
Abstract
Purpose:
To objectively analyze the optical quality of the FineVision Toric intraocular lens (IOL) with two cylinder powers when different combinations of rotations and residual refractive errors are induced.
Methods:
This study assessed the FineVision Toric IOL with two different cylinder powers: 1.5 and 3.0 diopters (D). Three different rotation positions were considered: centered, 5° and 10° rotated. An optical bench (PMTF) was used for optical analysis. The optical quality of the IOLs was calculated by the modulation transfer function (MTF) at five different focal points (0.0, 0.25, 0.50, 0.75, and 1.00 D).
Results:
The MTF averaged value of the reference situation was 38.58 and 37.74 for 1.5 and 3.0 D of cylinder, respectively. For the 1.5 D cylinder, the combination of 5° of rotation with a defocus of 0.25, 0.50, 0.75, and 1.0 D induced a decrease on the MTF of 12.39, 19.94, 23.43, 24.23 units, respectively. When induced rotation was 10°, the MTF decrease was 17.26, 23.40, 24.33, 24.48 units, respectively. For the 3.0 D cylinder, the combination of 5° with 0.25, 0.50, 0.75, and 1.0 D of defocus, induced a decrease on the MTF of 12.51, 18.97, 22.36, 22.48 units, respectively. When induced rotation was 10°, the MTF decrease was: 18.42, 21.57, 23.08, and 23.61 units, respectively.
Conclusion:
For both FineVision Toric IOLs there is a certain optical tolerance to rotations up to 5° or residual refractive errors up to 0.25 D. Situations over these limits and their combination would affect the visual quality of patients implanted with these trifocal toric IOLs.
Keywords
Introduction
Preoperative astigmatism is a key factor to be addressed by surgeons for successful cataract surgeries and intraocular lens (IOL) implantation. Some data estimates that around 50% of patients that underwent cataract surgery present preoperative astigmatism over 1.00 D. 1 Therefore, the global impact of preoperative astigmatism in the quality of vision represents a challenge that exceeds the classical cataract surgical burdens.
To compensate preoperative astigmatism, toric IOL implantation is the main method used among clinicians. 2 One of the most important factors for successful surgeries with toric IOLs implantation is the reaching of a proper alignment of the IOLs. 3 It is easy to find some degree of rotation after IOLs implantation but in general, toric platforms show high rates of stability3,4 and good clinical results. 2
Multifocal toric IOLs also showed good clinical results and high rates of spectacle independence of astigmatic patients for both distance and near vision.5–7 It has been reported that the impact of rotations in distance vision is greater for multifocal (bifocal) toric than for monofocal toric IOLs. 8 Currently, trifocal toric IOLs are also available for surgeons and the impact of potential rotations of these IOLs has been recently reported. 9
Furthermore, slight over-refractions are common after cataract surgery. However, these over-refractions have relevant clinical implications as they can worsen the distance vision. Hence, the analysis of the combination of some degree of rotation and residual refractive error after trifocal toric IOLs implantation may offer a useful clinical approach to potential clinical scenarios after surgeries. This analysis should be done under the same conditions to eliminate inter-subject variability and physiologic variables that may confound measurements in vivo. For this purpose, an optical bench represents an objective and non-invasive method, as previously reported. 9
Therefore, the current research aims to objectively analyze the optical quality of a trifocal toric IOL with different cylinder powers when determined amounts of rotation are combined with positive residual refractive errors.
Methods
Intraocular lens designs studied
The trifocal toric IOL analyzed was the FineVision Toric IOL (PhysIOL; Liège, Belgium). This is a double C-loop IOL with 5° angulation made of 26% hydrophilic acrylic material (hydroxyethylmethylmethacrylate-co-methylmethacrylate copolymer) with a refractive index of 1.46. 9 The lens incorporates both UV and blue-light filtration and has been used in a recent study. 9 As in the case of the non-toric version, trifocality is reached by combining two bifocal apodized diffractive patterns for far/near and far/intermediate vision respectively.9–11 The lens presents a biconvex aspheric design with −0.11 μm of spherical aberration for a 6.0 mm of pupil size. The overall diameter of the lens is 11.40 mm and the optic zone is 6.00 mm. The optical power of the lens goes from +6.0 to +35.0 D in 0.50 D steps. The addition powers of the lens are +1.75 and +3.50 D for intermediate and near vision respectively. The power of the sphere was +20.0 D. Cylinder powers of 1.5 and 3.0 D were considered as a representation of low and moderate-high astigmatism, respectively. 12
Optical bench
The image quality of each IOL was assessed with the PMTF optical bench (LAMBDA-X, Belgium) with the Software version: 1.13.6, used in similar previous investigations.9,11,13,14 This device complies with International Standard Organization (ISO) 11979-2 and 11979-9 requirements. The optical bench allows optical quality measurements at different frequencies, focal planes, and pupil apertures.
