponding values were 88.2%, 82.4%, 68.6%, 58.8%, and 47.1%. In the control group, respectively. At baseline, average IOP was 22.3 ± 2.7 and 23.8 ± 8.3 mmHg in the case and control groups, respectively (p = 0.17). Mean IOP was significantly higher in the case group than in the control group in years 2, 3, 4, and 5.
Conclusion:
Serous choroidal detachment affects the long-term surgical success of trabeculectomy, especially in patients with advanced glaucoma when lower target pressure is required.
Introduction
Trabeculectomy, since its first introduction in 1967, has long been the procedure of choice in the surgical management of glaucoma. While its long-term success in the control of intraocular pressure (IOP) and lower number of required glaucoma medications, higher rate of postoperative complications, especially after antimetabolite use is among the major drawbacks of trabeculectomy. 1
Choroidal detachment, an early-onset complication after trabeculectomy, occurs intraoperatively and most commonly postoperatively. 2 In other words, the separation of choroidal tissue with the accumulation of fluid in serous detachments and blood in hemorrhagic detachment occurs. Older age, higher preoperative IOP, tachycardia, systemic hypertension, and poor surgical techniques are among the possible risk factors for choroidal detachment.2 –4
The incidence of serous choroidal effusion after trabeculectomy widely varies in different studies, and it has been reported to be between 7.9% and 18.8%.5 –10 The high incidence of choroidal detachment after trabeculectomy makes this event a common complication requiring unique attention to both prevention and management. Choroidal effusion has been recognized as a cause of permanent visual loss in various reports.9 –11 However, it is a common complication, its long-term effects on the surgical success of trabeculectomy have not yet been determined.
Monteiro et al. 12 investigated three different methods in the management of the flat anterior chamber and concluded the superiority of medical management when visual acuity was the primary goal and AC reformation with viscoelastic when lowering IOP in the long term was the main goal. Kim and Jung 13 reported a similar long-term success rate among patients with the flat anterior chamber than among patients with normal AC. Five out of 23 patients had the choroidal detachment in their flat chamber group. Although the choroidal detachment was more common in the flat AC group, its direct effects have not been investigated in the long term. Consequently, Benson et al. 14 investigated the presence of hypotony within the first month after the surgery as a risk factor for the failure in a case-control study and concluded its adverse long-term effects.
The present study aimed to understand the effects of choroidal effusion on surgical success in the short- and long-term. We hypothesized that choroidal effusion might lead to lower surgical success in the long term.
Methods
In this case-control study, all patients, who underwent trabeculectomy from 2000 to 2015 in an academic tertiary ophthalmology center, developed choroidal detachment and completed at least 3 years of follow-up, were included. Exclusion criteria were uveitic or neovascular glaucoma, previous intraocular surgery or surgery in the follow-up, and incomplete follow-up data for less than 3 years. The protocol of the study was approved by a local ethics committee that is equivalent to an institutional review board. The study adhered to the tenets of the declaration of Helsinki.
The controls were matched according to age (within 2 years), sex, preoperative IOP (within 3 mmHg), glaucoma type, and presence of systemic disease (HTN and DM), and they were selected from the same database of patients who underwent trabeculectomy. Seventeen patients were entered in each study group.
All surgeons 3 performing trabeculectomy were glaucoma specialists with at least 5 years of surgical experience. All procedures were limbal-based trabeculectomy with the use of 0.1 cc MMC 0.01% for 2 min applied by a sponge in the presumed bleb area before scleral flap formation. A triangular or a rectangular partial-thickness scleral flap was made. After fashioning a paracentesis, a block of sclera under the scleral flap was excised and an iridectomy was made. The scleral flap was closed with interrupted 10–0 nylon sutures.
The patients’ records were reviewed by two ophthalmologists, and the required data, including IOP, glaucoma medications, and other ocular surgeries at baseline, and at different intervals, glaucoma type, and intraoperative or postoperative complications were extracted from the patients’ records. Glaucoma diagnosis was provided by a glaucoma specialist.
