
Abstract
Background/objectives:
To compare the number of eye surgical procedures performed in Italy in the 2 months following the beginning of lockdown (study period) because of COVID-19 epidemic with those performed in the two earlier months of the same year (intra-year control) and in the period of 2019 corresponding to the lockdown (inter-year control).
Methods:
Retrospective analysis of surgical procedures carried out at 39 Academic hospitals. A distinction was made between elective and urgent procedures. Intravitreal injections were also considered. Percentages for all surgical procedures and incidence rate ratios (IRR) for rhegmatogenous retinal detachment (RRD) events were calculated. A p value <0.05 was considered significant.
Results:
A total of 20,886 versus 55,259 and 56,640 patients underwent surgery during the lockdown versus intra-and inter-year control periods, respectively. During the lockdown, only 70% of patients for whom an operation/intravitreal injection was recommended, finally underwent surgery; the remaining patients did not attend because afraid of getting infected at the hospital (23%), taking public transportation (6.5%), or unavailable swabs (0.5%). Elective surgeries were reduced by 96.2% and 96.4%, urgent surgeries by 49.7% and 50.2%, and intravitreal injections by 48.5% and 48.6% in the lockdown period in comparison to intra-year and inter-year control periods, respectively. IRRs for RRDs during lockdown dropped significantly in comparison with intra- and inter-year control periods (CI: 0.65–0.80 and 0.61–0.75, respectively, p < 0.001 for both).
Conclusion:
This study provides a quantitative analysis of the reduction of eye surgical procedures performed in Italy because of the COVID-19 epidemic.
Keywords
Introduction
In late 2019, multiple cases of pneumonia of unknown etiology were reported from the city of Wuhan in China. After genomic sequencing, it was found that these cases were caused by a novel virus, which was called Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). 1 This coronavirus infection spread throughout the world, leading to the World Health Organisation 2 declaring it a global pandemic on 11 March 2020. In an effort to limit the spread of COVID-19 (the disease caused by SARS-CoV-2), many governments enforced “lockdowns” of varying degrees.
To adhere to the restrictions imposed by governments and to reduce the risk of new case development, many medical societies worldwide issued recommendations regarding the cessation of routine clinical and surgical duties. These recommendations included the postponement of routine consultations and elective surgeries and the continuation of urgent or emergent care only. Ophthalmology has been significantly affected by these changes because this is a branch of medicine that largely deals with elective surgeries and because ophthalmologists rank among the medical specialties with the highest risk for COVID-19 infection.3–6
Since the start of the epidemic, several papers with recommendations and prevention measures that were set up by ophthalmology societies worldwide have been published.7–13 However, data about the reduction in ophthalmic surgical procedures because of the lockdown restrictions are scarce and limited to few centers in the world.14–17
In Italy, the lockdown measures came into force on 10 March 2020 18 and lasted for about 2 months, till the 3rd of May 2020. Based on government directives, people were forbidden from assembling in public places and allowed to move only for necessity, work, and health circumstances.
In order to reduce the chance of transmitting the virus to either patients or healthcare personnel, government directives decreed that all elective surgeries had to be deferred and only emergency healthcare services functioned. 19 Similar measures were taken by European countries first and then by the rest of the world, which followed within the span of a few weeks.
To estimate the effect of the COVID-19 outbreak on ophthalmic surgical procedures in Italy, the first European country that was severely struck by the epidemic, we gathered data from 39 Italian referral Institutional Ophthalmology Departments. The aim of the study is to provide a quantification of the COVID-19-related drop in volume of eye surgical procedures by comparing those performed during the lockdown period with those that were performed 2 months before the lockdown and in the period of 2019 corresponding to the lockdown.
Methods
This retrospective analysis of eye surgical procedures was performed at 39 Academic Italian hospitals. Among these 39 centers, 18 are located in the North, 11 in the Center, 5 in the South, and 5 on the main Islands (3 in Sicily and 2 in Sardinia) of Italy. The study period was defined as the time between 10 March and 9 May 2020 (2 months that started from the beginning of the lockdown). We compared the number of eye surgical procedures between the study period and two control periods, as follows: an earlier period during the same year (10 January–9 March 2020, “intra-year” control period) and a corresponding period during the previous year (10 March–9 May 2019, “inter-year” control period). The primary outcome was the percent of reduction of the urgent and elective surgical procedures that were performed in the lockdown period compared to the control periods. Secondary outcomes were the detailed analysis of the reduction of each surgical procedure and the analysis of the reasons for which planned surgeries were not performed. The study was conducted in accordance with the Declaration of Helsinki. Given the retrospective nature of the study, local Ethics committees and Institutional Review Boards waived the need for informed consent.
At all centers during the lockdown period, special strategies were implemented to guarantee treatment appropriateness while maintaining proper social distancing. A questionnaire for travel and contact history was administered to the patients and temperature measurement was performed upon clinic entry. In addition, a swab test confirming the absence of the virus in the nose or throat was collected in all patients planned to undergo surgery.
