
Abstract
Purpose:
To evaluate the efficacy of Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT) in differentiating between optic nerve head drusen (ONHD) and optic disc oedema (ODE).
Methods:
This was a cross-sectional study of 140 patients: 83 patients with ONHD (49 hidden and 34 visible), 20 patients with pseudopapilloedema (without drusen), and 37 patients with ODE. EDI-OCT of the optic nerve was performed, selecting one high-resolution line from the HD 5-line raster protocol. Two observers blindly evaluated the presence of a hyporeflective core surrounded by a hyperreflective margin or border. The sensitivity, specificity, predictive values and posttest probability were evaluated as well as the inter-observer agreement (k).
Results:
EDI-OCT demonstrated a sensitivity of 92% (95% CI: 83%–96%), a specificity of 96% (95% CI: 87%–99%), with a positive predictive value of 97% and a negative predictive value of 89%. The inter-observer agreement was as remarkable as k = 0.8985 (95% CI 0.8252–0.9718). A positive EDI OCT increases the posttest probability to 97% (95% CI: 91%–99%); when negative, the posttest probability is reduced to 12% (95% CI: 6%–21%).
Conclusion:
EDI-OCT allowed for differentiation between ONHD and ODE with high sensitivity and specificity.
Keywords
Introduction
Differentiation between optic disc oedema (ODE) and pseudopapilloedema due to optic nerve head drusen (ONHD) is important in our daily clinical practise. However, differential diagnosis can be difficult, especially in patients with buried drusen. Several diagnostic methods have been described for this purpose: fundus examination, 1 fluorescein angiography, 2 autofluorescence, 3 monochromatic filters, 4 SLO, 5 computerised axial tomography (CT) 6 and ultrasound scanning. 7
Optical coherence tomography (OCT) has been used to differentiate ONHD and ODE using time-domain OCT (TD-OCT) 8 and spectral domain OCT (SD-OCT).9,10 Moreover, the higher penetrance of recent OCT has allowed the identification of new signs to identify ONHD: hyporeflective core surrounded by a hyperreflective border.11–14
The objective of this study was to determine the validity of Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT) in differentiating ONHD from ODE. Therefore, we assessed sensitivity, specificity, and predictive values, in addition to the inter-observer concordance.
Methods
Approval was obtained from the Ethics Committee of the Alcorcon Foundation University Hospital (Spain) and the study was conducted complying with the principles of the Helsinki Declaration. Written informed consent was obtained from all participants.
A prospective, descriptive, transversal study was conducted, which included patients with ODE and pseudopapilloedema (with and without ONHD) during the period between January 2013 and December 2016 in the Ophthalmology unit of our hospital.
All patients included in our study underwent a complete ophthalmological examination, which included: measurement of best-corrected visual acuity, anterior segment examination, fundus examination under pharmacological mydriasis, colour photography, fundus autofluorescence of the optic disc using a mydriatic fundus camera with 20° (FF 450 plus IR; http://www.meditec.zeiss.com), B-scan ultrasound (OTI Ophthalmic Technologies Inc.; http://2774.ca.all.biz) and SD-OCT using a Cirrus OCT 4000 model (5.0.0 version; http://meditec.zeiss.com).
Inclusion criteria
Three groups of patients were included: patients with ONHD (visible and hidden), patients with pseudopapilloedema due to other causes, and patients with ODE. All patients were followed for at least 6 months.
(1) ONHD: Patients with visible and/or buried drusen, unilateral or bilateral, confirmed in all cases with a B-scan ultrasound with a gain of <27 dB.
(2) Pseudopapilloedema (without optic disc drusen), defined as anomalous blurring and/or elevation of one or both optic discs without oedema of the retinal fibre layer: tilted disc, myelinated nerve fibres, epipapillary glial tissue (Bergmeister’s papillae), small optic discs and other congenital anomalies were included. Patients with drusen were excluded from this group (excluded through B-scan ultrasound and fundus autofluorescence).
(3) Optic disc oedema (ODE): Patients with ODE of different aetiologies were included. They underwent a complete neurological and ophthalmological examination with definitive diagnosis of ODE. The papilloedema group included patients with emerging optic disc oedema and increased intracranial pressure (lumbar puncture opening pressure greater than 25 cm H2O).
Exclusion criteria
- Patients with a lack of collaboration for any of the tests, lack of follow-up over 6 months, doubtful or unconfirmed diagnosis, or absence of informed consent.