Surgical success was defined based on two criteria. The first definition was considered 5 < IOP < 16 and more than 20% reduction from the baseline (Criterion A). The second definition was 5 < IOP <22 and more than 20% reduction from the baseline (Criterion B). Loss of visual acuity to the amount of no light perception, and the need for further glaucoma procedure were also considered failures in both definitions.
Statistical analysis
To present data, we used mean, median and standard deviation. Normality of the data was assessed using the Kolmogorov-Smirnov test. T-test, chi-square and fisher exact test were used for the univariate analysis. Kaplan-Meier survival analysis was used to evaluate the cumulative probability of success, and the Log-Rank test was used to compare the two study groups. All analyses were conducted using the SPSS software version 25.0 (IBM, SPSS, Inc., Chicago, IL, USA).
Results
Seventeen eyes of 15 patients were included as cases and 17 patients were included as matched controls. The mean age of the patients in the case and control groups was 53.7 ± 14.2 and 53.5 ± 12.6 years, respectively (p = 0.96).
Thirteen patients were male in both groups. Two groups were also comparable in terms of F/U duration and refractive error (Table 1).
Baseline characteristics of study participants.
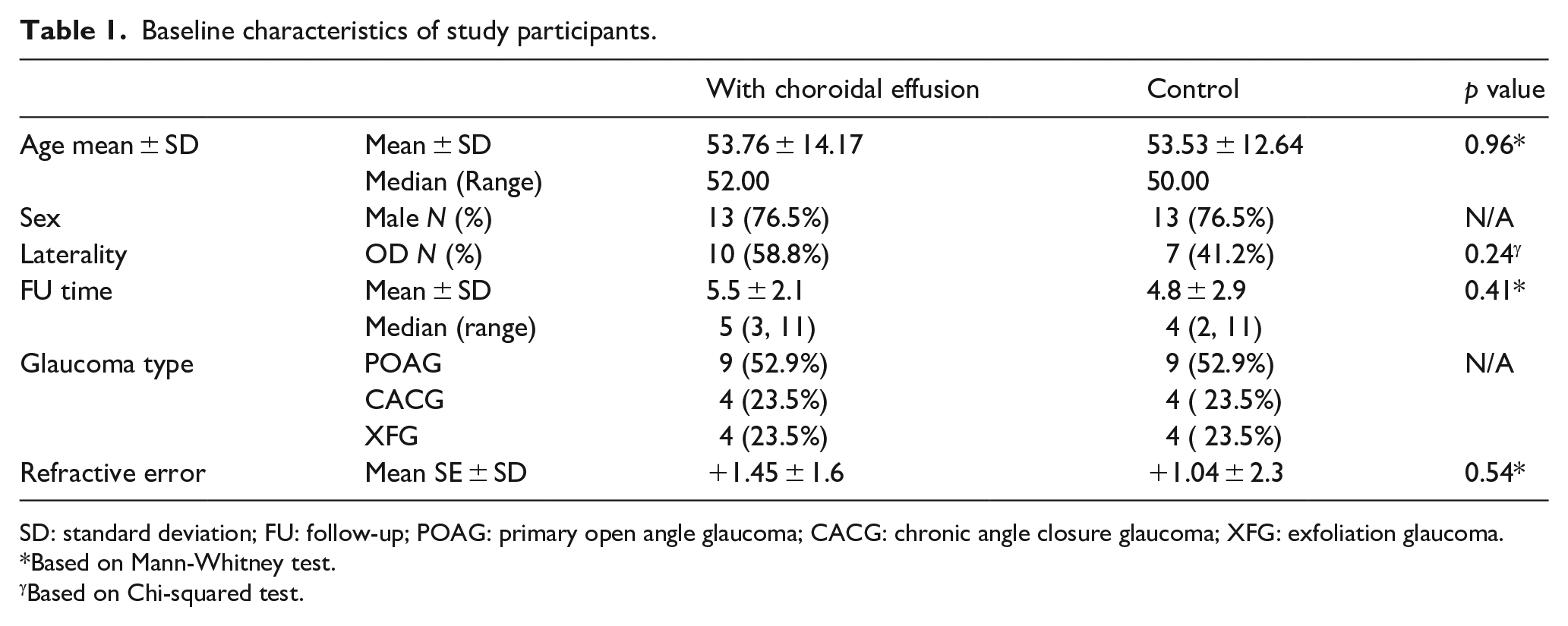
SD: standard deviation; FU: follow-up; POAG: primary open angle glaucoma; CACG: chronic angle closure glaucoma; XFG: exfoliation glaucoma.
