
Abstract
Purpose:
To report a case of macular choroidal osteoma treated with photodynamic therapy.
Observations:
A 34-years old woman with decreased visual acuity in her left eye came to our observation for assessment of an amelanotic choroidal tumor in the left eye. On the basis of ophthalmoscopic and echographic features the tumor was diagnosed as choroidal osteoma. Imaging examination revealed subretinal fluid involving the foveal area associated with alterations of outer neuroepithelial layers and photoreceptors without evidence of choroidal neovascularization. Foveal sparing standard fluence rate photodynamic therapy was performed. After treatment, subretinal fluid reabsorption and visual acuity recovery was noted with progressive restoration of foveal architecture. Due to the relapse of fluid and visual impairment, 1 year after treatment, a second PDT session was made using the same parameters and protocol of treatment. Despite a complete subretinal fluid reabsorption and visual acuity recovery the second treatment was complicated by the development of subretinal fibrosis.
Conclusions:
PDT is effective to induce subretinal fluid reabsorption and visual recovery in choroidal osteoma located in the macular area. However, the risk of possible complications related to the treatment have to be considered.
Introduction
Choroidal osteoma (CO), first described by Gass et al. in 1978, is a benign ossifying tumor affecting choroid composed by structured bone tissue. 1
The tumor is considered to be a rare condition affecting mostly young patients, usually in their second or third decades of life, with a 6:1 female to male ratio. 2 Although the tumor is often presented unilaterally, bilateral disease has been reported in 21% of patients. 3 In most cases choroidal osteoma is located at the posterior pole, often in the juxtapapillary or peripapillary region, appearing as an irregular elevated orange-red to yellowish-white lesion, depending on the grade of retinal pigment epithelium (RPE) depigmentation.
In most cases choroidal osteoma is asymptomatic with well preserved visual acuity, although some patients could complain blurred vision, metamorphopsia, photophobia, or visual fields defects due to different triggers: degeneration of the retinal pigment epithelium overlying the osteoma, serous retinal detachment associated to the lesion, decalcification of the tumor, growth of subretinal new vessels (CNV) which represents its most common complication. 4
To date, there is no standard treatment for CO, and all therapeutic options are mainly directed in treating secondary new vessels through laser therapy, photodynamic therapy (PDT), or anti-VEGF drugs.
We report a case of choroidal osteoma located in the macular region associated with serous foveal detachment, without CNV, treated with Photodynamic Therapy (PDT) sparing the foveal area.
Case report
A 34-years old Caucasian female with a 2 months history of blurred vision in the left eye (OS) was referred for evaluation and management of an amelanotic choroidal tumor in her left eye. She reported no other ophthalmologic disorders and her medical history was negative for surgeries, tumors or illnesses. At presentation, best corrected visual acuity (BVCA) was 20/20 in her right eye (OD) and 20/40 in her left eye (OS). The anterior segment examination was unremarkable in both eyes. Fundus examination was normal in the right eye, while in the left eye revealed a flat, white-yellowish amelanotic choroidal lesion, with fairly regular and well defined margins, involving the whole macular area. Ultrasonography showed a highly hyperechoic choroidal lesion with posterior shadowing, typical for calcification.
Spectral Domain Enhanced Depth Imaging Optical Coherence Tomography (EDI-OCT) (Spectralis HRA + OCT, Heidelberg Engineering, Heidelberg, Germany) revealed irregularities of outer retina with focal alterations of the outer plexiform layer and of the external limiting membrane. Mild elongation of the outer segment of photoreceptors was noted associated with subretinal fluid (SRF) involving the foveal area. The tumor displayed a low internal reflectivity giving minimal shadowing posterior to the lesion, with clear evidence of the external posterior limit of the choroid. Based on the clinical and instrumental features, the diagnosis of choroidal osteoma was made.
Fluorescein Angiography, Indocyanine green angiography (IGA) and OCT-Angiography (OCT-A) did not reveal signs of choroidal neovascularization (CNV) (Figure 1).
