
Abstract
Purpose:
Royal College of Ophthalmologist recent guidance recommended delaying cross-linking services during the COVID-19 pandemic. This study investigates the effects of such delays in the delivery of cross-linking services in patients with keratoconus progression.
Methods:
Retrospective observational study of 46 patients with keratoconus progression, whose cross-linking was delayed due to the COVID-19 pandemic. Demographic and clinical details were obtained from assessments on the day of listing, and subsequent review on the day of the procedure. Topographic indices included keratometry of the posterior and anterior corneal surface, maximum keratometry (Kmax), thinnest corneal thickness, ABCD progression and progression based on standard criteria recommendations (1.5 D Kmax & 20 microns thinning).
Results:
A total of 46 eyes were analysed with an average time between being listed for CXL and having the procedure done was 182 ± 65 days. The delay due to COVID-19 was of 3 months. In this time period they had a significant worsening of all keratometric indices and lost almost one line of visual acuity (0.19 ± 0.19 to 0.26 ± 0.18 LogMAR, p: 0.03). Thirty two eyes (70%) demonstrated progression in accordance with the ABCD progression criteria, while 18 eyes (39%) showed either an increase in Kmax of more than 1.5D or a thinning in corneal thickness of at least 20 μm.
Conclusions:
The treatment delay for the keratoconus patients caused further progression and vision worsening. We recommend that corneal collagen crosslinking needs to be considered as a high priority intervention.
Keywords
Introduction
The current coronavirus 2019 pandemic has led to a global crisis within health systems. To mitigate the risk of viral transmission within hospitals, care providers operated on an emergency-only basis. Within ophthalmology departments, elective clinical and surgical activities were suspended as per national guidance. 1 Ophthalmic services, typically comprising of high-volume outpatient clinics and theatre lists, were further limited by social distancing measures.2,3 In view of this, The Royal College of Ophthalmologists published the following document; ‘Prioritisation of Ophthalmic Procedures May 2020’. This provided recommendations for re-prioritisation of ophthalmic services during the heightened restriction. These guidelines considered keratoconus patients as lower risk, advising delaying corneal collagen crosslinking (CXL) by 3–4 months for rapidly progressing disease or very thin corneas. For those not in this category, a delay of more than 4 months was recommended. 1 The objective of this study is to investigate the rates of keratoconus progression of patients present on the waiting list for corneal cross-linking during the period of suspension due to coronavirus outbreak.
Methodology
Retrospective, single-centre case series where patients who had been listed for corneal collagen crosslinking at The Royal Liverpool University Hospital (Liverpool, UK) prior to the time of suspension of the service (March 2020–June 2020), due to coronavirus outbreak, were included. All patients experienced a delay in treatment due to the suspension of the service and were rebooked in accordance with Royal College of Ophthalmologist Guidance Document: Prioritisation of Ophthalmic Procedures. 1 Rapid disease progression and patients with thin corneas (less than 400 microns) were given priority, as per the aforementioned document. Patients under 18 years old were also prioritised, as this has previously been identified as a risk factor for progression. 4
Corneal topographic data (Oculus Pentacam HR Type 70900) and corrected distance visual acuity on the day of being listed for corneal crosslinking and on the day of the corneal cross-linking treatment were recorded.
Keratoconus progression during the time between listing and procedure (initial time in the waiting list, plus, additional delay due to the service suspension) was calculated according to the standard progression criteria and the ABCD progression analysis.
The standard progression criteria was defined as either a steepening in K-max of at least 1.5D or as a thinning in minimum corneal thickness of at least 20 µm. 5
The ABCD progression was defined as a worsening of at least one parameter outside the stated 95% confidence interval or a worsening of at least two parameters outside of an 80% confidence interval for the keratoconus populations. 6
Percentage of patients who experienced keratoconus progression according to each criterion were calculated. Factors associated with progression were also investigated.
The retrospective data collection followed the tenets of the Declaration of Helsinki and was approved by the local Institutional Review Board (A02719). No funding was received for the following study. No conflict of interest existed for any author of this study.
Statistical analysis
The statistical analyses were performed using STATA 14.0 (StataCorp, College Station, TX) and a p-value of less than 0.05 was considered statistically significant. All measurements were expressed as mean ± standard deviation (SD). The normality of all the data was estimated using the Shapiro-Wilk normality test. Comparison for the same patient of baseline versus post-COVID follow-up were performed with paired t-test in case of normally distributed data and with matched-pairs Wilcoxon signed-rank test if not normally distributed.
