
Abstract
Purpose:
To compare lateral rectus recession (LRc) and medial rectus advancement (MRadv) for correction of consecutive exotropia (CXT).
Methods:
Of the 43 exotropic patients 20 of them underwent LRc (group 1) and 23 of them underwent MRadv (group 2). Postoperative exodrift, strabismic angle, dose effect relationship were compared with minimum 2 years follow‑up.
Results:
An average dose-effect in group 2 is higher than group 1 in the early postoperative period, however there was no significant difference at the second year follow-up (p=0,109). An average exodrift after 2 year follow-up was 6,6±7,12 PD in group 1, and 8,13±7,45 PD in group 2. Postoperative overall success rate was 50% in group 1 and 65% in group 2 at the last follow-up. The success rates were not significantly different between the groups (chi-square, p =0.31).
Conclusion:
Although there was no statistically significant difference at the last follow-up, better results were obtained with MRadv than LRc in the treatment of CXT.
Keywords
Introduction
Consecutive exotropia (CXT) is a common complication that occurs early or late after esotropia surgery. When non-surgical methods (botulinum toxin injection, prismatic glasses, alternating occlusion, and optical therapy) are ineffective, surgical approaches should be considered.1,2 The most preferred surgery for esotropia is bilateral medial rectus recession (BMRc).3,4 Age, accommodation, muscle slippage (disinserted and retracted rectus muscle within its capsule and reattachment to the sclera by an empty tendon sheath) and stretched scar formation are effective factors in the development of CXT.5–7 The slipped muscle creates a varying degree of adduction limitation, while a stretch scar is rarely associated with adduction limitation. 6
Various surgical approaches are used to correct CXT, including medial rectus advancement (MRadv) (with or without resection), lateral rectus recession (LRc), and a combination of these methods. Esotropia is generally preferred in the early postoperative period since there is a risk of exodrift over time.8,9 On the other hand, there is no consensus on the amount of esotropia to be targeted in the postoperative period. This is why it is important to compare surgical methods especially involving long-term results.1,10–12 To the best of our knowledge, no previous study has compared the long-term outcomes of MRadv and LRc in the treatment of CXT. Therefore, we aimed to report the dose-effect relationship of surgery and results in CXT patients.
Materials and methods
Subjects
This retrospective cohort study was carried out in accordance with the principles of the Declaration of Helsinki after obtaining the approval of the local ethics committee. The medical records of patients who underwent BMRc without lateral rectus resection for childhood esotropia between January 1994 and April 2018 were reviewed. The indication for CXT surgery was exotropia ⩾12 prism diopters (PD). Pre- and post-operative data collection and analysis included age (initial surgery for esotropia and CXT), gender, amount of previous BMRc, pre- and post-operative ocular alignment, presence of muscle slippage or stretch scar, adduction deficit, inferior oblique (IO) overaction, hypertropia, A or V pattern without dissociated vertical deviation (DVD), best-corrected visual acuity (BCVA), cycloplegic refraction, anisometropia, presence of amblyopia, biomicroscopy, and fundus examination.
Inclusion and exclusion criteria
According to the type of surgery, we divided patients into two groups: Group 1 consisted of patients who underwent only LRc (unilateral or bilateral) and group 2 who only had MRadv (unilateral or bilateral). Any patient with IO overaction greater than
Preoperative management and examinations
The angle of deviation was measured using the alternate prism cover test at near (30 cm) and distant (6 m) fixation with spectacle correction in primary gaze and gaze-up/down positions. The Krimsky method was used for uncooperative cases. The absence of a central, steady, maintained fixation, a BCVA value of <0.6 or an interocular BCVA difference of >2 lines (tumbling “E” or Snellen chart) were defined as amblyopia.2,13 In patients aged under 10 years, occlusion therapy was implemented before surgery until no further improvement was observed for three consecutive months. Anisometropia was defined as an interocular difference in the spherical equivalent of at least 1.00 D. The degree of duction deficit was graded on a scale of −4 to 0, with −4 indicating no adduction beyond midline, −3 indicating 75% adduction deficit, −2 indicating 50% adduction deficit, −1 indicating 25% adduction deficit, and 0 indicating full adduction. 14 Stereoacuity was evaluated with the Titmus stereotest (Stereo Optical, Chicago, IL, USA).
