
Abstract
Purpose:
Pythium insidiosum causes a rare sight-threatening keratitis and is a devastating ocular pathology with a high morbidity. It is frequently mistaken as fungal keratitis. Here we highlight a rare case of pediatric Pythium insidiosum keratitis which was successfully managed using an antibiotic combination of linezolid and azithromycin with cyanoacrylate glue.
Case description:
A 9-year-old young male child presented to our clinic with defective vision, pain, redness in the right eye for 5 days post stick injury. In the right eye, Snellen’s best-corrected visual acuity (BCVA) was 6/12 which deteriorated to hand movements within 5 days of treatment. Ocular examination revealed 6 × 5 mm dry-looking mid stromal corneal infiltrate with feathery margin involving the visual axis. The clinical picture was suggestive of fungal keratitis. Corneal scraping and smear examination with 10% KOH and Gram stain revealed long slender hyaline hyphae with sparse septations. Before the culture result, the patient was started on 5% Natamycin and 1% Itraconazole hourly, but still, the infiltrate progressed. Further, P. Insidiosum keratitis was considered as the differential, which was confirmed on blood agar culture. After receiving culture results, the patient was managed with 0.2% Linezolid and 1% Azithromycin hourly. Due to the rapid progression of infiltrate, corneal melt, and younger age, cyanoacrylate glue, and bandage contact lens were used. On the last follow-up, the BCVA recovered to 6/12.
Conclusion and importance:
Prompt diagnosis, clinical awareness, and a specific treatment regime is needed for managing this devastating corneal entity. Cyanoacrylate glue due to its antibacterial properties can be a potential rescuer and can be considered for managing these cases.
Introduction
Pythium insidiosum is a filamentous parasitic oomycete belonging to the genus Pythium of family Pythiaceae and is mostly seen in aquatic habitats. The fungi like oomycete live in soil and water in tropical, subtropical, and temperate climates. 1 It is still a diagnostic dilemma for the majority of the clinicians, and in non-endemic areas, it is often misdiagnosed as unidentified fungal keratitis cases. 2 There has been a recent upsurge of cases in the past 4–5 years and numerous studies have been published on similar literature.2,3 The first case report of human pythiosis dates back to 1985 from rice workers in Thailand 4 where it was considered to be endemic. 1 Hasika et al. 2 in their retrospective analysis reported a prevalence of 5.9% (71/1204) of Pythium keratitis cases. Similarly, Sharma et al. 5 in their analysis reported a prevalence of P. insidiosum among unidentified fungal isolates to be 5.5% (9/162) in phase 1. In phase 2, 4/102 cases (3.9%) of fungal keratitis were identified as P. insidiosum. In contrast to fungus the cytoplasmic membrane lack ergosterol, and the organism exhibits asexual reproduction through the formation of sporangia containing zoospores. 1 It is well known that Pythium keratitis closely mimics fungal keratitis and often misdiagnosed based on slit-lamp evaluation and corneal scrapings. 6 This is the probable reason why we were missing a major chunk of Pythium cases 4–5 years ago. The various risk factors include injury with dust, dirty water, vegetative matter, insect fall, and clay injury. On slit-lamp evaluation 7 the classical clinical features are dense grayish- cotton wool-like white infiltrates with feathery extension, hyphate edges with filamentous lesions, tentacular projections, and peripheral furrowing resembling that of filamentous fungi. In addition, on histopathological staining and confocal microscopy 8 filaments closely resembling fungus. When such clinical features are noted in a patient who is not responsive to conventional antifungal drugs, the possibility of P. insidiosum as the primary causative agent should be considered. Human Pythium exists in four different clinical forms – ocular, vascular, disseminated, and subcutaneous or cutaneous form. 2 Compared to other forms, ocular pythiosis has extremely poor prognosis. It primarily causes keratitis in the eye. 3 Owing to lack of ergosterol in their cell wall, and it is unresponsive to antifungal drugs. 7 Moreover, definitive microbiological identification is characterized by zoospores formation and when spore formation is absent, DNA sequencing is a must for identification. 5 The various medical treatment options available are antifungal drugs (Natamycin, Itraconazole, Voriconazole, Ketoconazole, Amphotericin B, and Terbinafine), 2 and antibacterial drugs (Linezolid, Azithromycin, Tigecycline, and Tetracyclines), 3 surgical treatment include Therapeutic and Tectonic Penetrating Keratoplasty(TPK) and non-resolving cases having scleral involvement, endophthalmitis, and pan-ophthalmitis requiring enucleation or evisceration. 2 Hasika et al. 2 in the retrospective case series proved that Therapeutic Keratoplasty has a better outcome compared to conservative management with antifungals. Bagga et al. 3 in their prospective trial showed that in vitro activity of antibiotics such as tigecycline, minocycline, and azithromycin, was found to be effective compared to conventional antifungals. After a detailed literature review and as per the best of our knowledge, none of the previously published literature has highlighted the use of cyanoacrylate glue as a management option for Pythium Keratitis. This report highlights a rare case of an Indian child with vision-threatening Pythium Insidiosum keratitis who was successfully managed with linezolid, azithromycin, and cyanoacrylate glue.