At the same time, for toric IOLs analysis and in order to simulate the principal meridians of the cornea, the optical bench presents specific horizontal and vertical targets to align the IOLs under study.
Optical quality assessment
The modulation transfer function (MTF) analysis is considered as a standard method when it comes to analyzing the optical quality of IOLs as optical systems.15–20 An optical system’s MTF characterizes the image degradation caused by the optical system 17 and drop in the MTF results could lead to a decrease of the optical system’s performance. 17 Previous authors have related MTF values to visual function parameters such us visual acuity. 21 Therefore, to achieve the main aim of the current study, the MTF analysis was performed.
Pupil size could affect the power distribution of the light through multifocal designs. 10 In order not to limit that distribution of light through the lens, an extreme small pupil aperture was avoided. Then, the selected pupil aperture for the current research was 4.5 mm. 9 As reported in previous studies,9,11,13,14,20 the MTF value was considered as the “average modulation value” which is the averaged values across all frequencies within the 0.0–100.0 cycles/mm range. This value is proportional to the area under the MTF curve between 0.0 and 120.0 cycles/mm.9,11,13,14,20 These range comprise from low to high spatial frequency values. Higher spatial frequencies are related to a larger drop in contrast due to an optical system. Then, the higher MTF value in the curve the better optical quality of the lens. At the same time, MTF curves at different focal points and for all different positions were performed.
Impact of defocus and rotations
In the current work, the IOLs studied were analyzed for a centered position and with 5° and 10° of rotation. In order to analyze the impact in distance vision of combining these rotations with some degree of residual defocus, the optical quality was also analyzed in each case for different positive foci (0.25, 0.50, 0.75, and 1.00 D) around the distance focal point (0.00 D). These positive foci are related to the distance focal points of myopic residual errors.
Following the methodology of a recent study, 9 measurements were taken with the IOL meridians aligned with the specific targets of the optical bench for a centered position to simulate the principal corneal meridians. For the analysis of the degradation of the optical quality, the IOLs were rotated by 5° and 10° versus the aligned position and the optical quality was assessed at the specific targets. As the targets and the principal meridians of the IOLs are always perpendicular, the degradation of the image was assessed for only one (and always the same) target.
Previous investigations correlated MTF values with potential visual acuity changes. Felipe et al. 21 described that the visual acuity would vary by 0.18 decimal units per 10 units of average modulation variation under photopic conditions. Considering that the previously reported visual acuity at distance vision with this IOL was slightly over 20/20, 22 for the current study we considered 10 MTF units as the limit of tolerance which corresponds to almost two lines of vision.
Results
Figure 1 and Table 1 show the results of the IOLs with low cylinder power (1.5 D – left part of the figure) and moderate-high cylinder power (3.00 D – right part of the figure). The figure presents the MTF curves for all defocus points (0.00, 0.25, 0.50, 0.75, and 1.00 D) for centered and rotated situations. Since the MTF for 0.00 D of defocus and for a centered position is expected to achieve the best optical results, this curve is presented as the reference value in all cases. On the other hand, the table compiles the average modulation values between 0.0 and 120.0 cycles/mm for all the specified situations. At the same time, the MTF averaged value for 0.00 D of defocus and for a centered position is showed as the reference value and all values are compared to this value. Regardless the amount of cylinder, the reference value showed to be similar.