- Ocular pathologies (dense corneal leucomas, mature cataract, vitreous haemorrhages and any other opacity), posterior segment surgeries, or eye trauma.
- Diagnostic test: lack of any diagnostic test (fundus photography, OCT, B-scan ultrasound), fundus photography with low quality, fundus images of peri-papillary atrophy, or OCT image signals of less than 7.
Optical coherence tomography
One experienced operator conducted all OCT examinations. Only images with a signal quality index higher than 7 were included. OCT was performed during the acute phase of neuropathy in the ODE cases. In Cirrus OCT, measurements were made on the Optic Disc Cube 200 × 200 protocol and 5 Line HD raster using the EDI protocol. The operator performed a one-line HD raster where drusen were identified (guided by EDI-OCT 5 line HD raster) or on the more elevated area (guided by the fundus examination).
The characteristic presence of a rounded hyporeflective core surrounded by a hyperreflective margin was evaluated (Figure 1).
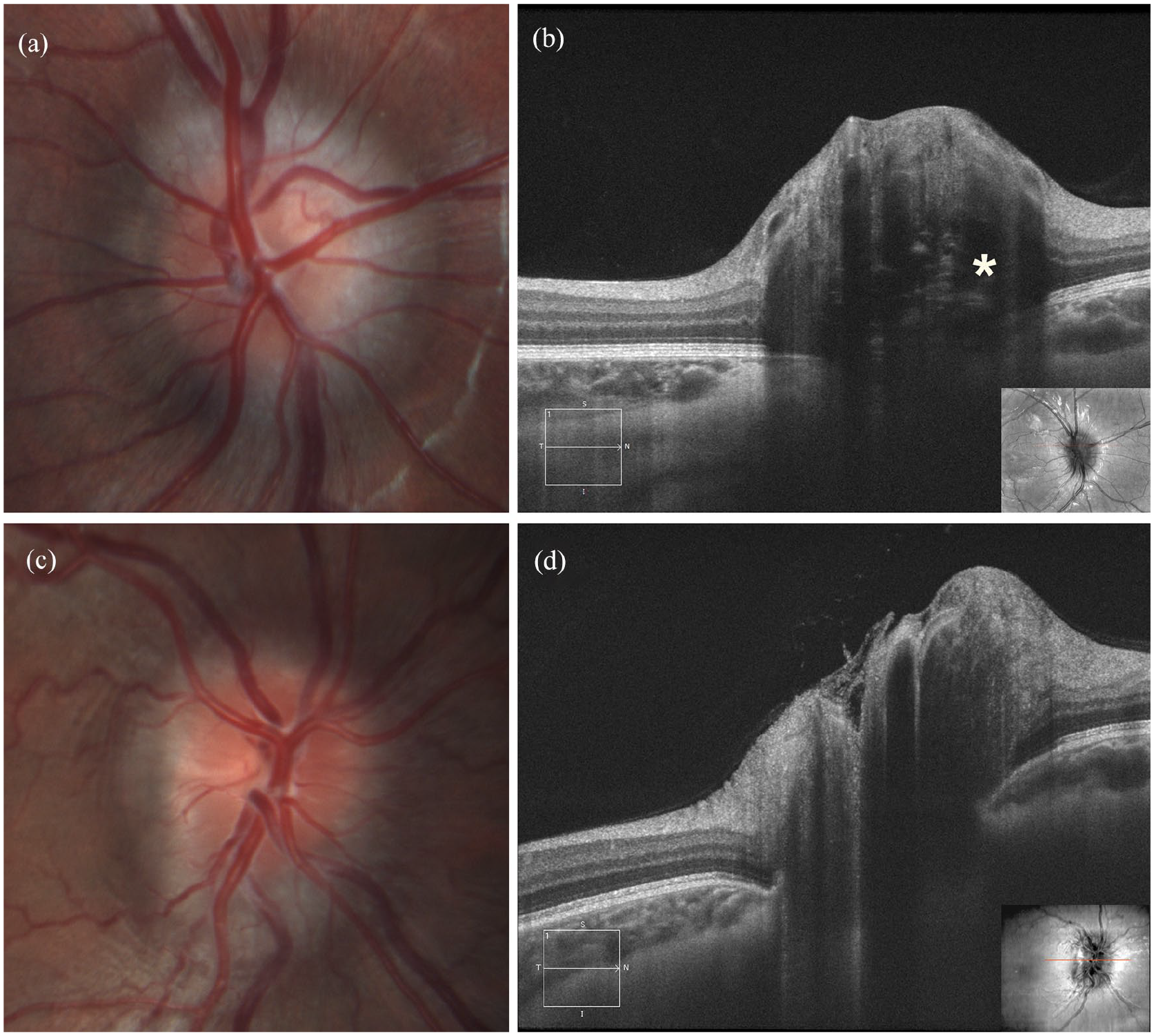
Hidden Optic nerve head drusen (ONHD): Fundus photography (a) and Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT) (b): hyporeflective intrapapillary structures surrounded by hyperreflective horizontal lines characteristic of ONHD (asterisks). Papilloedema (ODE): Fundus photography (c) and EDI-OCT (d): lack of hyporeflective intrapapillary structures surrounded by hyperreflective margin.