For data analysis, a distinction was made between elective and urgent procedures. Generally, cases that could be postponed for more than 4 weeks without considerable risk of loss of vision were qualified as “elective.” The elective procedures included the following: routine corneal transplantation, collagen cross-linking for slowly progressive corneal ectasia, standard cataract extraction, surgery on lacrimal system, surgery for strabismus, pars plana vitrectomy (PPV) for silicone oil removal, and epiretinal membrane (ERM) peel.
Urgent procedures included the following: any trauma repair, scleral buckling, or PPV for rhegmatogenous retinal detachment (RRD); PPV for dense vitreous hemorrhage; PPV for acute full-thickness macular hole; PPV for dropped nucleus/retained lens fragments; poorly controlled, sight-threatening glaucoma requiring trabeculectomy; glaucoma drainage implants; cataract extraction for narrow angle; cycloablation; and oncology surgery. Such a distinction largely reflects the released recommendations from the American Academy of Ophthalmology (AAO) 7 list of elective and urgent procedures.
Intravitreal injections were also considered. Generally, treatment for patients with neovascular age-related macular degeneration (nAMD), especially those in the first 2 years of treatment was maintained; treatment for new cases of nAMD and for macular oedema secondary to diabetes (DMO) and retinal vein occlusion cases was considered for cases with significant vision loss, and for monocular or quasi-monocular patients (best-corrected visual acuity >20/40 only in one eye). 13 An effort was made to evaluate each case individually to balance the risk of exposure to COVID-19 with the potential visual implications of treatment postponement. 20
Statistical analysis
Percentages of reduction for all variables and incidence rate ratios (IRRs) only for RRD (an event that is unlikely to remain undiagnosed within a few weeks) were calculated. The analysis of the variables relatively to the three periods considered for the study (“10/3/2019–9/5/2019” vs “10/1/2020–9/3/2020” vs “10/3/2020–9/5/2020”) was performed using Generalized Linear Mixed Model (GLIMMIX) procedure considering Poisson or Negative Binomial as distribution and log as link function. Poisson or Negative Binomial distribution were used in order to avoid the over-dispersion (in presence of over-dispersion the variance may be larger than the mean and therefore the results may affect the fit). The Tukey (homoscedasticity) and Games-Howell (heteroscedasticity) tests were used to correct multiple comparisons. Homoscedasticity was tested by Levene and Brown-Forsythe test. A p-value <0.05 was considered significant. Statistical analyses were performed by using SAS v.9.4 (SAS Institute Inc., Cary, NC, USA).
Results
According to the government rules, in all centers, the eye surgical procedures were limited to urgent procedures and to intravitreal injections. At four centers (two in the North and two in the South), the eye surgical activity was completely stopped during the lockdown period. Only one of these centers, that is, Bergamo, was at the very epicenter of the epidemic.
Globally, there were 87,626 surgical procedures and 45,159 intravitreal injections that were performed during the three periods (lockdown, intra-year, and inter-year controls) at the 39 academic centers that participated in this study; 50.7% of the patients who underwent surgery or intravitreal injection during the study period (n = 20,886) were male, and the mean (±standard deviation (SD)) age was 62.2 ± 19 years. For the 55,259 and 56,640 operations that were performed during the intra-year and inter-year control periods, 17,380 (46.6%) and 17,516 (45.3%) of the patients who underwent surgery were male, respectively, and their mean age was 66.3 ± 14.9 and 67.7 ± 12.5 years, respectively.
Data on the number of patients who finally underwent surgery/intravitreal injection among those who visited the hospital for urgencies and those called from the hospital to undergo surgery/injection during the lockdown period were available for 28 out of 39 centers. Overall, 70% of the patients for whom surgery/intravitreal injection was recommended underwent the procedure. Although they were advised to undergo surgery after a visit that was performed at the hospital or according to a scheduled appointment (e.g. for intravitreal injection), 23% of patients did not attend the appointment because of the fear of being infected at the hospital. An additional 6.5% of patients did not attend because they were concerned about going to hospital unaccompanied, because they were afraid of taking public transportation, or because of the risk of quarantine after their return home. A remaining 0.5% could not attend because the swab test results, which were needed to get access to operating rooms, were not available or because the results of a swab test were delayed.
Elective surgeries were reduced by 96.2% and 96.4%, urgent surgeries by 49.7% and 50.2%, and intravitreal injections by 48.5% and 48.6% during the lockdown period compared to intra-year and inter-year control periods, respectively (Figure 1 and Tables 1 and 2). Among elective surgeries, the most relevant reduction was observed for strabismus (−98.7%) and cataract operations (−97.7% and −97.8% compared to intra- and inter-year controls, respectively).