Surgical procedures and outcomes
All patients underwent either MRadv (unilateral or bilateral) or LRc (unilateral or bilateral). The forced duction test (FDT) was performed under general anesthesia before starting the operation. If adduction limitation was evident and no limitation was determined with FDT, MRadv (without resection) was performed. If no adduction limitation was preoperatively or the lateral rectus muscle was tight during FDT, single or bilateral LRc was performed depending on the angle of strabismus. Unilateral LRc was performed preferably on the non-fixating eye. All surgical operations were undertaken with a fornix-based incision with two double-armed 6.0 polyglactin 910 (Vicryl; Ethicon, Inc, Somerville, NJ) sutures using halfwidth, partial thickness bites, followed by two quarter-width and then third-width, full-thickness reverse locking bites at each edge with the non-adjustable technique. In the presence of a stretch scar, resection was performed as described by Ludwig and Chow. 6 Success was defined as deviation within 10 PD of orthophoria. 1 Overcorrection was defined as esotropia >10 PD, and undercorrection as exotropia >10 PD. 9 The postoperative angle of deviations were measured at the first week, sixth week, sixth months, and every 6 months thereafter. Surgical outcomes at the sixth week and second year after MRadv or LRc were analyzed for the study.
Statistical analysis
Statistical analysis was performed using Student’s t-test and Pearson’s chi-squared test with SPSS, version 16 (SPSS Inc., Chicago, IL, USA). Values of p < 0.05 were considered to indicate statistical significance
Results
The records of 64 patients diagnosed with CXT were reviewed, of which 43 met the inclusion criteria. Twenty-one patients were excluded for the following reasons; seven did not have complete follow-up data, six had undergone combined surgery (LRc+ MRadv), two had undergone adjustable surgery, three had missing data, and three had a neurological disease. There were 20 (10 male/10 female) patients in group 1 and 23 (11 male/12 female) patients in group 2. The mean age of the patients was 25.30 ± 7.45 years. While 21 patients were initially operated elsewhere, 22 patients had their first surgery in our hospital. Of the 43 cases, 28 (65%) had infantile esotropia, nine (21%) had partially accommodative esotropia, and six (14%) were classified as unknown type (no available records of childhood esotropia). Bilateral surgery was performed in four patients in each group. In group 1, 16 patients underwent unilateral LRc, and in group 2, 19 patients underwent unilateral MRadv. The average amount of LRc was 6.17 ± 0.94 (range: 5–8) millimeter (mm) in group 1 and the average amount of MRadv was 5.2 ± 0.49 (range: 4–6) mm in group 2. The mean age at initial surgery was 3.12 ± 2.01 years, and the mean age at surgery for CXT was 12.26 ± 9.61 years. Forty-one patients (95%) had basic exotropia (distance and near deviation within 10 PD), two (5%) had exotropia with convergence insufficiency (near deviation exceeding distance deviation by 10 PD). Table 1 summarizes the demographic and clinical data of the patients.
Demographic and clinical data of patients.
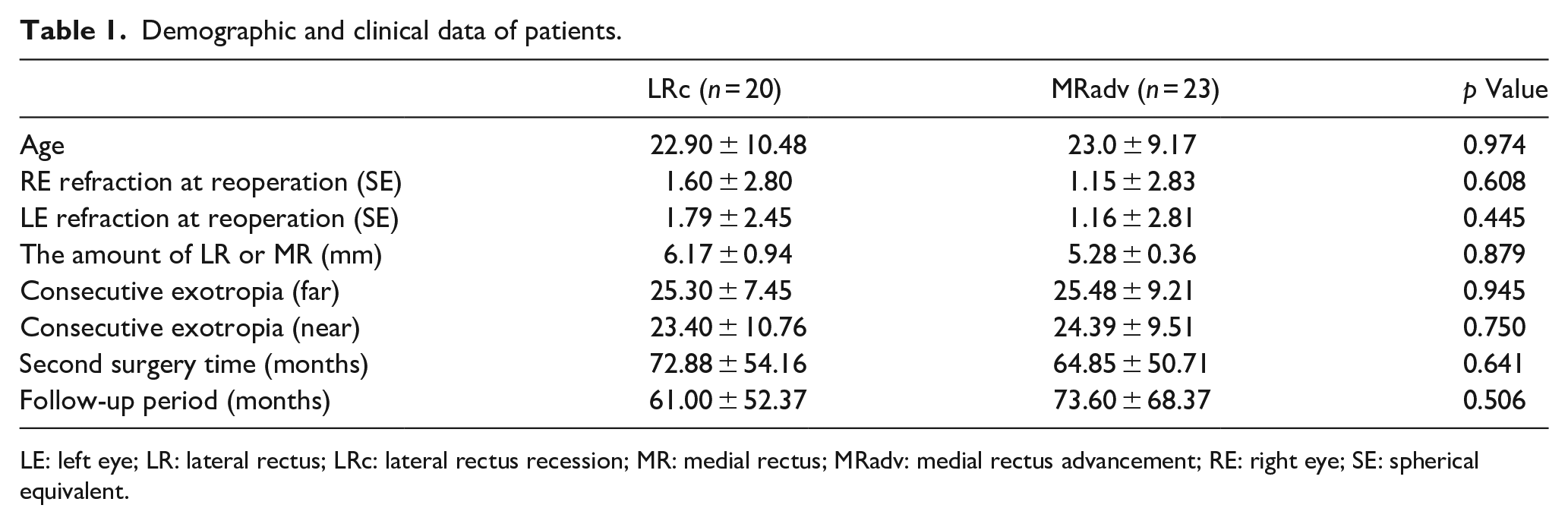
LE: left eye; LR: lateral rectus; LRc: lateral rectus recession; MR: medial rectus; MRadv: medial rectus advancement; RE: right eye; SE: spherical equivalent.