The OCT images were analysed afterwards by two masked observers to assess the presence or absence of these OCT signs.
Statistical analysis
From all patients with bilateral pathologies, one eye of each patient was randomly selected. In the descriptive analysis, the qualitative variables were expressed as frequencies, and the quantitative variables were expressed as mean and standard deviation (SD) or median and interquartile rank according to data distribution.
To study the differences between the two groups, qualitative variables were compared using the Chi square or Fisher’s exact test. Quantitative variables were compared with the Student’ s t-test for two independent samples or the Mann-Whitney U test in cases of non-normal distribution. For comparing three groups, ANOVA or Kruskal-Wallis test (in cases of non-normal distribution) were used.
The sensitivity and specificity with 95% confidence intervals, the positive predictive value (PPV), and negative predictive value (NPV) were analysed, considering B-scan ultrasound as the gold standard in ONDH diagnosis. The likelihood ratio (LR positive and LR negative) as well as the post-test probability (or adjusted positive predictive value) was also studied. LR+ near 10 and LR− near 0.1 are considered clinically relevant.
Kappa values were used to determine inter-observer reliability for categorical variables. Values of 0.81 to 1.0 are indicative of excellent agreement; 0.61 to 0.80 substantial agreement; 0.41 to 0.60 moderate agreement; 0.21 to 0.40 fair agreement; 0 to 0.20 slight agreement; and <0 poor agreement.
Statistical analyses were performed using the SPSS program for Windows (version 19.0.1; http://www.01.ibm.com/software/analytics/spss/) and MedCalc (version 7.3.0.1; http://www.medcalc.org/). All tests were two-tailed, and a significance level of 5% was established. Bonferroni correction was used to correct multiple comparisons, and p < 0.016 was considered to indicate a statistically significant difference.
Results
The study population included 140 eyes of 140 patients with a median age of 35 years (IQR 25–59), with a range between 5 and 89 years, and with a predominance of women (66, 61.4%). Eighty-three patients had ONHD (49 visible and 34 buried drusen), with a median age of 43 years (IQR 30–57) and 60.2% were women. Thirty-seven patients had ODE: 16 with papilloedema (12 with idiopathic intracranial hypertension, four with tumoural origin), nine with AION, three with neuritis, two with central retinal vein occlusions, and one with papillary oedema due to hypotony). The median age was 45 years (IQR 27–65) (67.6% women). Twenty patients had pseudopapilloedema without ONHD, with a median age of 18 years (IQR 6–33) (55% women) (Table 1).
Studied population characteristics.