Based on Mann-Whitney test.
Based on Chi-squared test.
The mean estimated duration of survival ±SD was 2.73 ± 0.35 (CI 95% 2.1, 3.4) years, which was significantly shorter than 3.98 ± 0.38 (CI 95% 3.3, 4.7) years in the control group (LogRank = 5.03, p = 0.02). Cumulative probability of success was 76.5%, 52.9%, 29.4 %, 17.6%, and 11.8% in years 1, 2, 3, 4, and 5. Corresponding values were 88.2%, 82.4%, 68.6%, 58.8%, and 47.1%, in the control group, respectively. Considering the second success definition, the two groups were comparable in terms of success (Figure 1).
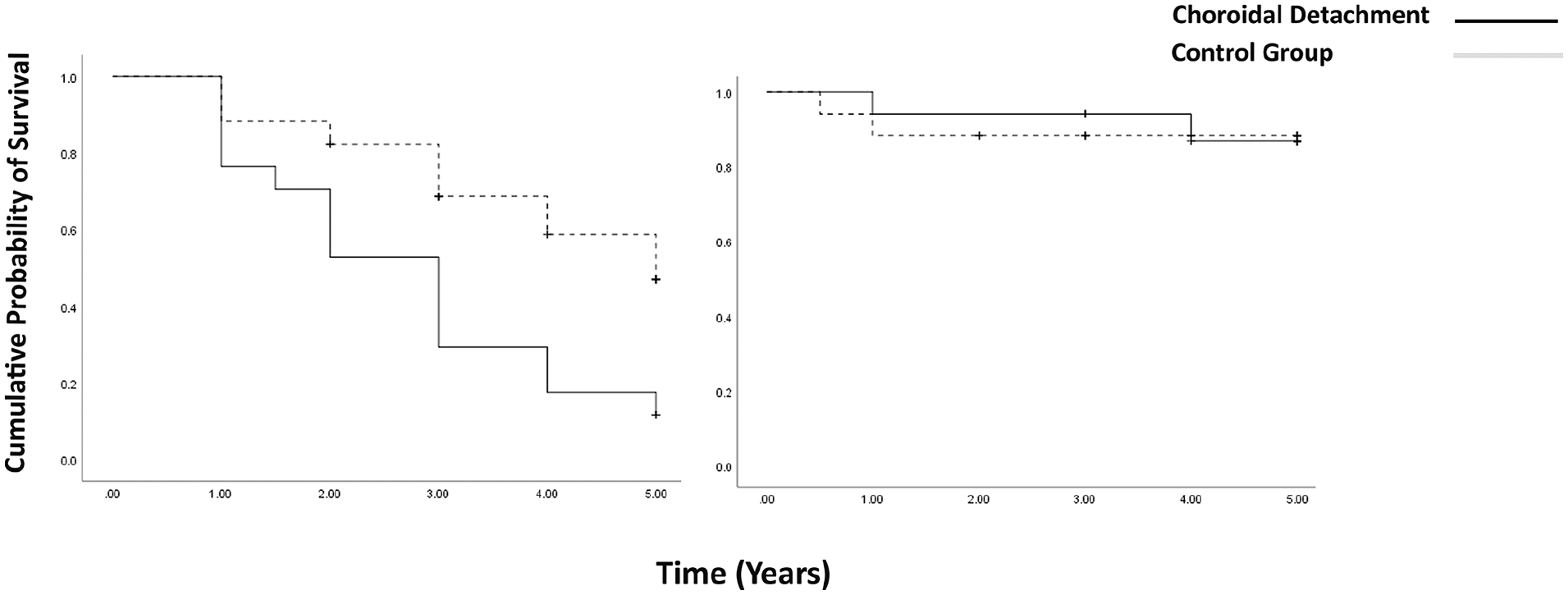
Kaplan-Meier curve showing cumulative probability of success in cases and controls over a 5-year period based on first success definition (5 < IOP < 16 and 20% reduction from the baseline) in the left and the second definition (5 < IOP < 22 and 20% reduction from the baseline) in the right.