Case report
A 9-year-old young boy presented to our clinic with complaints of pain, redness, and defective vision in the right eye (OD) since 5 days post stick injury. There was a history of use of some eye drops taken from a local chemist shop for 2 days. Snellen’s best-corrected visual acuity was 6/12 on presentation. The intraocular pressure in the left eye (OS) was 14 mmHg and OD was not recordable. Slit-lamp biomicroscopic examination in OD revealed conjunctival congestion, 3 × 3 mm dry looking mid stromal corneal infiltrate with feathery margin involving visual axis, stromal edema, and normal anterior chamber depth with no hypopyon (Figure 1(a)). The clinical picture was suggestive of fungal keratitis. Corneal scraping and smear examination with 10% KOH and Gram stain revealed long slender hyaline hyphae with sparse septations (Figure 1(c)). Before culture results were available the patient was started on topical antifungals 5% Natamycin hourly and 1% Itraconazole hourly, cycloplegic topical Homatropine 2.5% BD, oral anti-inflammatory Diclofenac 200 mg BD for 3 days and the ulcer worsened. The visual acuity deteriorated to hand movements close to the face (HM+) within 5 days of treatment and infiltrate progressed to 6 × 5 mm. Hence, P. Insidiosum keratitis was considered as a differential, which was confirmed with the zoospore (Figure 