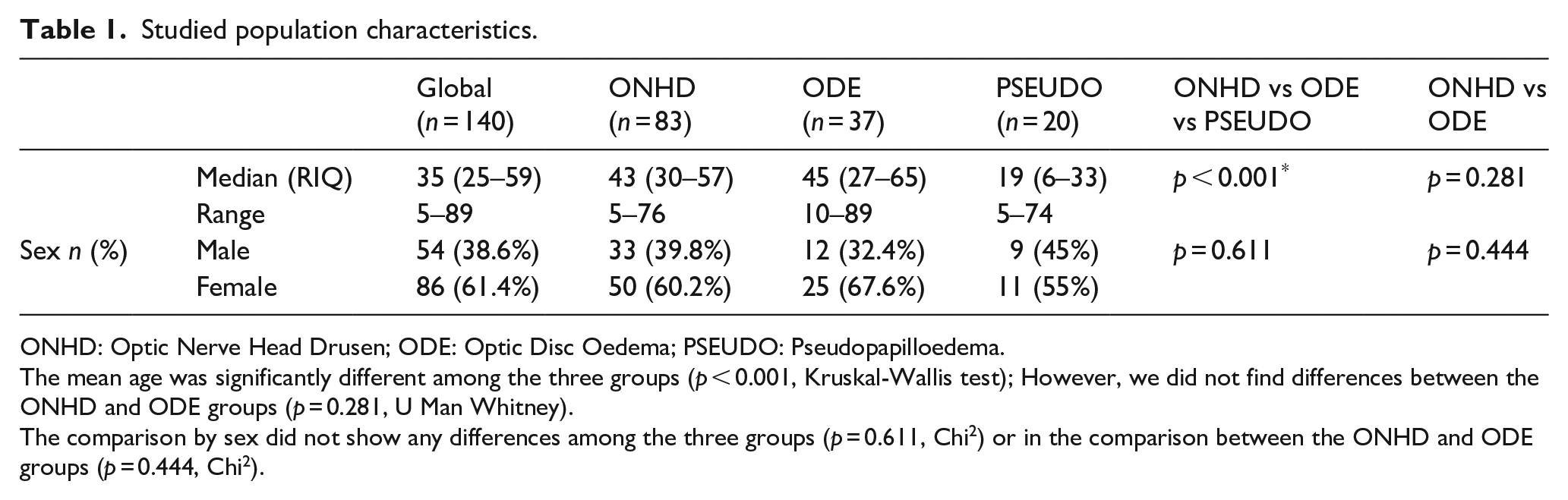
ONHD: Optic Nerve Head Drusen; ODE: Optic Disc Oedema; PSEUDO: Pseudopapilloedema.
The mean age was significantly different among the three groups (p < 0.001, Kruskal-Wallis test); However, we did not find differences between the ONHD and ODE groups (p = 0.281, U Man Whitney).
The comparison by sex did not show any differences among the three groups (p = 0.611, Chi2) or in the comparison between the ONHD and ODE groups (p = 0.444, Chi2).
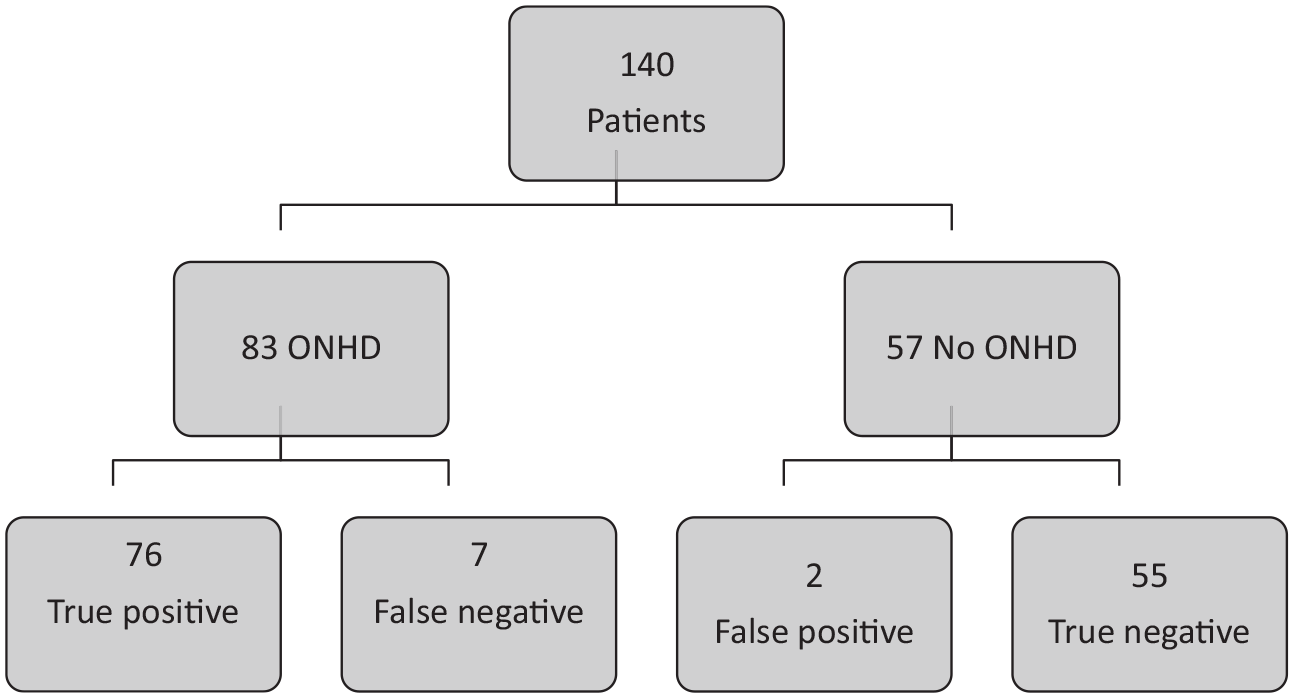
The presence of a hyporeflective core surrounded by a hyperreflective margin or border was analysed, and it was present in 76 of 83 patients with ONHD (92% true positive). Only 2 of 57 patients without ONHD were assessed as positive (4% false positive) (Figure 2).