At baseline (p = 0.17), the average IOP ± SD in the case and control groups was 22.3 ± 2.7 mmHg and 23.8 ± 8.3, respectively. The mean IOP was significantly higher in the case group than in the control group in years 2, 3, 4, and 5 (Table 2 & Figure 2). The mean reduction of IOP was 29 % and 46 % in the case and control groups in year 5, respectively (p = 0.04).
Intraocular pressure in study groups within the study intervals.
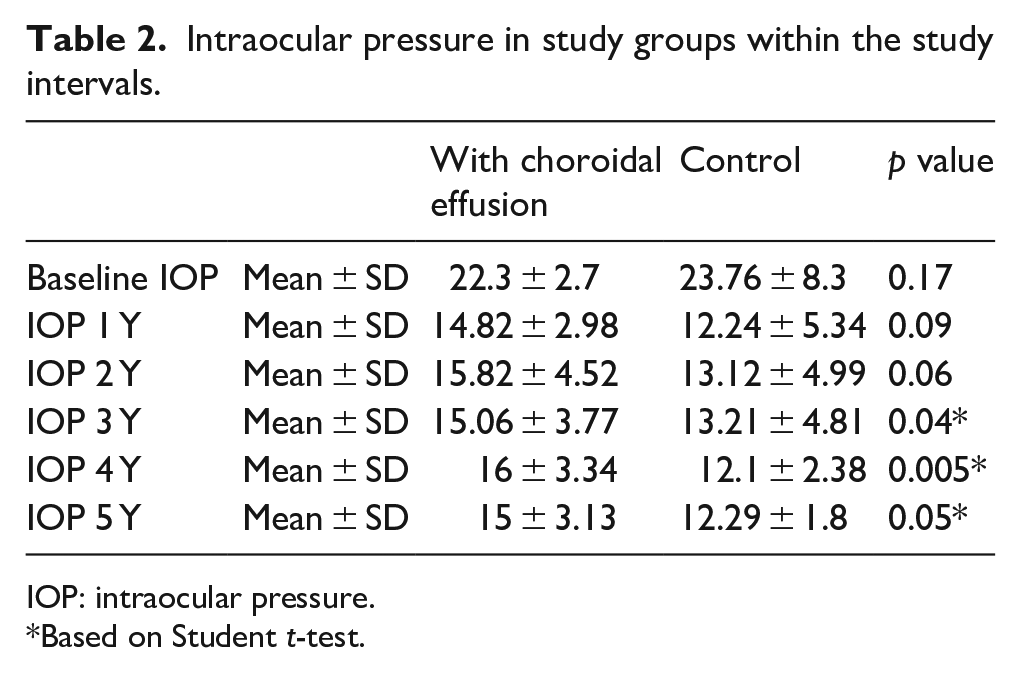
IOP: intraocular pressure.
Based on Student t-test.