The average deviation corrected per mm of LRc was 2.48 ± 1.12 PD at the sixth week and 2.13 ± 1.22 PD in the second year. The average deviation corrected per mm of MRadv was 3.70 ± 1.27 PD at the sixth week and 2.80 ± 1.39 PD at the second year. The effect of advancing medial rectus was more than LRc at the sixth week follow-up (p = 0.002), but there was no statistically significant difference between the two groups for the second year follow-up (p = 0.109). In group 1, the mean preoperative exotropia was 25.30 ± 7.45 PD and 23.40 ± 10.76 PD at distance and near fixations, respectively. In the same group, the mean postoperative exotropia was 8.15 ± 7.50 PD at distance fixation and 6.25 ± 7.07 PD at near fixation, and the mean postoperative esotropia/phoria was 0.90 ± 0.62 PD and 1.20 ± 0.65 PD, respectively at the latest follow-up (61.00 ± 52.37 months). In group 2, the mean preoperative exotropia was 25.48 ± 9.21 PD and 24.39 ± 9.51 PD at distance and near fixations, respectively. In the same group, the mean postoperative exotropia was 7.39 ± 2.07 PD at distance and 7.43 ± 1.98 PD at near fixation, and the mean postoperative esotropia/phoria was 2.21 ± 1.05 PD and 1.60 ± 0.82 PD, respectively at the latest follow-up (73.60 ± 68.37 months). The average exodrift was 3.1 ± 4.70 PD in group 1 and 2.50 ± 2.98 PD in group 2 at the sixth week (p = 0.621). The average exodrift was 6.6 ± 7.12 in group 1 and 8.13 ± 7.45 in group 2 at the second year (p = 0.447). Ocular alignments measured at the sixth week, sixth month, first year and second year after CXT surgery are given in Table 2. While alignment remained within 10 PD of orthotropia in 63% (27/43) of patients, five out of 16 (37%) patients who did not benefit from surgery were re-operated. The overall postoperative success rate was 55% (11/20) in group 1 and 70% (16/23) in group 2 at the second year. There was no statistically significant difference in terms of surgical success between the groups (p = 0.32). In comparison, no statistically significant difference was found between the two groups in terms of age, gender, preoperative angle of deviation, refractive error, stereopsis, IO overaction, amblyopia, hypertropia, A- or V- pattern and follow-up time, (p > 0.05). Amblyopia was present in 10 (23%) patients, two of them were in group 1 and eight were in group 2 (p = 0.081). There was no statistically significant difference in terms of surgical success between the patients with and without amblyopia (p = 0.939). Five (12%) patients had hypermetropia >2.50 D, four (9%) patients had hypermetropia <2.50 D and three (7%) of these patients also had anisometropia. These patients were operated according to the angle of deviation with spectacles. While adduction limitation was present in a total of 15 (35%) patients before surgery, −1 adduction limitation was detected in only two (5%) patients postoperatively in group 2 at the last follow-up. The data of stereopsis before and after BMRc were incomplete. Of the 25 patients who were able to undergo stereopsis testing before CXT surgery, 30% (6/20) of patients in group 1 and 39% (9/23) of patients in group 2 had gross stereopsis (3000 s/arc) (p = 0.531). Postoperative gross stereopsis was achieved in 45% (9/20) patients in group 1 and 48% (11/23) patients in group 2.
Angle of deviations at 6 week, 6 month, 1 year, and 2 year after CXT surgery.