Analysis of Enhanced Depth Imaging Optical Coherence Tomography diagnostic validity.
The analysis of OCT EDI diagnostic validity demonstrated a sensitivity of 92%, a specificity of 96%, a positive predictive value of 97%, and a negative predictive value of 89% (Table 2).
Sensitivity and specificity of Enhanced Depth Imaging Optical Coherence Tomography in optic nerve head drusen diagnosis.

Sn: sensitivity; Sp: specificity; PPV: Positive predictive value; NPV: Negative predictive value; LR+: Positive likelihood ratio; LR−: Negative likelihood ratio.
The ONHD prevalence (pre-test probability) in our study was 59% (95% CI: 51%–67%). The positive likelihood ratio (LR+) quotient was 26.10, and the negative likelihood ratio (LR−) quotient was 0.09. With a positive OCT EDI, the post-test probability increases to 97% (95% CI: 91%–99%). With a negative OCT EDI, the post-test probability decreases to 12% (95% CI: 6%–21%) (Figure 3).
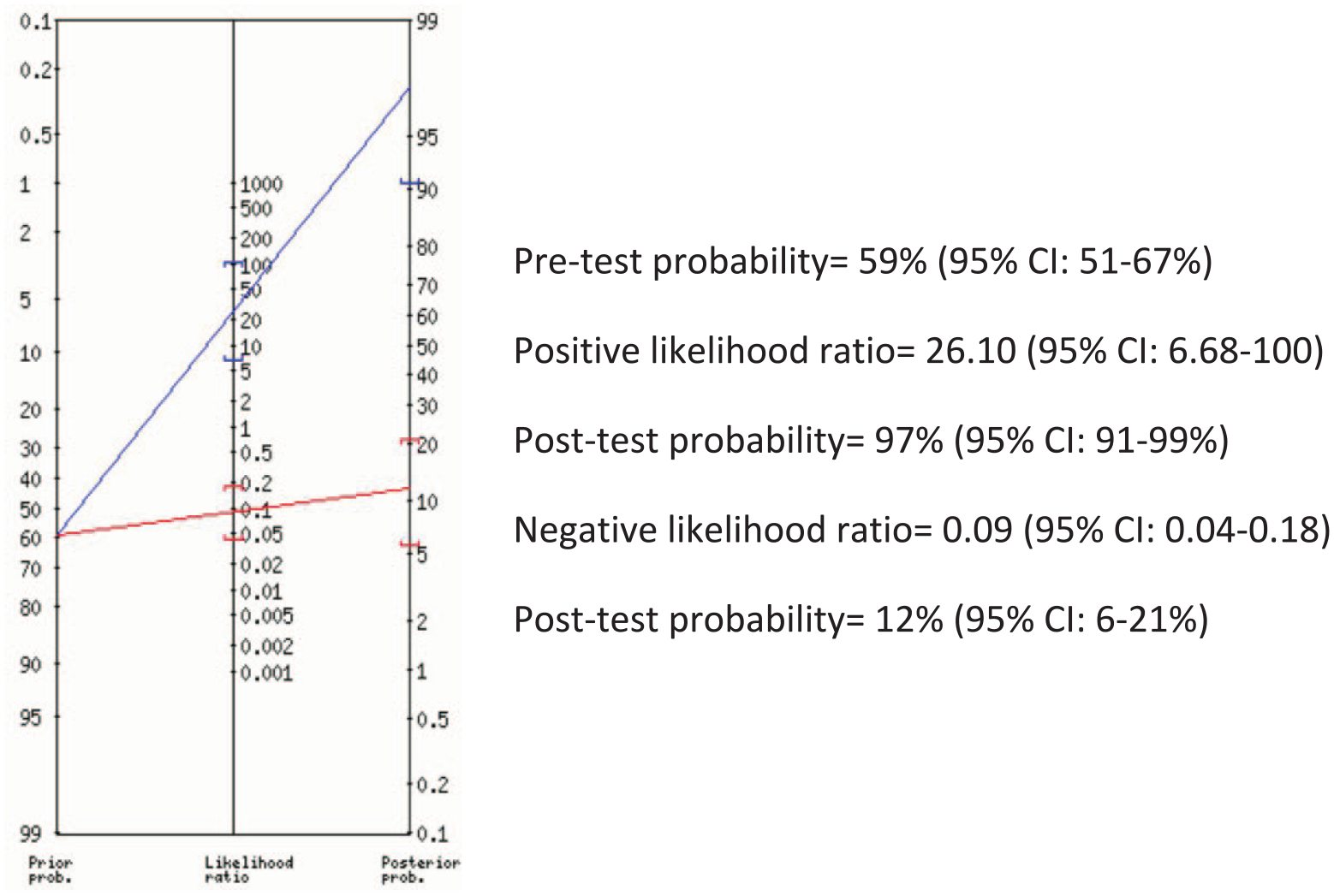
Fagan’s nomogram for optic nerve head drusen diagnosis with Enhanced Depth Imaging Optical Coherence Tomography.
The inter-observer agreement for OCT EDI image interpretation showed excellent values of k = 0.90 (95% CI: 0.83–0.97).
Discussion
Optic nerve head drusen (ONHD) are acellular calcified deposits. Their prevalence has been estimated to be between 3.4 and 24 per 1000 in population, 15 with a higher frequency among individuals of the Caucasian race and a slightly greater prevalence in women. 16 ONHD tends to be asymptomatic; nevertheless, visual field defects are frequent. Usually, they are diagnosed through an ordinary fundus examination, as elevated and blurry margins of the optic disc, mostly bilateral, and occasionally with visible calcifications. Different methods have been described for the diagnosis of ONHDs. The most commonly used techniques include fundus examination, 1 fluorescein angiography, 2 autofluorescence, 3 monochromatic filters, 4 SLO, 5 computerised axial tomography (CT), 6 ultrasound scanning 7 and, more recently, optical coherence tomography. To date, no studies have examined the sensitivity and specificity of all available modalities for the diagnosis of ONHD. 17 Fundus