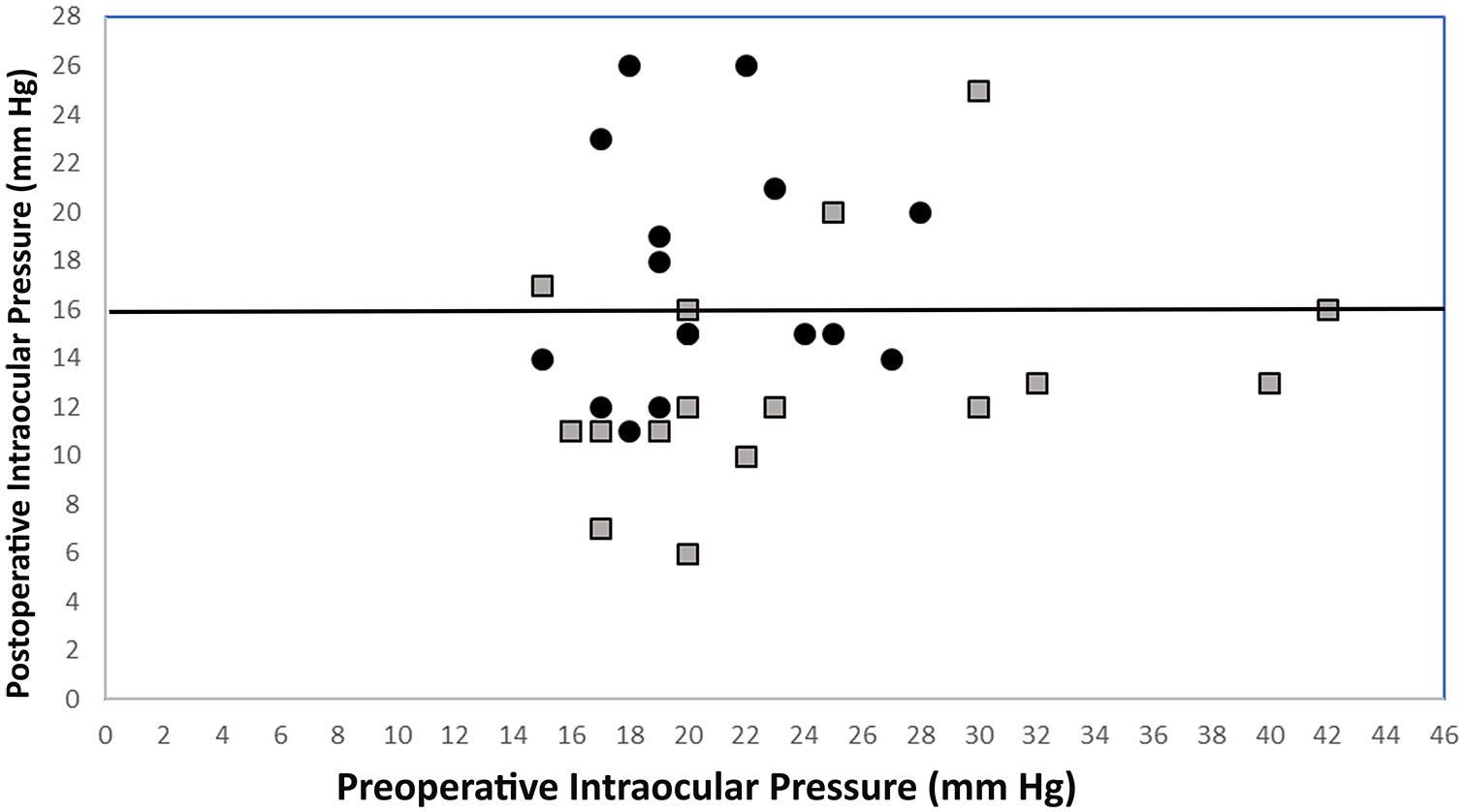
Scatterplot of preoperative intraocular pressure (IOP) versus postoperative IOP at the final visit. Black circles represent cases while grey rectangular shapes denote controls.
At baseline, two groups were similar in terms of glaucoma medication with a median of 3 in both groups. During the follow-up, the mean required number of medications was significantly higher in the case group than in the control group (Table 3).
Glaucoma medication within the study period.