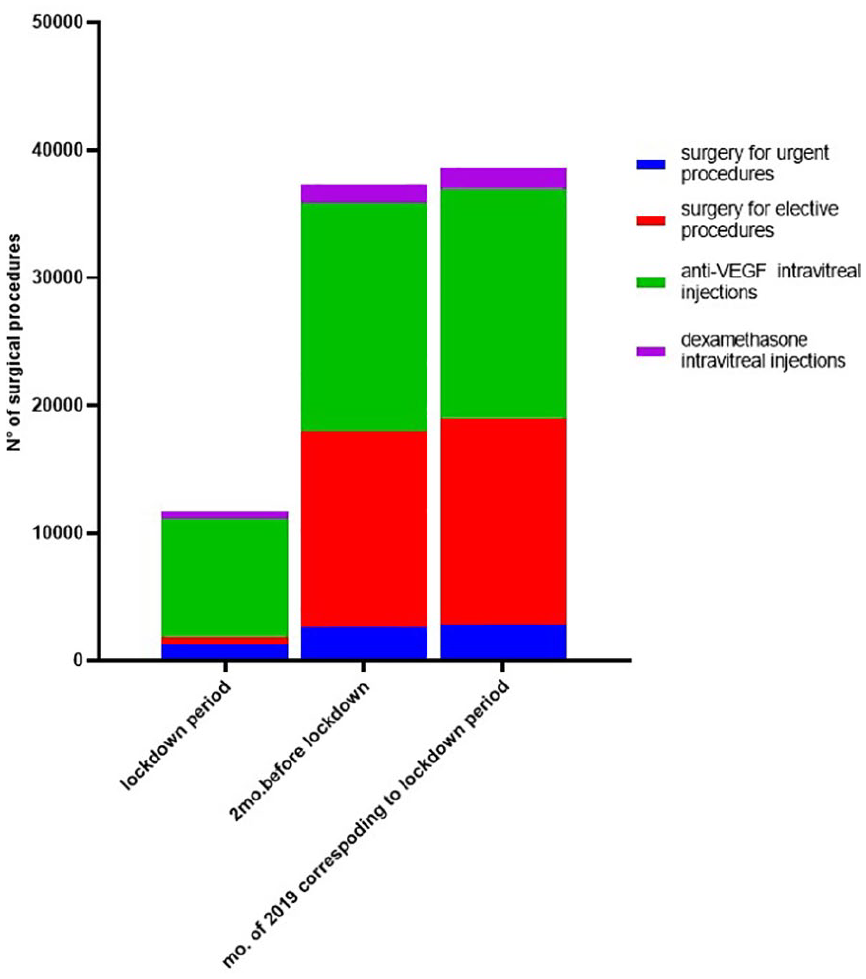
Stacked bar charts showing the number of elective and urgent surgical procedures and the number of intravitreal injections of anti-vascular endothelial growth factor and dexamethasone performed during the 2 months following the beginning of national lockdown (10 March–9 April 2020) compared with those performed in the period 10 January–9 March 2020 (pre-lockdown, intra-year control) and those performed in the period corresponding to the lockdown in 2019 (10 March–9 April 2019, inter-year control).
Comparison between the number of eye surgical procedures that were performed during lockdown in 2020 with those that were performed 2 months before the lockdown and with the period in 2019 that corresponded to the lockdown.
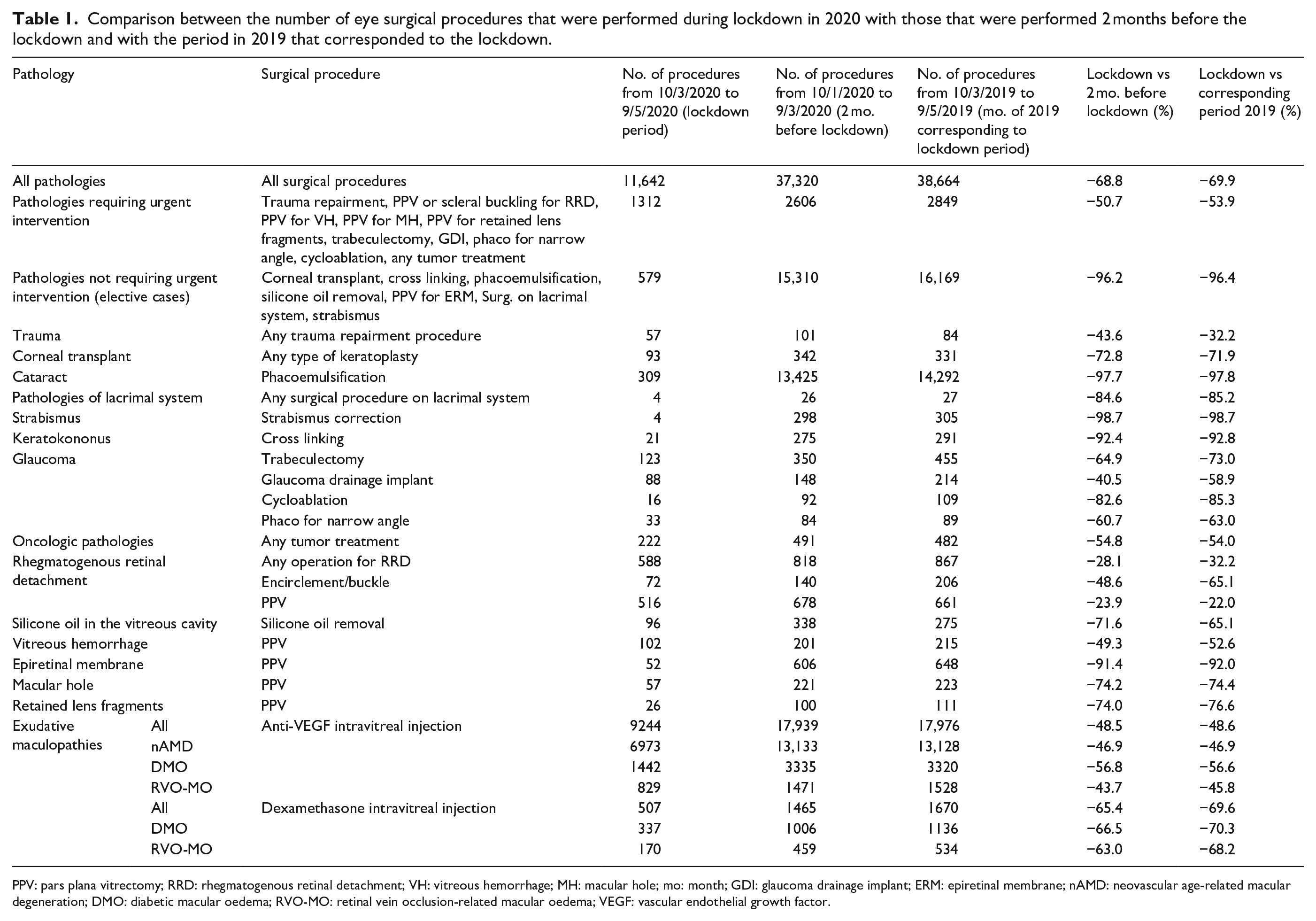
PPV: pars plana vitrectomy; RRD: rhegmatogenous retinal detachment; VH: vitreous hemorrhage; MH: macular hole; mo: month; GDI: glaucoma drainage implant; ERM: epiretinal membrane; nAMD: neovascular age-related macular degeneration; DMO: diabetic macular oedema; RVO-MO: retinal vein occlusion-related macular oedema; VEGF: vascular endothelial growth factor.
Comparison of the median of the surgical procedures that were performed during lockdown in 2020 with those that were performed 2 months before the lockdown and with those performed in the period of 2019 that corresponded to the lockdown.