autofluorescence can identify nearly all visible drusen and many buried drusen.3,4 Computed tomography (CT) will show calcified ONHD; however, the usual 1.5 mm slices can reduce sensitivity, which leads to inability in detecting any non-calcified ONHD, and radiation exposure also limit the utility of CT. 17 In 2013, when patient enrolment for this study started, B-scan ultrasound was considered the ‘gold standard’ in the diagnosis of ONHD, with a greater sensitivity than CT scanning or autofluorescence. A highly echogenic focus at the optic disc that persists at low gain can confirm both visible and buried drusen, understood to represent calcification.17,18
The wide diffusion and continuous improvement of optical coherence tomography equipment has allowed us to better diagnose ONHD and to differentiate them from other entities. Different qualitative and quantitative criteria have been described regarding time-domain OCT and especially spectral domain OCT in the description of ONHD.10–23
The observation of a hyporeflective space, located between the neurosensorial retina and pigmented epithelium in ONHD, with an irregular contour and an abrupt decrease was described by Johnson et al., 8 as a differentiation criterion from the hyporeflective space found in papilloedema described by Savini et al. 23 This feature is quite characteristic, with a sensitivity of 88% and a specificity ranging from 80% to 89%. 10 Sarac et al. 19 reported a thickness of hyporeflective space >464 m with a sensitivity of 85% and specificity of 60% in ONHD diagnosis. This hyporeflective space is really an artefact due to the low penetrance of the first generations of OCT.17,22
Peripapillary hyperreflective ovoid mass-like structure (PHOMS) has been described in patients with ONHD. 9 Some authors have supported the theory that PHOMS represent a precursor or a variant of ONHD. 24 However, PHOMS should not be diagnosed as ONHD14,17,22 In fact, there is histopathological evidence that PHOMS are lateral bulges of retinal nerve fibres. 14
In contrast, Kulkarni et al. 25 concluded that the value of OCT in differentiating ONHD and mild papilloedema is low (between 50% and 64%) with a fair agreement (K = 0.35).