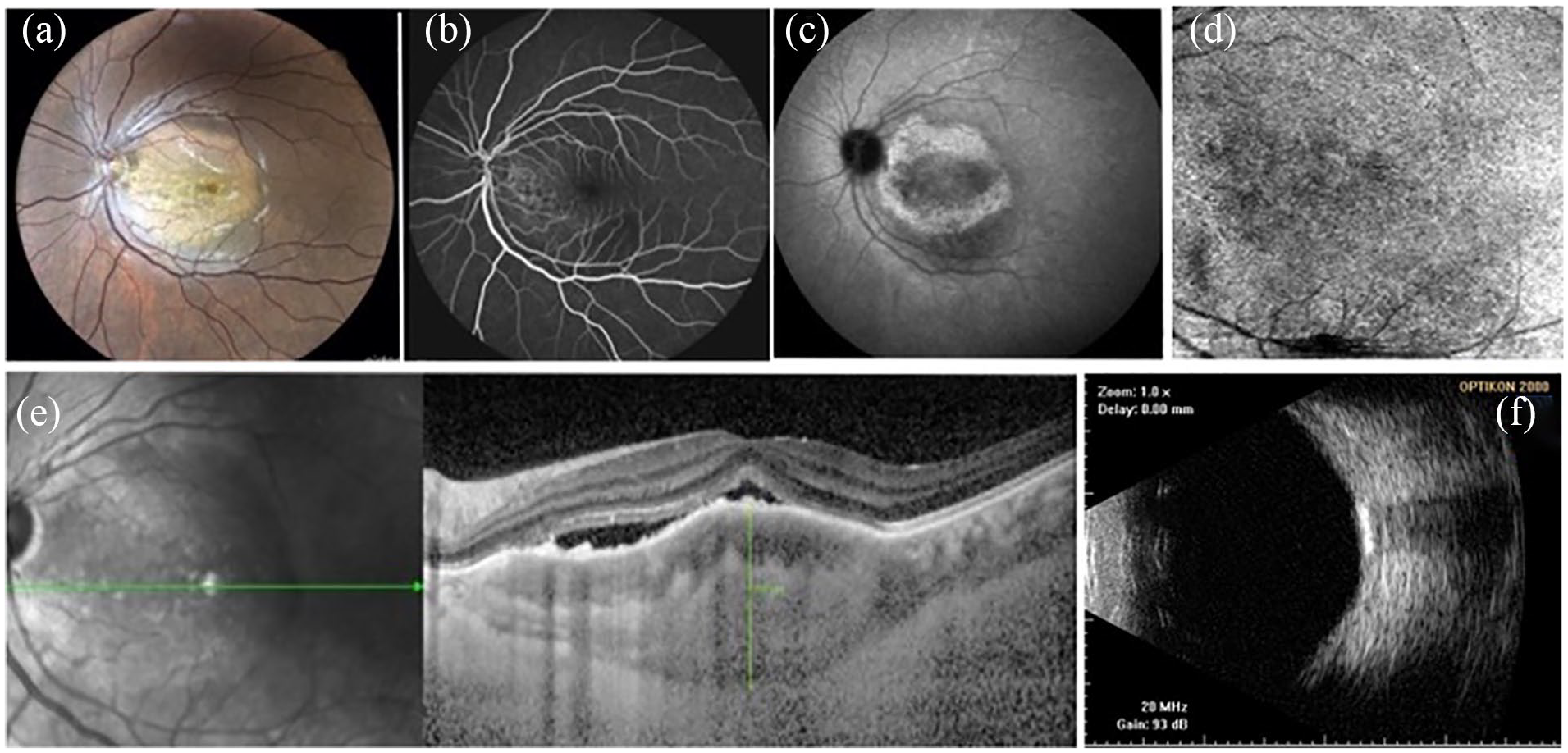
(a) Fundus photography of the left eye. Yellowish unilateral choroidal osteoma with well defined margins, located in the macular area. (b) Fluorescein angiography showed irregular fluorescence of the tumor without evidence of choroidal neovascularization. (c) Indocyanine green angiography: late ring of hyperfluorescence with external margins corresponding to the tumor shape. These characteristics have been interpreted as a staining phenomenon. (d) OCT angiography (image 6 × 6 mm): automated segmentation of Sub-RPE. No evidence of neovascular networks was depicted. (e) EDI-OCT scan showing the tumor low internal reflectivity with clear evidence of the external posterior limit of the choroid. The tumor thickness corresponded to 797 µm. (f) B-scan ultrasound showing a highly hyperechoic area with posterior shadowing.