Comparison between progressed and non-progressed patients were performed with the Student t-test in case of normally distributed data and with two-sample Wilcoxon rank-sum (Mann-Whitney) test in case of non-normally distributed data.
A generalized linear model was performed to analyse the association of different parameters with progression.
Results
In total, 46 eyes, of 34 patients, were reviewed. All eyes demonstrated evidence of keratoconus progression when listed for corneal collagen cross-linking (CXL), prior to suspension of services. Of these, 30 males and 16 females. It was noted that 39% had a history of atopy and 25% were contact lens wearer – of which, 60% used soft contact lenses, 40% rigid contact lenses. The mean age was 25.4 ± 7.5 years. Fifty two percent of listings were intended for bilateral CXL.
The average time between being listed and having the procedure done was 182 ± 65 days. Additional delay due to the service suspension (COVID-19) accounted to approximately 3 months.
Best corrected visual acuity and tomographic measurements taken at baseline and post-delay are summarised in Table 1, with respective p-values.
Summary of baseline and post-COVID characteristics for the population.
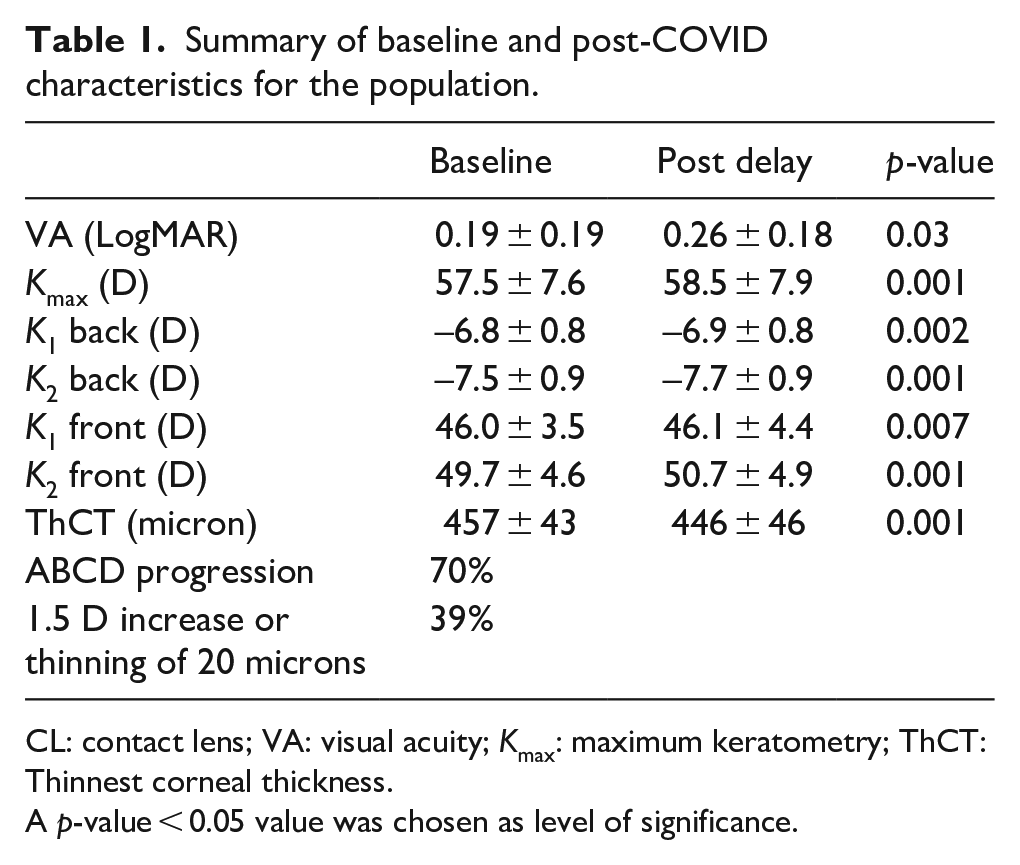
CL: contact lens; VA: visual acuity; Kmax: maximum keratometry; ThCT: Thinnest corneal thickness.
A p-value < 0.05 value was chosen as level of significance.
It was noted that 32 eyes (70%) demonstrated progression in accordance with the ABCD progression criteria. Using this criterion, patients listed for a bilateral CXL showed progression in both eyes in seven cases (58%), unilateral progression in two cases (16%) and no progression in three cases (25%).
With regards to the tomographic criteria, 30% of patients had an increase in K-max of more than 1.5D and 17% had a thinning in corneal thickness of at least 20 µm. In total, 18 eyes (39%) had at least one among these two criteria and were considered progressed. Using this criterion, patients listed for a bilateral CXL showed progression in both eyes in three cases (25%), unilateral progression in three cases (25%) and no progression in six cases (50%). Tomographic data is summarised in Table 1.