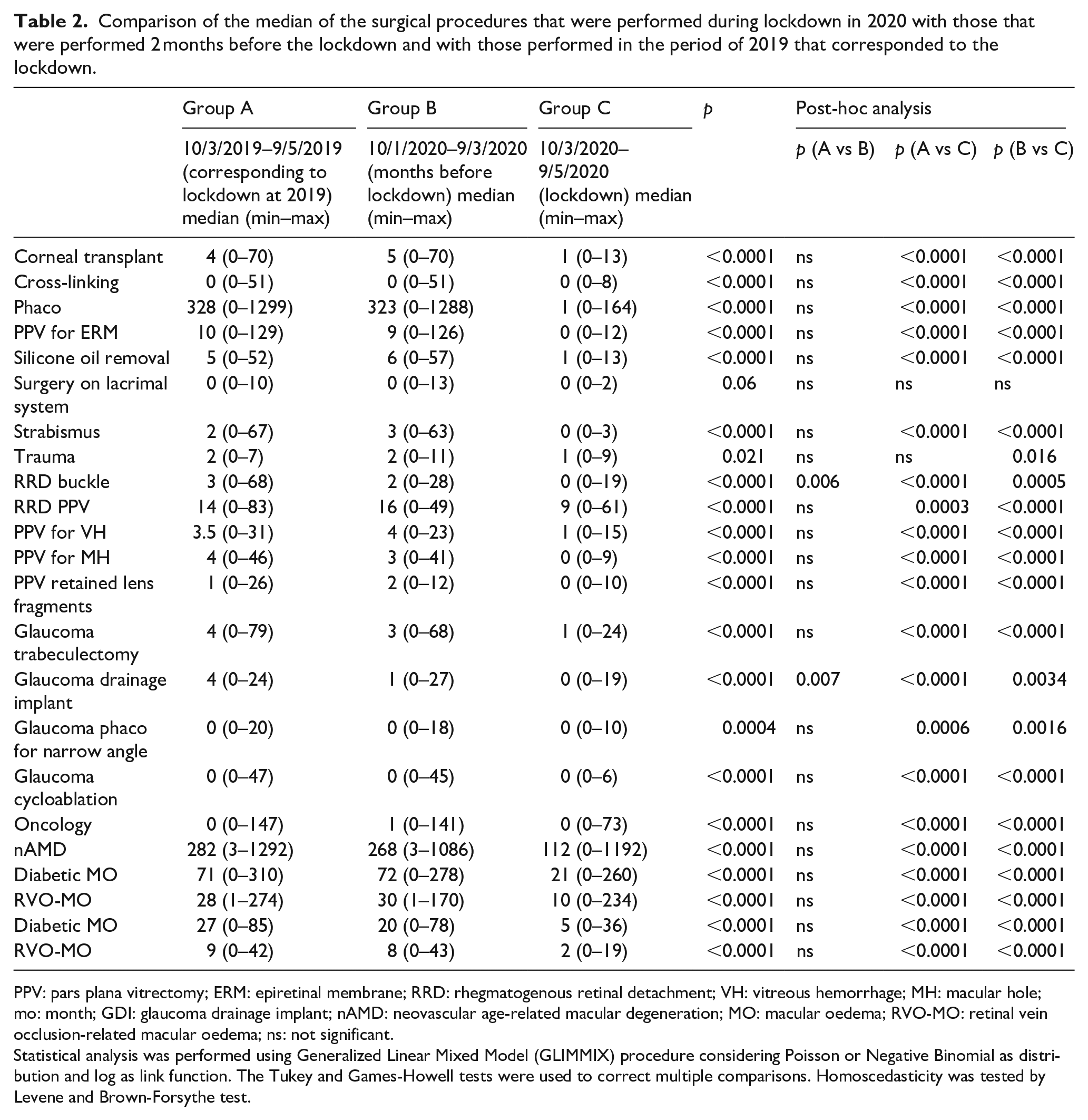
PPV: pars plana vitrectomy; ERM: epiretinal membrane; RRD: rhegmatogenous retinal detachment; VH: vitreous hemorrhage; MH: macular hole; mo: month; GDI: glaucoma drainage implant; nAMD: neovascular age-related macular degeneration; MO: macular oedema; RVO-MO: retinal vein occlusion-related macular oedema; ns: not significant.
Statistical analysis was performed using Generalized Linear Mixed Model (GLIMMIX) procedure considering Poisson or Negative Binomial as distribution and log as link function. The Tukey and Games-Howell tests were used to correct multiple comparisons. Homoscedasticity was tested by Levene and Brown-Forsythe test.
Among the urgent procedures, surgeries to repair the RRD (scleral buckling and PPV) decreased by 28.1% and 32.2%, thus scleral buckling procedures (−48.6% and −65.1%) were reduced more than the PPV procedures (−23.9% and −22.0%). We computed IRRs for the 60-day incidence of RRD (including scleral buckle and PPV) to compare the lock-down period with the two control periods. A significant drop was recorded for both comparisons (IRR 0.72, 95%, CI: 0.65–0.80, p < 0.001 compared to the intra-year control period and IRR: 0.68, 95%, CI 0.61–0.75, p < 0.001 compared to the inter-year control period, respectively).
Similarly, procedures to treat oncologic pathologies were more than halved during lockdown compared to control periods (−54.8% and −54.0%). For glaucoma surgery, cycloablations procedures were substantially reduced during lockdown compared to control periods (−82.6% and −85.3%), and trabeculectomies were reduced more than glaucoma drainage implants (−64.9% and −73.0% vs −40.5% and −58.9%).
Regarding anti-vascular endothelial growth factor (VEGF) intravitreal injections, the reduction of those performed for nAMD (−46.9% and −46.9%) was similar to the reduction of those performed for retinal vein occlusion-associated macular oedema (−43.7% and −45.8%). Conversely, the reduction in injections to treat DMO was more conspicuous (−56.8% and −56.6%). Corticosteroid intravitreal injections (either for DMO or retinal vein occlusion-associated macular oedema) decreased even more than anti-VEGF injections during lockdown (−65.4% and −69.6% compared to control periods). Variability was high among different centers. Some centers lost only about 10% of the planned intravitreal therapies mainly because patients refused to travel to the hospital because of fear of infection or because patients were unable to travel through different regions. Other centers completely stopped administering intravitreal injections because of resource shortages.