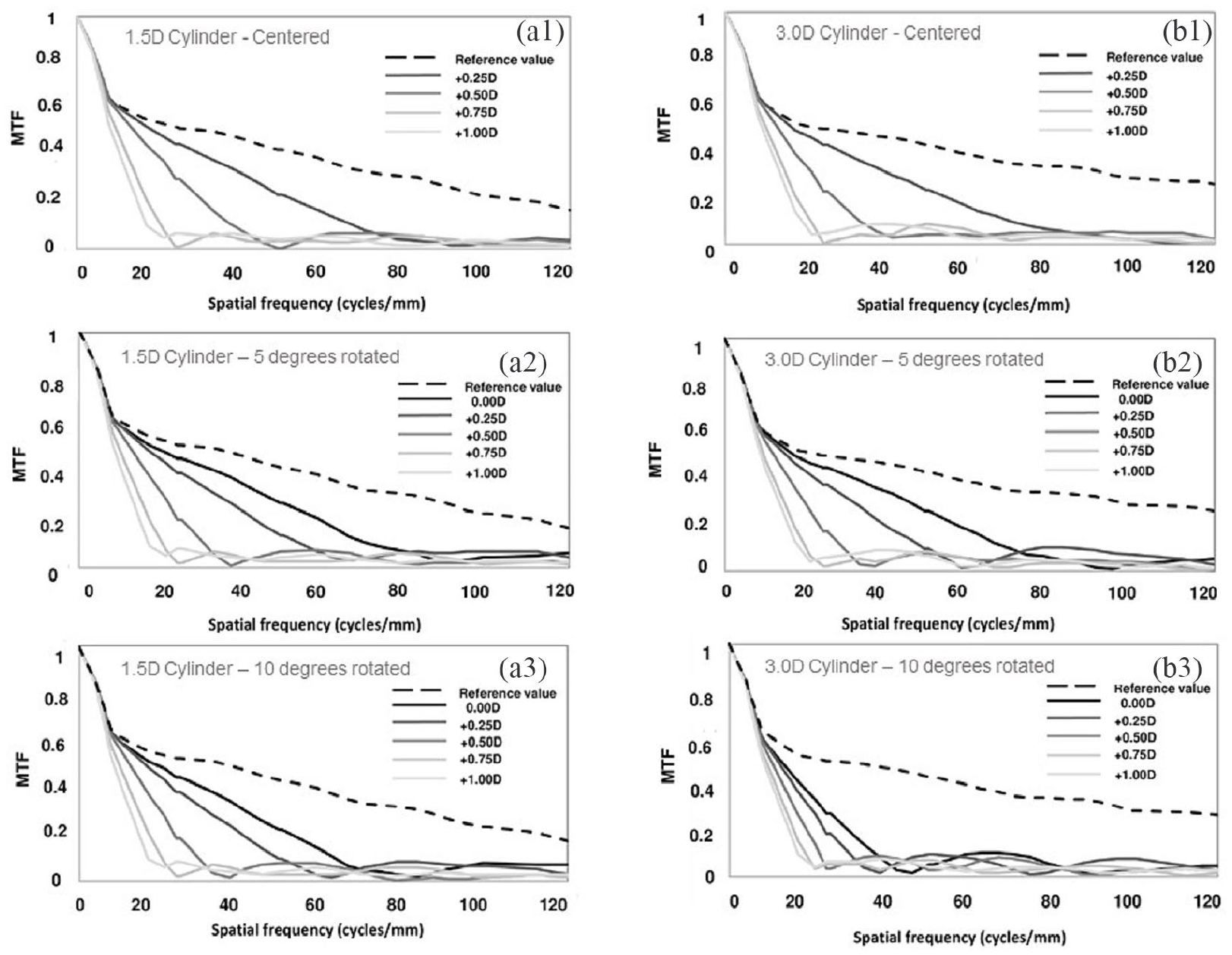
MTF curves at different object vergences (0.0, 0.25, 0.50, 0.75, and 1.0 D) for the low cylinder (a – left part of the figure) and the moderate-high cylinder lens (b – right part of the figure) at three different positions: centered (1), 5° rotated (2), and 10° rotated (3).
Average modulation values of the lenses under study at different focal points (residual defocus) and for the three different positions (centered, 5° rotated, 10° rotated).