Further analysis comparing characteristics of patients who demonstrated further progression, against those who did not, was performed. Progression was evaluated with both ABCD and standard criteria. A statistical significance difference in baseline K-max between progressed and non-progressed eyes was noted as a factor in progression of keratoconus using both criteria. Results are summarized in Table 2.
Characteristics of patient who progressed compared to those who didn’t progress according to ABCD and Liverpool criteria of progression.
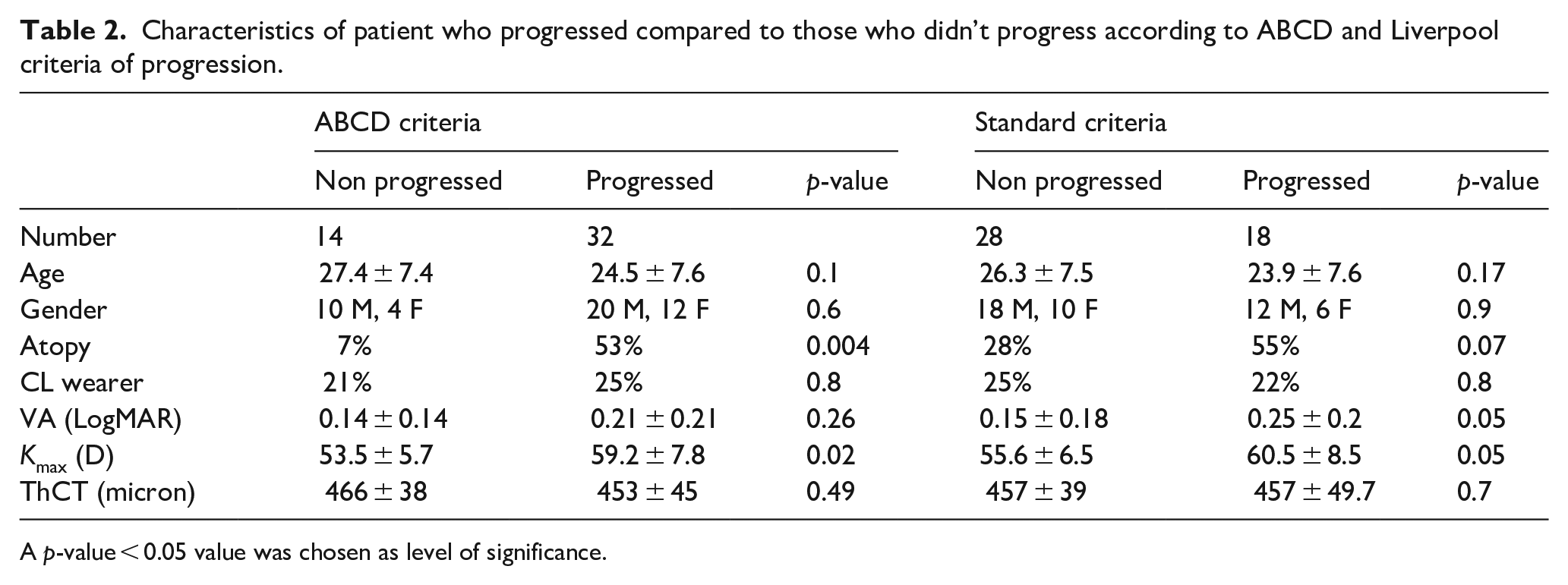
A p-value
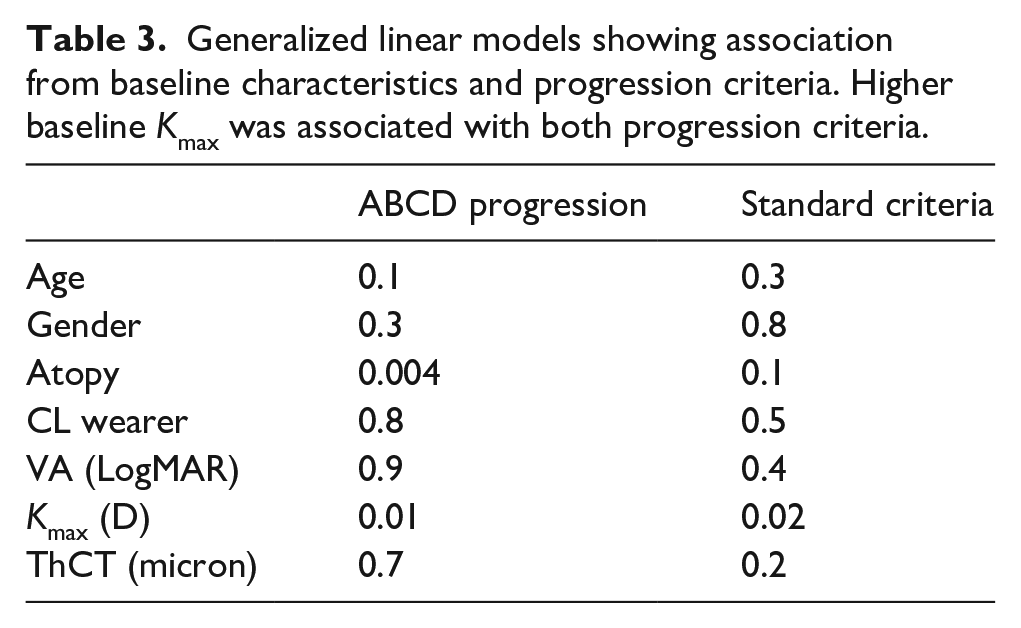
A generalized linear model, analysing factors associated with progression, was performed. This reiterated that a higher baseline K-max was associated with progression in both the ABCD and Liverpool criteria. Atopy was also found to be associated with keratoconus progression using the ABCD criteria (p-value 0.004). In contrast, age, gender, CL wear, VA and) and thinnest corneal thickness (ThCT) showed no association (Table 3).
Generalized linear models showing association from baseline characteristics and progression criteria. Higher baseline Kmax was associated with both progression criteria.
Discussion
Progression of keratoconus not only compromises patients’ vision, but also has significant implications on quality of life. 7 It is therefore recommended that, in cases of documented progression, corneal collagen cross-linking be offered in a timely manner. 8 As previously discussed, The Royal College of Ophthalmologist COVID-19 Guidance imposed suspensions, and subsequent delays, of the corneal collagen cross-linking service. This procedure was considered a lower risk procedure, and therefore, treatment and follow-up were deferrable. Results from our study suggest that delays due to re-prioritisation of ophthalmic services has resulted in further progression of keratoconus – 70% of cases demonstrating ABCD criteria progression, and 39% in accordance with the standard progression criteria.
These findings are consistent with multiple previous studies, which have noted keratoconus progression between the time of initial listing and procedure.4,9,10 A pertinent difference to note however is the dramatic increase of progression demonstrated by this study, alongside longer delay times. Further to significant worsening of all keratometric indices analysed, patients lost almost one line of visual acuity. This is of utmost importance, as keratoconic eyes in which visual acuity cannot be corrected with glasses or contact lenses, may need a cornea transplant – an intervention with significant risks and complications. 11