Due to the absence of validated Guidelines for the treatment of SRF associated with CO and considering the reduction of visual acuity complained by the patient and the OCT findings suggesting a prolonged time of neuroepithelial elevation, a cycle of three monthly anti-VEGF drugs with Aflibercept (Bayer plc, Regeneron, Inc) was scheduled, assuming the possible role of VEGF in leading to tumor vessel exudation. However, due to the persistence of the same amount of subretinal fluid, which was interpreted as the absence of clinical response, the treatment was interrupted after the second injection. Three months after the second injection, photodynamic therapy (PDT) with verteporfin was then considered for treatment, with the aim of inducing a resolution of subretinal fluid and restoring the normal anatomy of the photoreceptors cells in the foveal area. The local ethic committee approved both Anti-VEGF and PDT off label treatment, and the patient signed specific consensus forms.
Verteporfin (Visudyne, Novartis Ophthalmics, Hettlingen, Switzerland) was infused intravenously in 10 min at a dose of 6 mg/m2 body surface area.
PDT was performed with a standard full fluence (689-nm diode laser, 600 mW/cm2 for 83 s with a radiant exposure of 50 J/cm2). Laser beam was directed to the retina soon after the end of infusion and multiple non overlapping spots were applied covering the whole area of the tumor except for the foveal and parafoveal areas, by ensuring that each laser spot would have been distanced from the external margin of the fovea approximately 500 µ.
One month after treatment visual acuity improved in the left eye to 20/32. OCT showed anatomic improvement of the external retina with almost complete resolution of subretinal fluid and evidence of multiple subretinal hyperreflective spots. Two months later, the patient presented a further visual improvement to 20/25. The OCT analysis of the neuroepithelium showed diffuse irregularities of the ellipsoid zone. At 6 months follow-up, the patient BCVA was recovered to 20/20 and this visual acuity remained stable at 9 months of follow-up. OCT detected during follow-up an improvement of the retina profile as well as a partial reconstitution of the ellipsoid zone and a complete disappearance of subretinal fluid.