1(d)) formation on blood agar culture (leaf incarnation method) (Figure 2)}. After culture results, the patient was managed with antibacterials topical 0.2% Linezolid hourly and 1% Azithromycin hourly. Due to the rapid progression of infiltrate, early corneal melt, and younger age group, cyanoacrylate glue, and bandage contact lens were used (Figure 1(b)). At 2 weeks follow-up, signs of healing were present and visual acuity improved to 5/60. On the last follow-up at 1 month, the BCVA recovered to 6/12. The timeline of intervention and outcome has been depicted in the Figure 3.
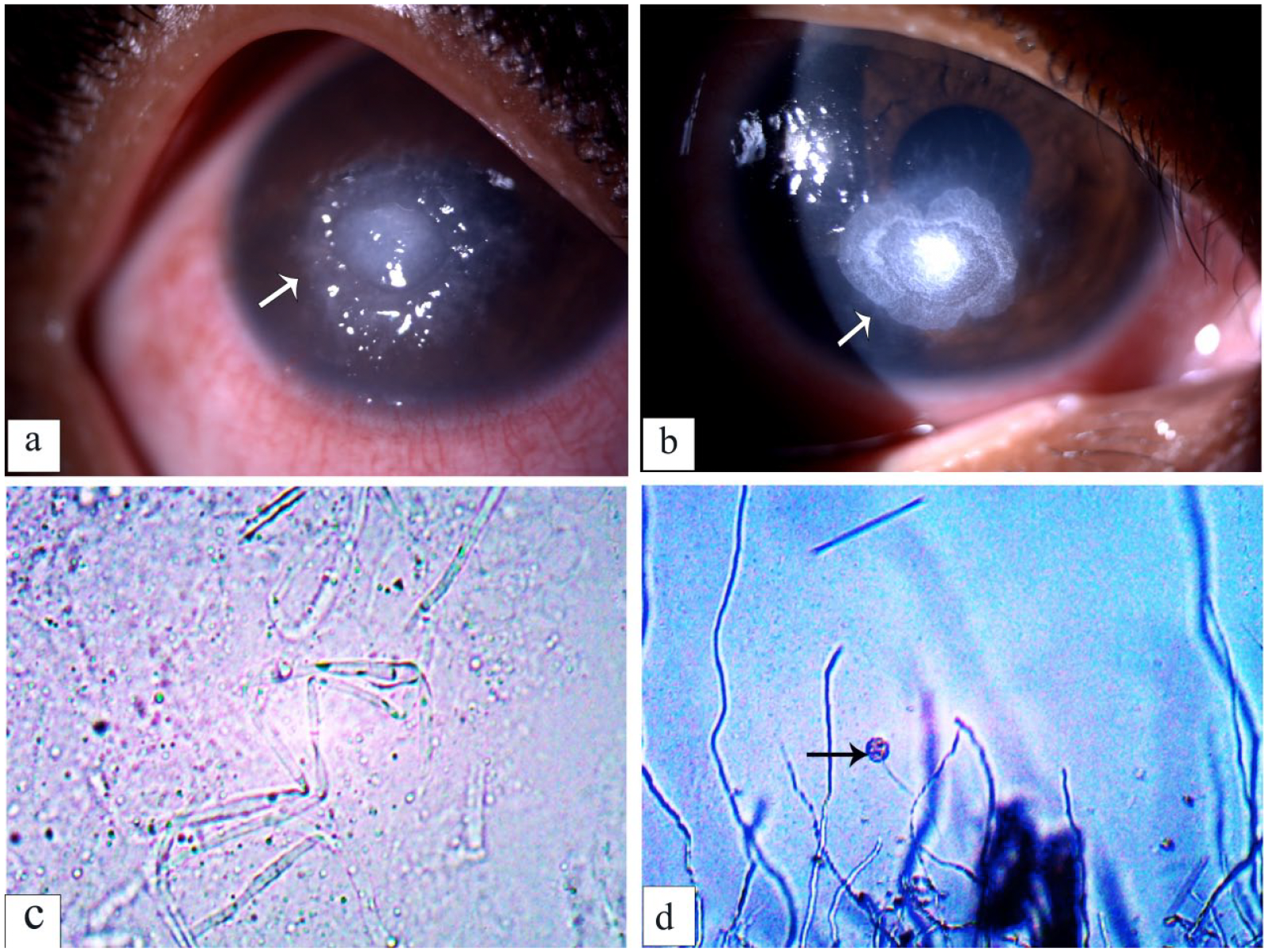
(a) Image of the right eye of the patient depicting 5 × 5 mm mid stromal infiltrate with tentacular projections and peripheral furrowing, (b) image of the right eye of the patient post cyanoacrylate glue application with corneal scarring, (c) a 10% KOH wet mount of corneal scraping depicting long slender hyaline hyphae of Pythium insidiosum with sparse septations. Numerous vesicles within the hyphae are usually observed, and (d) a vesicle containing zoospores that formed after 3 h incubation before zoospore release (×10) using cultured leaf incarnation method.

Five percent Sheep blood agar culture (fifth day) of P. insidiosum at 37°C.
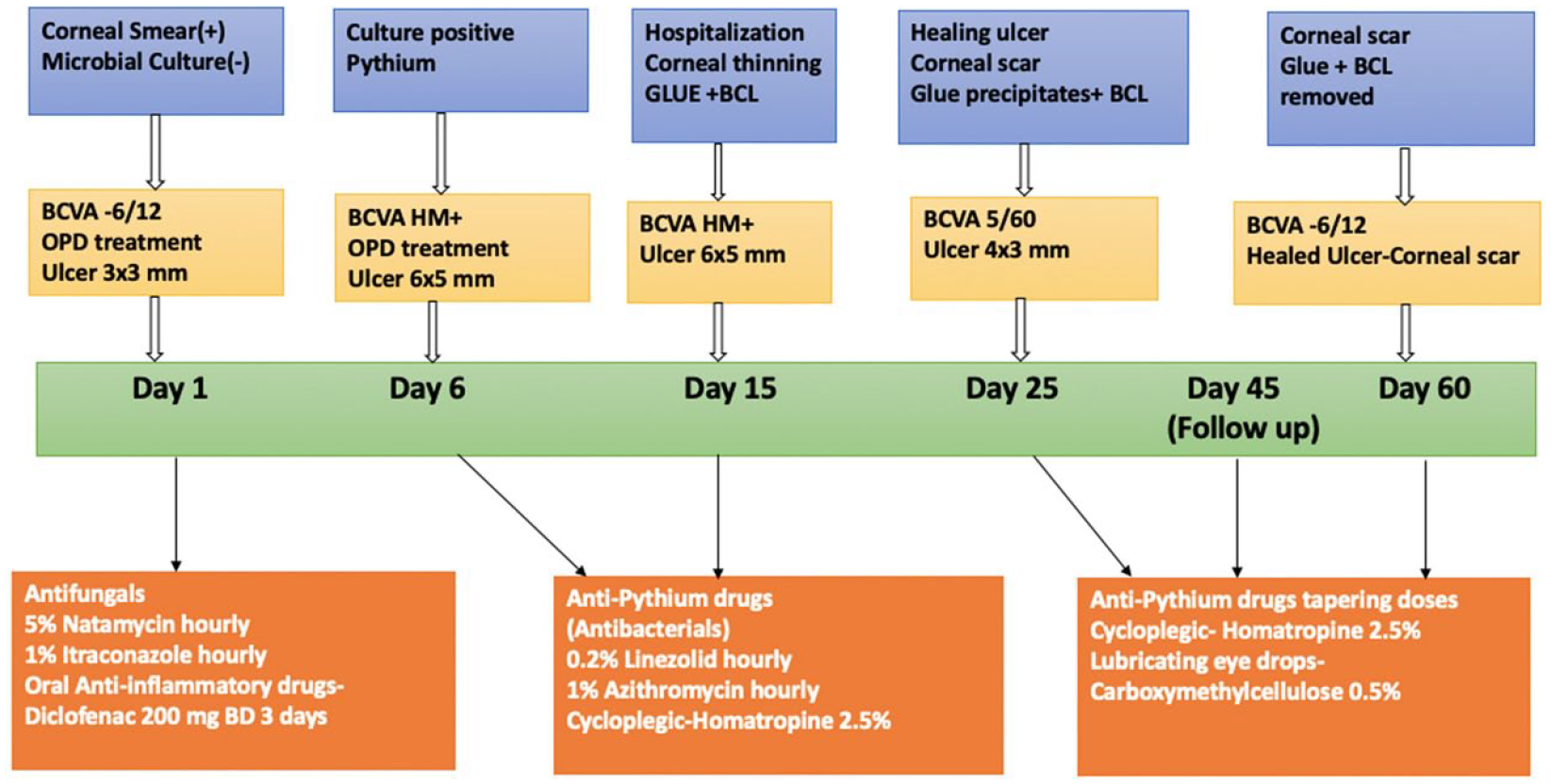
Flowchart – timeline of interventions and outcome.