Discussion
In December 2019, the novel coronavirus SARSCoV- 2 emerged in China as the cause of COVID-19. 1 According to the Italian National Institute for Health, SARSCoV-2 may have been present in Italy as early as December when the virus was found in samples of sewage water in Milan and Turin. 8 In just a matter of weeks, from the end of February to the beginning of March 2020, Italy went from the discovery of the first official COVID-19 case to a state of lockdown. However, lockdown initially occurred exclusively in the Northern regions, and only on 10 March 2020 was the lockdown proclaimed on national scale. 7 Since then, Italian public health authorities ordered physicians to visit and treat only patients with emergent or urgent conditions. In the “red zones” (i.e. the region of Lombardia, which was hit the hardest by the pandemic), the shortage of hospital beds and ventilators became a concrete threat, and health professionals from different disciplines were converted to COVID-19 patient care.21,22
Because specific guidelines for ophthalmologists were not available at that time, and because the number of COVID-19-positive cases varied highly across regions, restrictions in treating eye pathologies or in continuing to administer intravitreal injections varied among different centers. Therefore, previous studies reporting data from single referral hospitals may have not estimated accurately the impact of these different restrictions on a national scale.14,15,17
The current study reports data that were collected at 39 Italian institutional centers, which are representative of the whole country, and the results show a substantial reduction in eye surgical procedures that were performed in the 2 months after the start of the national lockdown compared to intra- and inter-year control periods (−68.8% and −69.9%, respectively). As expected, such a reduction included predominantly elective surgeries (−96.2% and −96.4%, respectively); however, urgent procedures (−49.7% and −50.2%) and intravitreal injections were also heavily affected.
During the lockdown, eye surgical activity was completely stopped at four centers. At all other centers except for one (Turin), the availability of operating rooms was limited to certain days per week or hours per day. The amount of undertreatment of urgent pathologies that was caused by this reduced availability is difficult to estimate. Our data suggest that 30% of the patients for whom an operation was recommended or an injection was planned during the lockdown period did not attend the hospital. This was because of flaws in the health care system (such as the inability to provide swab results promptly or because of the lack of supplies) in less than 1% of the cases. In the remaining cases, it was because of the patients’ fear of getting infected at the hospital or because of difficulties/fear of using public transportation or going to the hospital on their own. Local differences in the availability of resources, staff, and supplies (even within the same geographic area) may have influenced the volume of treated pathologies. This explains why in the areas of Milan and Rome (each with four Institutional centers that participated in this study), the percentage reduction of surgeries varied substantially among different centers. Other factors may have played a role. For example, it can be hypothesized that the reduction in volume of operated trauma cases (−43.6% and −32.2% compared to intra- and inter-year controls) might have been secondary to the restriction of outdoor activities that was imposed by the government during the lockdown. Furthermore, the shut-down of local hospitals and private clinics and offices may have contributed to the reduced number of “urgent” cases that were sent to referral centers. Finally, because of fear of infection and lockdown restrictions, patients may have underestimated the importance of symptoms with a consequent delay in care. For this last aspect, some considerations may be given. According to our data, during the lockdown period, surgery for RRD repair decreased significantly compared to the two control periods, with scleral buckle surgeries reducing much more than PPVs (−48.6% and −65.1% vs −23.9% and −22.0%). Usually, scleral buckling is chosen for recent-onset, macula-on, and not complicated by proliferative vitreoretinopathy (PVR) RRDs, whereas PPV is used for more severe scenarios. Thus, it might be speculated that examination of patients who were affected by RRD may have been delayed during the lockdown period, and those patients who eventually underwent surgery presented with more long-standing and PVR-complicated detachments. It is likely that similar delays affected the treatment of other vitreo-retinal pathologies such as acute vitreous hemorrhages and macular holes (about −50% and −75%, respectively in comaprison to the control periods).
For elective procedures, very few cataract surgeries (a mean of eight per center), corneal transplant, cross-linking for keratoconus, removal of silicone oil, and PPV for ERM were performed during the lockdown period. The decision to perform these “elective” surgeries was determined by the physician’s judgment based on the patient’s age, laterality of the disease, and the impact of the pathology on the quality of life. Most of these “elective surgeries” were performed in the regions where the pandemic was less severe, with only few patients affected by COVID-19. Because the health system in these regions was never under the enormous pressure that was experienced in some areas in the North, “elective” surgeries continued to be performed there, especially for patients who were at risk of legal blindness (less than 20/200 in both eyes).
Concerning intravitreal therapies, all the centers tried to perform regularly administered injections to avoid delays that would possibly cause irreversible functional worsening and to avoid difficulties in rescheduling a high volume of injections. 19 Where appropriate, scheduled appointments were maintained and new patients with significant vision loss were treated. Despite this effort, anti-VEGF injections decreased by an average of almost 50% and steroid injections reduced by almost 70% during the lockdown compared to control periods. Similar results have been reported by previous few-center or single-center based studies in Italy.14,17 It is likely that patients affected by retinal diseases requiring injections may have substantially contributed to such a high decrease by refusing treatment for several of the following reasons: age ⩾65 years; concomitant cardiovascular or pulmonary diseases; and living in a nursing home or care facility. 20 In other circumstances, the chronicity of the disease or a combination of causes may have caused cancellation or deferral of the treatment. For example, the substantial reduction of steroid injections during the lockdown period might have been secondary to the fact that steroids are preferentially administered to diabetic patients with chronic macular oedema. Diabetic patients are more vulnerable to COVID-19 and a few weeks deferral of treatment for chronic DMO may have a limited impact on the visual prognosis. Thus, it is likely that a certain number of steroid injections for DMO was deliberately postponed by the physicians.