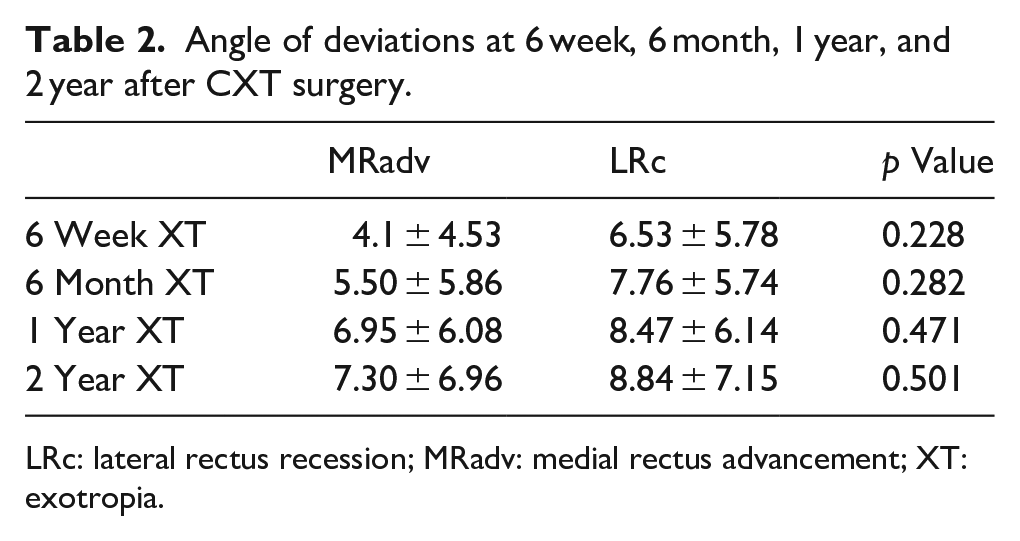
LRc: lateral rectus recession; MRadv: medial rectus advancement; XT: exotropia.
Discussion
It has been reported that CXT may develop at a rate of 3% to 31% in the long term follow-up.11–13 Unlike other studies, we investigated patients who underwent MRadv or LRc surgery after BMRc at a minimum of 2 years follow-up.1,2,15 LRc is generally used in basic or divergence excess exotropia where medial rectus function is normal.2,9 Cooper 13 suggested weakening the intact lateral rectus instead of performing a second surgery on the medial rectus. The success rate in Patel et al.’s 4 study where they applied bilateral LRc on CXT with an average follow-up of 30 months was 65%. Donaldson et al. 9 reported 86% success in patients who underwent LRc with a mean follow-up of 16 months. In the present study, 55% success rate in group 1 was lower than the previous two studies. On the other hand, the follow-up period was longer in our patients compared to the study by Donaldson et al. Gesite-de Leon and Demer 10 reported the success rate as 50% in different types of esotropic patients who underwent MRadv for CXT at the last follow-up (1.6 ± 1.8 years). Cho and Ryu 16 reported 79.2% success rate after MRadv (unilateral or bilateral) for CXT treatment at a minimum follow-up of 3 years. In the current study, the success rate of group 2 (69%) was lower than the study of Cho and Ryu 16 and higher than that of Gesite-de Leon and Demer 10 . The lower success rate of our study compared to the study of Cho and Ryu 16 may be related to the lower number of patients who underwent bilateral surgery. Mohan et al. 17 reported 91% success in a follow-up period of less than 2 years, but noted that this rate decreased to 52% when the follow-up period was longer than 2 years. Additionally, Rajavi et al. 18 reported that esotropia etiology did not show any relationship with the success or failure of CXT surgery. In previous studies, controversial results were obtained from various surgical methods, including combined procedures in the treatment of CXT.1,8,9,17–19 In this paper, long-term results of unilateral or bilateral surgery on the same muscle are discussed excluding the results of combined methods. On the other hand, there are studies targeting different amounts (5–15 PD) of esotropia for the postoperative period.9,10,20 Therefore, the long-term results of the studies in CXT are indispensable.1,9,19,20 In several studies, an average of 4 to 10 PD exodrift was reported in the early postoperative period (4–8 weeks) including MRadv + LRc.1,8–10 Similarly, an average of 4.1 PD exodrift was reported with a single MRadv in the early postoperative period by Tinley et al. 21 In the current study, an average of 3.1 ± 4.70 PD exodrift was detected in group 1 and 2.5 ± 2.98 PD exodrift was detected in group 2 at the sixth week, which were consistent with previous studies. In a study by Cho and Ryu 16 an average of 8.6 to 9.3 PD exodrift was reported after MRadv (50.6% unilateral/49.4% bilateral) in the long term follow-up (12–47 months). Different from the other studies, an average of 17 PD exodrift was reported after MRadv (90% bilateral, 10% unilateral) in the long term follow-up (1.6 ± 1.8-years) by Gesite-de Leon and Demer. 10 In the current study, an average of 8.13 ± 7.45 PD exodrift in group 2 and 6.6 ± 7.12 PD exodrift in group 1 was observed at the second year follow-up which were consistent with previous studies.