Discussion and conclusion
P. insidiosum exhibits mycelial growth on agar media and is commonly misdiagnosed and treated as a fungal keratitis. 1 It closely mimics algae more than fungi and initially cutaneous granulomas and arteritis were the most common reported systemic infection. 2 With high mortality and morbidity, it had added to the burden of infective keratitis in the world necessitating TPK in the majority cases.2,3 Increased knowledge of the organism’s appearance on smears (KOH and Gram stain), colony characteristic, zoospore identification, and nucleic acid sequencing information have aided in more accurate diagnoses earlier in the course of the disease, however there is still a deficit in strategies for treating the infection.5,8
Currently, there are no standard treatment guidelines for Pythium keratitis, and recently in vitro and in vivo susceptibility tests has demonstrated the application of antibacterial drugs for this pathogen. Ramappa et al. 7 depicted the successful management of P. insidiosum keratitis using a triple-drug regimen of atropine, azithromycin, and linezolid. Similarly, Maeno et al. 9 also highlighted successful resolution of Pythium keratitis using a triple-drug therapy of linezolid, chloramphenicol, and minocycline. Few of the earlier clinical reports have demonstrated the neck-to-neck comparisons of antibacterial and antifungal therapy for Pythium. A combined regimen of topical azithromycin and linezolid is considered superior to topical natamycin, which indicate better response of P. insidiosum to antibacterial agents. 3 Romero et al. 10 concluded that the polymerization reaction is related to the efficacy of cyanoacrylate tissue adhesives. Therefore, shorter alkyl-chain adhesives with their strong antibacterial properties can be used in severe or recalcitrant gram-positive bacterial corneal ulcers as an adjuvant to topical antibiotics. This antibacterial effect may be an added advantage in patients with melting or perforation when glue is use to salvage the cornea.
Our rationale for using antibacterial drugs was based on information available in the published literature. In our case, we used topical linezolid and topical azithromycin after culture confirmation of zoospores of pythium. Further, we used cyanoacrylate glue and bandage contact lens because of progressive thinning and corneal melt. Although keratoplasty is the proposed treatment in majority of the cases, considering the age of the child, salvaging vision, and the corneal tissue was our major goal. The Keratoplasty was best delayed until the organism was eradicated. The use of cyanoacrylate glue is well known in bacterial, fungal, and other infective keratitis. But, as per the best of our knowledge, none of the previous published reports have reported use of glue as an adjuvant for Pythium keratitis. This is the first report of successful management of pediatric pythium using antibacterials and cyanoacrylate glue with excellent visual outcomes. The glue having antibacterial properties have an additive effect on the proposed antibacterial treatment. 10
Importance
Prompt diagnosis, clinical awareness and specific treatment regimen is needed for managing this devastating corneal entity. Here we highlight a rare case of pediatric Pythium insidiosum keratitis who was successfully managed with antibacterials like 0.2% Linezolid, 1% Azithromycin, and cyanoacrylate glue. The patient showed rapid resolution with glue due to additive antibacterial properties. Thus, treating clinicians should be aware that glue can be used as an adjunct to anti-pythium drugs for treating this devastating ocular infection with good visual outcomes.
Footnotes
Acknowledgements
Aravind Eye Hospital and Post Graduate Institute of Ophthalmology, Cuddalore main road, Thavalukuppam, Pondicherry, India, 605007.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
Appropriate informed consent was obtained from the patient for sharing his/her medical information for study, research and publication purpose.