We acknowledge some limitations of this study. First, this was a retrospective study with the limitations that are inherent to such a study design. Second, the results presented may not be completely applicable to other countries in Europe and in the rest of the world because restrictions imposed by governments and health systems during the lockdown period varied from country to country.
A strength of this study is that, to the best of our knowledge, it is the first to compare, on a national scale, the number of eye surgical procedures that were performed during the lockdown with those that were performed during two control periods. Thus, although an overall reduction in elective, urgent, and intravitreal injection procedures was expected during the lockdown period, this study provides a quantitative analysis of this reduction. Furthermore, the centers involved in the study are located in the North, Center, and South of Italy, including the two main islands. Since regional inequalities exist in Italy as far as economic resources, density of population, railway/highway networks, and infrastructures are concerned and these determinants have inevitable repercussions on efficiency and availability of supplies of local health services, the results of this study, including 39 centers located in seventeen out of the 20 Italian regions, are very representative of the global Italian situation.
We hope that the results of this study will inform physicians, administrators, and policy-makers about what the epidemic caused in Italy in terms of reduced eye surgical procedures and what the future may hold for eyecare, should Italian people endure a new period of generalized lockdown.
Footnotes
Acknowledgements
Michele Reibaldi, Paola Marolo (Eye Clinic, University of Turin, Turin)
Carlo Enrico Traverso, Michele Iester, Carlo Alberto Cutolo (Eye Clinic, San Martino Policlinic, Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health [DiNOGMI], University of Genoa, Genoa)
Claudio Azzolini, Simone Donati, Elias Premi (Department of Medicine and Surgery, University of Insubria of Varese-Como, Como)
Paolo Nucci (Department of Clinical Sciences and Community Health, University of Milan) Stela Vujosevic (University Eye Clinic San Giuseppe Hospital, IRCCS MultiMedica, Milan)
Giovanni Staurenghi, Ferdinando Bottoni, Francesco Romano (Eye Clinic, Department of Biomedical and Clinical Sciences, Luigi Sacco Hospital, University of Milan, Milan)
Francesco Bandello, Giuseppe Querques, Domenico Grosso, Enrico Borrelli, Riccardo Sacconi (Department of Ophthalmology, University Vita-Salute, IRCCS Ospedale San Raffaele, Milan)
Francesco Viola, Paolo Milella, Simone Ganci (IRCCS Ca’ Granda Ospedale Maggiore Policlinico Foundation University of Milan, Milan)
Mario R. Romano, Gabriella Ricciardelli, Davide Allegrini (Department of Ophthalmology, Humanitas Gavazzeni/Castelli, Bergamo)
Luciano Quaranta, Marco Casaluci (Department of Surgical, Clinical, Diagnostic and Pediatric Sciences, Section of Ophthalmology, University of Pavia, Pavia)
Francesco Semeraro, Davide Romano (Eye Clinic, Department of Neurological and Vision Sciences, University of Brescia)
Giorgio Marchini, Francesca Chemello, Camilla Amantea (Dipartimento DNBM, Università e Azienda Ospedaliera Universitaria Integrata di Verona, Verona)
Edoardo Midena, Rino Frisina, Elisabetta Pilotto, Raffaele Parrozzani (Department of Ophthalmology, University of Padova, Padova)
Lanzetta Paolo, Daniele Veritti, Valentina Sarao (Department of Medicine - Ophthalmology, University of Udine, Udine)
Tognetto Daniele (Eye Clinic, Department of Medical, Surgical Sciences and Health, University of Trieste, Trieste)
Massimo Busin, Francesco Parmeggiani, Katia De Nadai, Luca Furiosi (Department of Morphology, Surgery and Experimental Medicine, University of Ferrara, Ferrara)
Rodolfo Mastropasqua, Bruno Battaglia, Matteo Gironi (Institute of Ophthalmology, University of Modena and Reggio Emilia, Modena)
Stefano Gandolfi, Enrico Luciani, Paolo Mora (Ophthalmology Unit, University Hospital of Parma, Parma)
Costantino Schiavi, Patrizia Bertaccini, Alessandro Finzi, Matilde Roda (Azienda Ospedaliero-Universitaria di Bologna, University of Bologna, Bologna)