The retinal nerve fibre layer (RNFL) measurement in the ONHD is one of the most studied quantitative criteria. The average thickness of the RNFL is usually increased in buried ONHD, but it is higher in cases of papilloedema. Some authors have suggested a cut-off point <116 µm for ONHD, with high sensitivity (91%) and specificity (97%). 10 Other authors have described the usefulness of average RNFL thickness to differentiate optic disc oedema from pseudooedema (cut-off value of >110 µm, sensitivity 70%, specificity 76%). 26
The presence of at least 7 contiguous clock hours with significant thickening of the RNFL (which appears white) with Stratus OCT described as characteristic of papilloedema yielded high sensitivity (98%) but low specificity (77%). 10 One disadvantage of this criterion is that it cannot be analysed in many devices when age is inferior to 18 years, since normalised data does not exist.
The nasal RNFL thickness can be useful in differentiating both entities, which is greater in papilloedema. The selected cut-off point varies between authors and equipment: 108 µm for TD OCT 10 and from 75 to 92 micron for SD-OCT.11,19 Sarac et al. 19 reported excellent sensitivity (92%) but lower specificity (47%).
Flores-Rodríguez et al. 10 described papillary elevation measurement as a diagnostic criterion, being greater in papilloedema than in ONHD. This parameter had a sensitivity of 86% and a specificity of 87%, for a cut-off point <800 µ with SD-OCT.
Other authors have reported alterations in the ganglion cell layer (GCL), found in 30% of patients with buried drusen, as a more sensitive parameter than average RNFL measurement (4%). 27 Pilat et al. 28 describes differential characteristics of vascularisation in patients with ONHD, papilloedema, and controls; however, his study does not provide sensitivity and specificity values.
The high penetrance OCT, such as EDI-OCT (849 nm) and SS-OCT (1060 nm), has enabled the description of new findings in ONHD.11–14 The Optic Disc Drusen Studies Consortium reached a consensus to define ONHD as hyporeflective structures with a full or partial hyperreflective margin, most prominent superiorly (Figure 1). 14 This hyperreflective margin seems to be caused by the reflection and scattering of the OCT beam bouncing off the calcium surface of the ONHD.11,13 Isolated hyperreflective horizontal lines might represent early drusen but should not be diagnosed as ONHD. 14
In our study, we evaluated the presence of this sign (hyporeflective structures with a full or partial hyperreflective margin), with a sensitivity of 92% and specificity of 96%. It has, amongst the qualitative criteria described, higher diagnostic validity values. The positive and negative likelihood quotients allow us to calculate the post-test probability, regardless of the prevalence. In our case, a positive EDI-OCT practically confirms the existence of ONHD (post-test probability = 97%). Even though the evaluated parameter is a qualitative criterion, the excellent inter-observer agreement (k = 0.90) obtained in our study confirms that this parameter can be easily conducted. Some authors even suggest that higher penetrance OCT could be more sensible than ultrasound scanning in ONHD detection.11–14,17,22
The strengths of our study include the following: a wide sample size, inclusion of pseudopapilloedema cases, selection of only one eye per patient, and assessment of inter-observer agreement.
Several limitations could be considered in our study. In the first place would be the qualitative and subjective nature of this diagnostic feature. Secondly, the diversity of pathologies included in the optic disc oedema group. Moreover, the evaluation of one-line HD raster could not detect the presence of ONHD, especially buried ONHDs. Another limitation that should be taken into account is that, as B-scan ultrasound is considered the gold standard, small, non-calcified buried drusen could not be identified, and these patients might be mistakenly included in the pseudopapilloedema group.
Continuous improvement of technology in OCT equipment will provide faster scans of higher quality and with higher penetrance capacity. This will improve our ability to detect even smaller and deeper localised drusen. In future studies, the combination of various parameters, which will increase the sensitivity and specificity of OCT in ONHD diagnosis, should be considered.
In conclusion, high-penetrance OCT images provide a means to allow visualisation of ONHD as low-reflectivity round masses surrounded by a hyperreflective margin. The assessment of this sign enables the differentiation of ONHD from optic disc oedema, with high sensitivity and specificity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.