EDI-OCT showed a progressive decrease in tumor thickness equal to 797, 645, 601, and 590 µm at 1, 3, 6, and 9 months of follow-up, respectively.
The tumor thickness was measured manually as the distance intercurring between the outer portion of the hyperreflective line of the EPR and the hyporeflective line corresponding to the sclerochoroidal interface. The measurements were performed at the fovea by two experienced retina specialists (A.S. and M.L.R.). No clear evidence of decalcification in the foveal area was noted during follow-up (Figure 2).
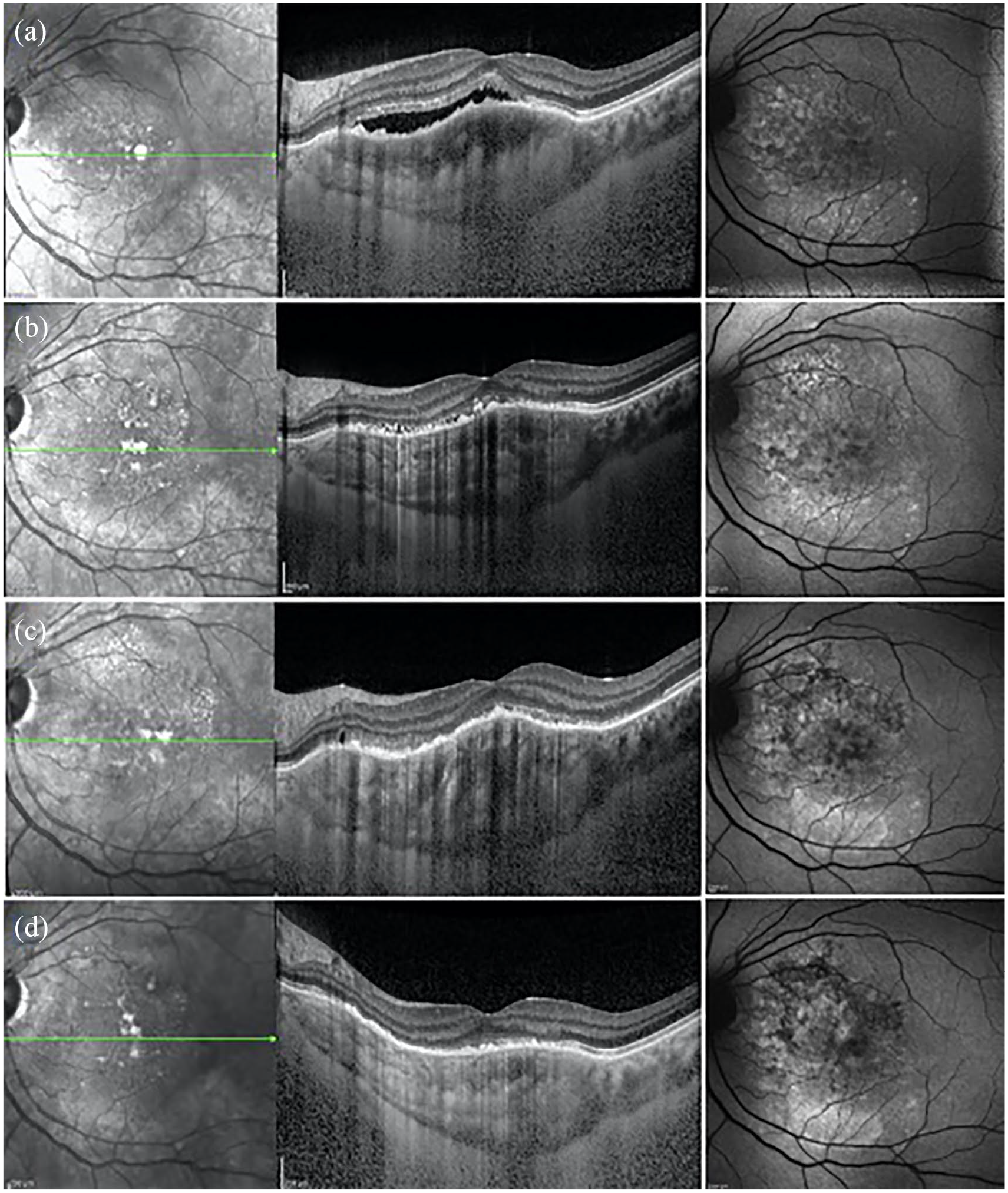
(a) EDI-OCT scan pre PDT treatment: serous subfoveal detachment of the neurosensory epithelium in the affected eye with lengthening of photoreceptor outer segment. (b) One month follow up: resolution of subretinal fluid with irregularities of ellipsoid zone with the presence of dot hyperreflective spots and posterior shadowing progressive improvement of the external retina and at 6 months (c) and 12 months (d) with complete resolution of SRF. During follow-up, progressive RPE atrophy was evident on FAF mostly in the extrafoveal superior part of the tumor as mottled autofluorescence areas.
At 1 year of follow-up, the patient complained a sudden visual acuity reduction in her left eye, with a BCVA dropped to 20/60. A serous subfoveal detachment of the neurosensory epithelium was found in the left eye on OCT examination and the absence of choroidal neovascularization was confirmed at the ICG Angiography. After a discussion with the patient about risks and benefits of retreatment, a second session of PDT treatment was then performed using the same parameters and protocol of treatment.
Soon after treatment the patient referred a central scotoma with decreasing visual acuity (20/100). OCT showed a worsening of the neuroepithelial detachment associated with hyperreflective spots preferentially located on the external retina and in the detached area. During the following months, the patient showed a partial recovery of visual acuity (20/50) despite the tumor collapse and the development of subretinal fibrosis confirmed at OCT scans (Figure 3). No fluid relapse was noted during 1 year follow-up and stable visual acuity was maintained.