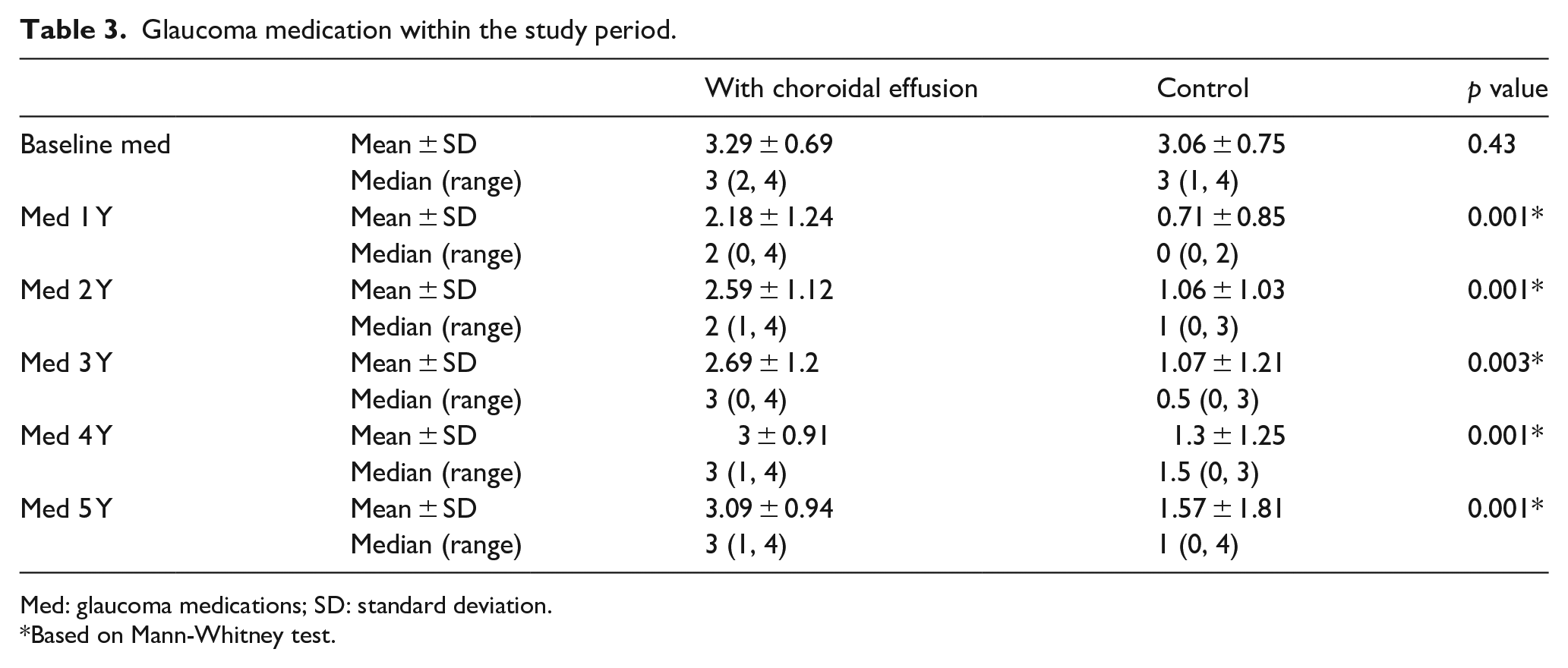
Med: glaucoma medications; SD: standard deviation.
Based on Mann-Whitney test.
The mean intraocular pressure (IOP) on the first day of choroidal detachment was 2.8 ± 3.7 mmHg. The mean period between surgery and occurrence of choroidal detachment was 1.73 ± 0.8 days.
In the case group, flat anterior chamber grade II was present in two patients managed by the AC reformation. Choroidal drainage was carried out in three patients who had kissing choroidal detachment in the operating room at a distance of 2–5 mm from the maximum place where fluid accumulation choroidal tap was carried out, sclera was punched and sclerectomy was made. All other choroidal detachments were resolved within 1 month of development. No complication occurred in the control group.
Discussion
Our results indicate that the presence of serous choroidal effusion leads to lower success rates, especially when target pressure is the IOP lower than 16 mmHg. The lower success rate was observed regardless of management of choroidal effusion. The control group with a final higher success rate was exactly matched for the known risk factors of age, sex, glaucoma type, and systemic diseases, including HTN and DM. Furthermore, risk factors such as glaucoma duration, preoperative IOP, and surgeon groups were comparable between the two study groups.