Another important point is that it is difficult to predict the dose effect of MRadv and LRc. An average of 3 to 5 PD/mm dose-effect has been reported by multiple authors for the correction of CXT including combined procedures.1,18,22,23 Lee et al. 1 reported the effectiveness of LRc to be 2.4 ± 0.5 PD/mm and MRadv to be 3.6 ± 1.4 PD/mm in the first postoperative month. Rajavi et al. 18 reported that each 1 mm of LRc and MRadv (with resection) corrected 2.20 ± 0.92 PD, 4.25 ± 2.27 PD over a 3-months follow-up, respectively. In the present study, each 1 mm surgery provided a correction of 2.48 ± 1.12 PD in group 1 and 3.70 ± 1.27 PD in group 2 at sixth weeks of follow-up. Our results at early follow-up were similar to those of Lee et al. 1 The results for group 2 can be considered as poorer if we do not take into account MRadv applied with resection in the series of Rajavi et al. 18 Cho and Ryu 16 reported that each 1 mm of MRadv corrected 3.2 ± 1.17 PD at the end of the 2-year follow-up. In our study, at the end of a 2-year follow-up, each 1 mm of surgery corrected 2.13 ± 1.22 PD in group 1 and 2.80 ± 1.39 PD in group 2. Compared to the study of Cho and Ryu 16 the correction of MRadv per 1 mm was lower in our study. Although the two studies have the same follow-up duration, the study groups differ in terms of first surgical procedure, since Cho and Ryu 16 evaluated patients with or without LRc in addition to BMRc.
The mean preoperative exotropia at distance and near fixations were 25.30 ± 7.45 PD and 23.40 ± 10.76 PD, respectively for group 1, and 25.48 ± 9.21 PD and 24.39 ± 9.51 PD, respectively for group 2. These results are consistent with the average values of previous studies.9,16,21 Medial rectus slippage was reported in 22% to 36% of patients with CXT.10,16 We did not detect muscle slippage in the present study, however we observed stretch scar formation in two (5%) patients. Donaldson et al. 9 did not find any difference between amblyopic (20.3%) and non-amblyopic (79.7%) patients in terms of surgical results. In our study, amblyopia was present in 10 (23%) patients. Similar to the study of Donaldson et al., we found no statistically significant difference in terms of surgical success between the amblyopic and non-amblyopic patients (p = 0.939). Previous studies reported 69% to 100% improvement in adduction limitation following MRadv.10,16,20,22,24 In the current study, adduction limitation was improved in 13 (87%) patients after CXT surgery consistent with the literature. However, −1 adduction limitation remained in two (13%) patients in group 2 at the last follow-up. In this study, the rate of gross stereopsis was 45% in group 1 and 48% in group 2, which was higher than reported by Lee et al. 1 (21.6%) in terms of same follow-up period. We consider that the higher rate of stereopsis among our patients may be related to the higher number of patients with partially accommodative esotropic (21%) patients compared to the Lee et al. 1 (13.5%) study.
This study has some limitations. First, it had a retrospective design. Second, simultaneous prism cover test, which is thought to be particularly useful in patients with accommodative esotropia and the monofixation syndrome was not used in the study. 25 Third, the data of stereopsis both preoperatively and postoperatively were not available for all cases. Fourth, since the same muscle surgery was applied to all patients, the structural changes and unfavorable insertions of unoperated rectus muscles could not be examined; thus, the rates of muscle slippage and stretched scar formation were limited. Finally, as recommended by Ludwig and Chow, 6 the use of non-absorbable sutures could have improved the success rate in the present study.
In conclusion, MRadv and LRc are effective procedures to correct CXT. In this study, an average dose-effect per mm was higher in group 2 than group 1 in the early postoperative period; however, there was no significant difference in the second-year follow-up (p = 0.109). Although the surgical doses of MRadv were not presented in tables, MRadv seemed to be more effective for the surgical treatment of CXT with respect to LRc and should be preferred in cases with adduction limitation, while LRc should be considered in recurrent cases of CXT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.