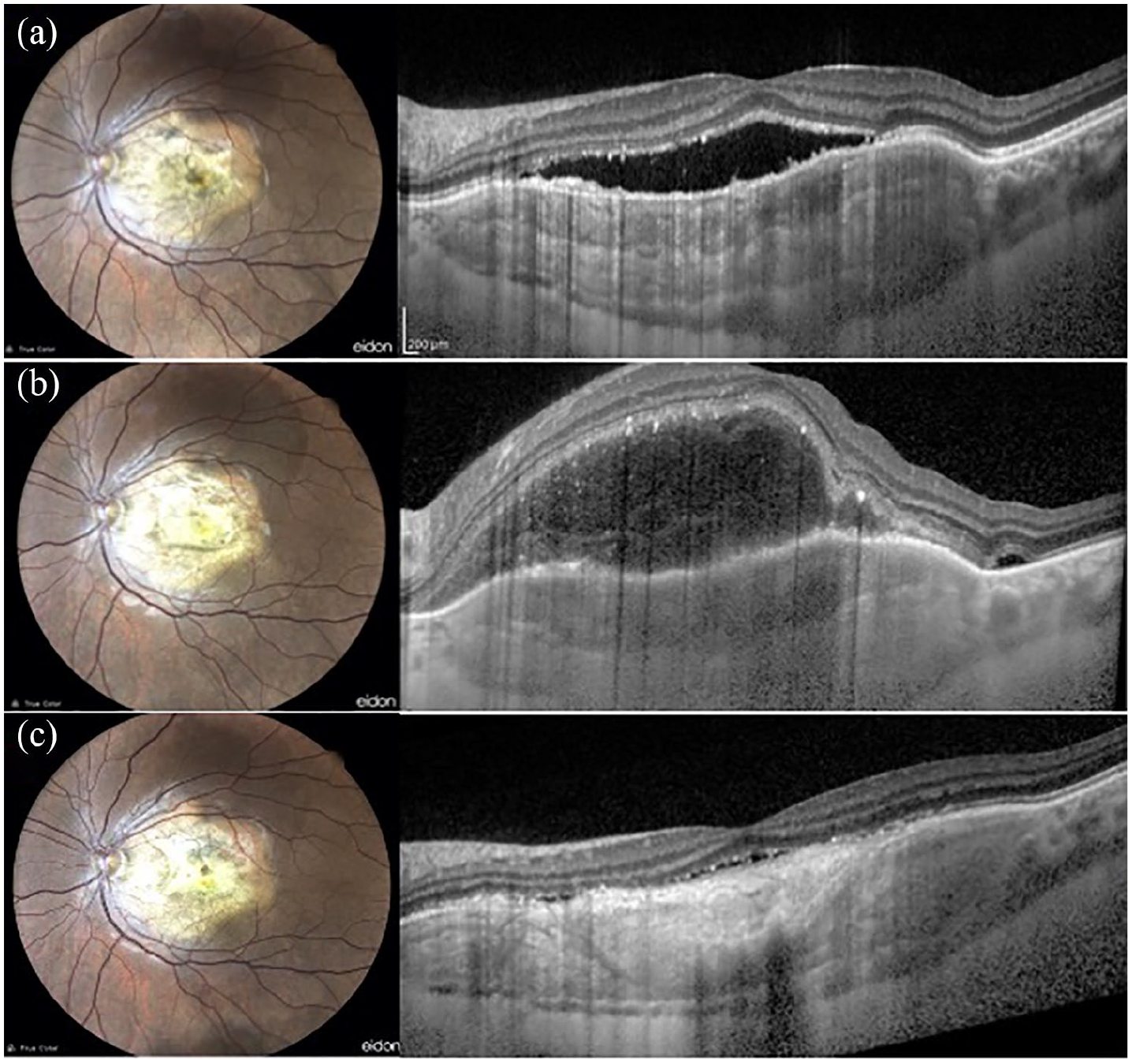
Fundus photograph and EDI-OCT scan at: (a) 1 year of follow-up reporting a serous subfoveal detachment of the neurosensory epithelium in the affected eye, (b) soon after the second PDT treatment, OCT scan revealed worsening of the neuroepithelial detachment associated with hyperreflective spots preferentially located on the external retina and in the detached area, and (c) during the follow-up months, OCT scans showed the development of subretinal fibrosis.
Discussion
Choroidal osteoma is an uncommon ossifying tumor originating in the choroid, with a rare frequency of occurrence. Despite CO is a benign tumor with well defined clinical features, its clinical course is generally poor with 58% of patients presenting visual acuity of 20/200 or worse by 10 years and 62% by 20 years. 5 To date, few studies have been addressed in finding the physiopathological factors influencing the tumor course. A large part of patients with a diagnosis of CO complain visual loss mostly related to the onset of serous retinal detachment, subretinal fluid, macular atrophy, or development of subretinal new vessels. Since all these changes could induce visual impairment, the tumor location has a significant meaning in the clinical course, with a poor prognosis in tumors located in the macular area.