Carlo Cagini, Marco Lupidi (Department of Biomedical and Surgical Sciences, Ophthalmology Section, University of Perugia, Perugia)
Gianni Virgili, Fabrizio Giansanti, Daniela Bacherini (Department of Neuroscience, Psychology, Drug Research and Child Health, University of Florence, Florence)
Gianmarco Tosi, Elena De Benedetto (Ophthalmology Unit, Department of Medical Sciences, Surgery and Neurosciences, University of Siena, Siena)
Marco Nardi, Michele Figus, Chiara Posarelli (Ophthalmology, Department of Surgical, Medical, Molecular Pathology and of Critical Area, University of Pisa, Pisa)
Cesare Mariotti, Vittorio Pirani, Michele Nicolai (Eye Clinic, Polytechnic University of Marche, Ancona)
Stefano Bonini, Marco Coassin, Antonio Di Zazzo (Ophthalmology Department, University Campus Bio-Medico, Rome)
Stanislao Rizzo, Mariacristina Savastano, Alfonso Savastano, Gloria Gambini, Umberto De Vico (Department of Ophthalmology, Catholic University of Sacred Hearth-Foundation “Policlinico Universitario A. Gemelli”-IRCCS, Rome)
Leopoldo Spadea, Andrea Iannaccone (Eye Clinic, Policlinico Umberto I, La Sapienza University, Rome)
Carlo Nucci, Federico Ricci, Francesco Aiello, Gabriele Gallo Afflitto (Ophthalmology Unit, Department of Experimental Medicine, University of Rome Tor Vergata, Rome)
Leonardo Mastropasqua, Giada D’Onofio, Federica Evangelista, Lorenza Brescia (Ophthalmology Clinic, Department of Medicine and Aging Sciences, University G. d’Annunzio of Chieti-Pescara, Chieti)
Ciro Costagliola, Roberto dell’Omo, Mariaelena Filippelli, Pasquale Napolitano, Paolo Polisena, Nicolina Gianfrancesco, Domenico Trivisonno, Francesco Petti (Ophthalmology Clinic, Department of Medicine and Health Sciences “Vincenzo Tiberio,” University of Molise, Campobasso)
Francesca Simonelli, Settimio Rossi, Antonio Tartaglione (Eye Clinic, Multidisciplinary Department of Medical, Surgical and Dental Sciences, Università degli Studi della Campania “Luigi Vanvitelli,” Naples)
Nicola Rosa, Maddalena De Bernardo (Department of Medicine, Surgery and Dentistry, “Scuola Medica Salernitana,” University of Salerno, Salerno)
Cristiana Iaculli, Anna Valeria Bux, Giulia Maggiore (Department of Ophthalmology, University of Foggia)
Francesco Boscia, Giancarlo Sborgia, Maria Oliva Grassi (Department of Medical Science, Neuroscience and Sense Organs, Eye Clinic, University of Bari, Bari)
Vincenzo Scorcia, Giuseppe Giannaccare (Department of Ophthalmology, University of Magna Græcia, Catanzaro)
Teresio Avitabile, Guglielmo Parisi
(Section of Ophthalmology, University Hospital “Policlinico-Vittorio Emanuele,” Catania)
Salvatore Cillino, Francesco Alaimo (University Eye Clinic, Department of Biomedicine, Neuroscience and Advanced Diagnostics, University of Palermo, Palermo)
Pasquale Aragona, Alessandro Meduri (Department of Biomedical Sciences, Ophthalmology Clinic, University of Messina, Messina)
Antonio Pinna, Andrea Sollazzo (Department of Medical, Surgical, and Experimental Sciences, Ophthalmology Unit, University of Sassari, Sassari)
Enrico Peiretti, Emanuele Siotto (Department of Surgical Sciences, Eye Clinic, University of Cagliari, Cagliari)
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RdO: none; MF: none; GV: none; FB advisor for Alcon, Alimera Sciences, Allergan (AbbVie), Bayer, Fidia-Sooft, Novartis, Ntc, Roche, Sifi, ThromboGenics, Topcon, Zeiss; GQ: advisor for Alimera Sciences, Allegro, Allergan, Amgen, CenterVue, KBH, Lumithera, Nevacar, Sandoz, consultant for Bausch & Lomb, Bayer Healthcare Pharmaceuticals, Heidelberg Engineering, Novartis, Roche, Sifi, Sooft/Fidia, Topcon, Thea, Zeiss; PL: advisor for Allergan, Bayer, Centervue, Novartis, Roche; TA: none, FV: advisor for Roche, Novartis, Bayer, Genentech, MR: none, FS: none, LQ: none, SR: none; EM: none, CC: none.
Francesco Bandello and Giuseppe Querques confirm they are, respectively, the editor in chief and an associate editor of this journal and were not involved in the peer review process of this paper. Paolo Lanzetta and Stanislao Rizzo confirm they are editorial board members of this journal and were not involved in the peer review process of this paper.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.