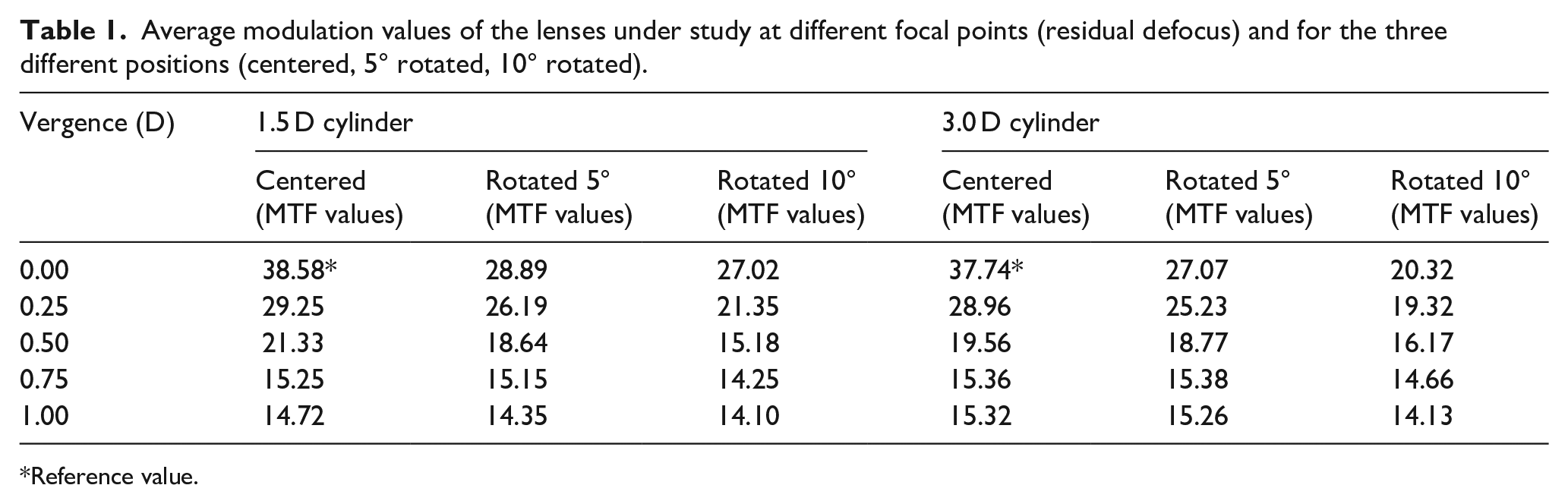
Reference value.
Optical quality analysis: Rotation and defocus
The left-mid and left-bottom parts of the figure show results of the low cylinder (1.5 D) IOL with 5° and 10° rotation, respectively (A.2 and A.3). The right-mid and right-bottom parts of the figure show the outcomes of the moderate-high cylinder (3.0 D) IOL with 5° and 10° rotation, respectively (B.2 and B.3). For both cylinders, Table 1 shows that a defocus of 0.25 induced a decrease in MTF average value around 15 units. When the defocus is ⩾0.5 D the decrease was ⩾20 units. For 5° rotation, the results are similar to those of the centered position with 0.25 D of defocus. For this rotated situation, a defocus of 0.25 D did not induce a significant decrease of MTF average values (only 5 units vs rotated position without defocus and around 15 units vs the reference value). However, with a higher defocus the decrease was over 25 units.
A rotation of 10° was equivalent to a defocus of 0.50 D in a centered position, with a decrease in MTF average values over 20 units. Obviously, in this situation any combination with some amount of defocus also induced a decrease over 20 units versus the reference value.
Discussion
The current study analyzed the impact of different degrees of rotation combined with residual refractive errors in the optical quality of a trifocal toric IOL. A certain tolerance to low defocus errors and low degrees of rotations was found. Nevertheless, when these situations were combined the optical quality of the IOL decreased significantly.
Previous authors have reported clinical outcomes of the trifocal IOL under study. 22 However, to analyze the impact of the postoperative complications considered in this study, an optical bench was used. Beyond the differences between clinical and optical quality results, the latter could explain or justify different clinical outcomes23,24 and could overcome the limits of classical clinical studies.
Both Figure 1 and Table 1 show the optical quality results for all the situations considered in the study. The first and the optimal situation to be analyzed for each IOL was the IOL without defocus (0.00 D object vergence) in a centered position, which was the “reference value”. The MTF for the rest of the situations were compared to this reference in order to discuss the effect of defocus-rotation combinations.
As mentioned in the methods section, the visual acuity would vary by 0.18 decimal units per 10 units of average modulation variation under photopic conditions. Analyzing the results of both lenses (1.5 and 3.00 D of cylinder) (Figure 1; Table 1) in a centered situation (analyzing the table vertically), it is possible to observe that a defocus of 0.25 D induces a worsening under 10 MTF units versus each reference situation. This deterioration goes over 15 units for 0.50 D and over 20 units for 0.75 and 1.0 D of defocus. Hence, it could be considered a defocus of 0.25 D as tolerable. At the same time, in Table 1, it could be observed that a rotation of 5° (without defocus) induces a worsening comparable to 0.25 D of defocus. On the other hand, a rotation of 10° in the 1.5 D cylinder lens induces a worsening of 11.56 MTF units, being over the limit of tolerance. For the 3.0 D cylinder lens, 10° of rotation induces a decrease of 17.42 MTF units, which is significantly higher than the low cylinder case. For a combination of 0.25 D with 5° of rotation the worsening is similar for both lenses, being 12.39 and 12.51 units for the 1.5 and 3.0 D cylinder lenses, respectively.