In our case, vision loss was essentially related to foveal detachment and photoreceptors malfunction attested by the lengthening of the outer segment. Even if CNV was excluded, based on angiographic and OCT-A findings, anti-VEGF therapy was attempted, on the assumption that SRF accumulation could have been attributable to tumor vessels endothelial barrier breakdown induced through an upregulation of VEGF. Although there is no evidence of Anti-VEGF therapy efficacy in case of chronic epitheliopathy and impairment in choriocapillaris/choroidal outflow, the hypothesis of tumor vessels dysfunction could be in line with the observation of Lafaut et al. that reported, on ICG study, the presence of abnormal vessels inside the CO causing late dye leakage. 6 However, considering the nonresponse to the treatment as happens in chronic epitheliopathy, VEGF seems not to be involved in the physiopathological mechanisms leading to SRF. 7 Following the failure of the anti VEGF treatment photodynamic therapy was then performed.
PDT is a two steps therapeutic tool positively used in treating the choroidal neovascularization associated with the tumor. It entails the systemic infusion of a photosensitizing agent and its activation by exposure to low-energy laser at the adapted wavelength. When activated by laser light, free radicals are released, and interacting with the blood vessels endothelial cells induce the production of modulators as thromboxane and TNF-a, causing vasoconstriction, and thrombosis. 8 First approved for the treatment of subfoveal choroidal neovascularization (CNV) in age macular degeneration, off-label use of PDT has become, during the past two decades, an accepted therapeutic approach in other chorioretinal disease. It has proven to be effective to induce subretinal fluid resolution in central serous chorioretinopathy (CSC) and in treating exudative retinal detachment in symptomatic circumscribed choroidal hemangioma. 9 PDT has been recently proposed for the treatment of extrafoveal vision-threatening choroidal osteoma with the aim of inhibiting the tumor growth under foveola and preserving visual acuity. It seems to stimulate the decalcification of the lesion that, when occurs spontaneously, is associated with regression of the tumor and inhibition of its growth.10,11 Although PDT is considered a safe treatment, different uncommon but worrying complications have been reported. RPE alterations, choriocapillaris hypoperfusion, and choroidal ischaemia may arise after PDT treatment. 12 Additionally, PDT causes a hypoxic damage which could be responsible for CNV development. 13 The case we have presented regards a macular choroidal osteoma involving the fovea, associated with subretinal fluid, treated with fovea sparing PDT. The decision to perform PDT excluding the foveal and parafoveal areas had the rationale of minimizing a possible central tumor decalcification, which is reported to be related with poor long term vision. The association between decalcification and reduced visual acuity still remains poorly understood. However, RPE alterations and choriocapillaris atrophy are often associated with the tumor decalcification and could be responsible for photoreceptor cells apoptosis and low visual outcome.
Our case showed PDT showed to be effective for the resolution of subretinal fluid with a progressive reconstitution of the ellipsoid zone and external retina depicted in OCT scans and a recovered good visual acuity. After 1 year, PDT beneficial effects were still present, and no clear evidence of decalcification in the foveal area was noted at the fundus examination. However, the second treatment performed 1 year later, has had a completely different outcome, due to the tumor collapse and the development of subretinal fibrosis. The cause of this different outcome still remains unclear. Nevertheless, the progressive decrease of tumor thickness observed on EDI OCT scans during follow-up could be the expression of calcium loss that could have changed the tumor characteristics and may have caused a relative overtreatment of the last PDT. Considering the effectiveness and safety reported for low-fluence PDT, modified protocol treatment, including an abbreviated duration of laser emission, half-dose of verteporfin, and a reduced fluence rate, could be a valid alternative to the conventional PDT to achieve more favorable treatment outcomes.
Conclusions
VEGF upregulation seems not to be involved in inducing SRF in case of CO not associated with CNV. Foveal sparing PDT therapy is effective in inducing fluid reabsorption and obtaining good visual recovery in short-term follow-up. However, the choice of treatment should be taken being aware of its possible complications. Further studies are needed to evaluate long-term evidence supporting the role of PDT in the treatment of macular choroidal osteoma. To date, the management of CO with macular involvement remains challenging.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The patient reviewed this case report and provided oral consensus for publication.