Factors found to be associated with greater risk of progression included higher baseline K-max (in both ABCD and standard progression criteria), as well as history of atopy (ABCD progression criteria only). When considering reprioritisation of corneal cross-linking services, it may be advisable to consider such factors when assessing a patient’s risk of progression. Furthermore, current guidance advises a delay of 3–4 months in a ‘very thin cornea’, 1 however, considering risks associated with corneal collagen crosslinking in corneal thicknesses below 400 µm, 12 we speculate that further corneal thinning associated with such delays may lead to patient’s becoming ineligible for this treatment option.
Due to the COVID-19 pandemic, the study period, as well as the availability of patients was restricted– resulting in a smaller sample size. Although we appreciate this limitation, it is to be noted that that these findings follow on from previous, larger studies, that have demonstrated the effects of delays in keratoconus treatment.4,9 Another area of consideration is the variation in accurately classifying keratoconus progression. In view of this, we felt it necessary to use a criteria that is locally acknowledged, as well as an internationally recognized criterion. For future analysis, the authors also recommend addressing other risk factors, including age of patient, family history and ethnicity of the patient.
The authors appreciate that COVID-19 has posed difficult questions and decisions to make, which have forcibly resulted in the suspension of those services deemed less essential to guarantee the best possible care to our patients. However, we believe that the results of our study clearly demonstrate that delays in cross-linking treatment has had important implications for both patient’s vision and limiting therapeutic options available for patients with keratoconus. We therefore suggest that, in the possibility of a second wave resulting in re-implementation of service restrictions, all patient be risk stratified – with atopy and K-max being considered, alongside factors previous described. 4 Subsequently, those considered higher risk of progression be categorized as high priority for corneal collagen cross-linking and treated without further delays.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.