Then these results suggest that there is certain tolerance to defocus up to 0.25 D or rotations up to 5°. However, a combination of 0.25 D and 5° exceed the limit of tolerance and could affect the visual quality. Obviously, for all potential combinations over 0.25 D and 5°, the optical quality of these trifocal toric IOLs decreased significantly (over 15 MTF units). In these cases, surgeons should consider surgical corrections for improving the visual quality of the patients.
The results showed in Table 1 present all potential combinations assessed in the study. These results, reading the table horizontally and/or vertically, could be a guide to understand whether reorientations or residual refractive correction (i.e. by corneal refractive surgery procedures) 25 could be the solution for restoring the visual quality of patients. For example, observing the results of the 3.00 D cylinder IOL at 0.25 D of defocus (horizontally), it is possible to observe that 10° of rotation induce a marked decrease in the optical quality. However, if the IOL is only reoriented (up to a centered position), the optical quality (and potentially the visual quality) could reach acceptable values. Another example could be the next defocus step, that is, the 3.00 D cylinder IOL at 0.50 D. Conversely, in the presence of a residual refractive error of 0.50 D, it is possible to observe that only a reorientation of the IOL itself would not achieve a tolerable value of visual quality. At the same time, only a surgical procedure for correcting this residual error could not provide a restoring of the visual acuity. Then, in that situation a reorientation should be combined with a correction of the residual refractive error.
Regarding the impact of residual refractive errors in the visual quality of patients implanted with trifocal IOLs, a previous investigation analyzed the effect of induced defocus with a trifocal (non-toric) IOL. 26 However, this previous study did not assess combinations of residual refractive errors and rotations (because it is impossible to analyze it in clinical studies). The results showed that defocus errors from 0.50 D affect the visual quality of patients at distance vision. Similarly, in our study, 0.50 D of defocus has a significant effect on the optical quality of the lenses and which could be correlated to those clinical results. This correlation confirm that our analysis could be a reliable approach to the visual quality of the patients. In addition, the analyzed combination of 0.25 D of defocus and 5° of rotation performed in our study has a similar impact if compared to 0.50 D of residual refractive error, confirming that the combination of low errors could induce a worsening of the visual quality.
We find it important to point out that the analysis through an optical bench does not fully represent a clinical scenario. But due to the aim of the study, this analysis is a useful and non-invasive methods for the simulated postoperative complications. In addition, some studies have reported a positive correlation of the results through optical simulation and their related clinical outcomes. 23 Despite the differences between clinical and theoretical approaches, the outcomes of the current study suggest that, even without defocus, rotations over 5° could affect the visual quality of the patients. Then, intraoperative position of trifocal toric IOLs seems crucial for clinical success with these premium lenses. Besides, the results as a function of defocus (residual refractive errors) show that these IOLs need for extreme accuracy in IOL calculation. This is due to two reasons: (1) Despite a certain tolerance, defocus errors of 0.50 D for centered IOLs show a decrease of the optical quality; (2) The results of the present study show that combinations of small residual refractive errors (0.25 D) with small amount of rotations (5°) are critical for the optical performance of these lenses.
To the best knowledge of the authors, this is the first work that objectively analyzed this trifocal toric IOL under the specified situations and no direct comparisons can be made with other studies. On the other hand, the lens under study is a widespread implanted IOL but other trifocal toric IOLs are commercially available. Therefore, these designs should be analyzed in similar future studies. Different pupil apertures and the analysis of residual refractive errors of different sign may give information of a wider postoperative refractive scenario. Finally, it would be interesting to analyze the impact of rotations and/or residual refractive errors at different distances of vision (multifocality) provided by these designs.
Despite the limitations of the study, the results could be the base for future studies that aimed to determine the limits of tolerance to misalignments and defocus errors with patients implanted with trifocal toric IOLs.
In conclusion, the results of the current study suggest that there is certain tolerance to defocus up to 0.25 D and rotations up to 5°. The combination of both situations (0.25 D and 5°) could decrease the optical quality beyond tolerable limits for the patients. For all situations and potential combinations over 0.25 D and 5°, the optical quality of these trifocal toric IOLs decreased significantly.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.