Choroidal detachment with the incidence rate from 7.7% to 18.9% after trabeculectomy, is a common early-onset complication. 4 The underlying pathophysiology is associated with the reduction of IOP during a short interval. The difference in the transmural pressure between choroidal capillaries leads to the exit of fluid from these vessels and its accumulation in suprachoroidal space. 2 Systemic HTN, tachycardia, older age, and higher baseline IOP are among the known risk factors of this condition. All of them are associated with the difference in the pressure inside and outside capillaries. 15
To the best of our knowledge, this is the first study reporting the long-term effect of choroidal detachment on the surgical success of trabeculectomy. The incidence of postoperative serous choroidal detachment in our study was similar to those of previous reports.8,16 In collaborative initial glaucoma study, choroidal effusion was diagnosed in 52 (11%) of 456 patients who underwent trabeculectomy. 8 Accordingly, in the tube versus trabeculectomy study, 14 (13%) of 105 patients developed serous choroidal detachment.9,10 The management protocol of the serous choroidal effusion in our center was the same as the one in the reported studies starting with the medical management, AC reformation in patients with flat AC grade 2, and choroidal drainage in patients with kissing choroidal detachment, or non-responsive to the medical management. 17
Benson et al. 14 investigated the presence of hypotony within the first month after the surgery as a risk factor for the failure in a case-control study and concluded that survival time was shorter in these patients after 5 years. The presence of choroidal detachment was included in the hypotony group. However, the direct effect of choroidal detachment was not investigated. Various studies reported the effect of hypotony on increasing postoperative inflammation that eventually could result in surgical failure.7,14,18 We postulate that hypotony may be a surrogate variable secondary to choroidal detachment that affects surgical failure. Since various etiologies could result in hypotony, we aimed to investigate the effect of choroidal detachment alone.
Multiple mechanisms can explain the lower long-term success found in our study. First, the success definition used in the present study emphasized further lowering of the IOP. Additionally, the other definition (<22 mmHg) found no significant difference between cases and controls. This result implies that choroidal detachment inhibits the achievement of lower IOPs, which is essential in trabeculectomy, especially in patients with advanced glaucoma. Furthermore, management of choroidal detachment may lead to higher IOPs. Medical management of choroidal detachment in patients with bleb overfiltration includes reduction of topical steroids in the most critical period of inflammation. 19 The subtle fibrosis formation reducing overfiltration may eventually lead to higher IOPs achieved in the long term. 20 Office-based procedures, including AC reformation with viscoelastic agents may also deteriorate the bleb function with mechanical pressure. Shu and Lovicu 21 indicated that mechanical pressure to the bleb induces Tenon’s capsule fibroblasts and leads to fibrosis formation. Finally, the surgical drainage of choroidal effusion can lead to increased inflammation, thereby reducing bleb functionality.
There are various measures to prevent choroidal detachment. Discontinuation of the anticoagulation drugs, control of blood pressure, and reducing the high IOP using hyperosmotic agents are among the preoperative measures to reduce the risk factors. Intraoperatively, creation of anterior sclerotomy in high risk patients, thicker flaps, prevention of IOP fluctuations, and good hemostasis might prevent the choroidal detachment. Postoperatively, avoidance of Valsalva-like maneuvers should be discussed with the patients. Topical and systemic aqueous suppressants might also play a role in choroidal effusion and it is better to avoid them in postoperative period and in the fellow eye, either.15,17
Retrospective design and small sample size are among the limitations of the present study. Another limitation was that matching was carried out for some variables except the surgeon’s experience, glaucoma duration, duration and number of glaucoma medications, and the refractive error which could affect our results. Considering refractive error, both hyperopia and myopia could play role in the occurrence of choroidal detachment. Moreover, the lack of visual acuity outcomes was one of the main limitations of the present study. A large amount of missing data on patients’ records and variability in visual acuity assessment in each visit caused us to omit the essential data.
In conclusion, our study suggests that the presence of choroidal detachment can affect both short-term and long-term success of trabeculectomy. This possibility should be considered in the management of patients with advanced glaucoma needing lower IOPs. It is recommended that preventive measures such as good control of perioperative IOP to avoid a large difference in IOP, meticulous closure of the wound to avoid hypotony, control of systemic hypertension, and tachycardia be taken to prevent the long-term failure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.