
Abstract
Purpose:
This study aimed to evaluate the relationship between diabetic iridopathy (DI) and diabetic retinopathy (DR) and distinguish iris neovascular and physiological leakage using iris fluorescein angiography (IFA).
Methods:
A total of 210 subjects were prospectively recruited in this study. Sixty normal subjects were divided equally into three groups (<40 years old, 40–59 years old, and 60–79 years old). One hundred fifty patients with diabetic mellitus (DM) were divided equally into five groups (no retinopathy, mild non proliferative DR (mildnPDR), moderate nPDR, severe nPDR, and PDR group). Normal subjects underwent IFA. Patients with DR underwent both IFA and ultrawide field fundus fluorescein angiography (uwFFA) at the same time. The leakage time and area were recorded and compared with each group.
Results:
Fluorescein leakage occurred at the pupillary edge of patients that were 40–59 and 60–79 years old but not in those <40 years old. In the PDR group, the leakage time was earlier and the leakage area was larger than nPDR and patients with no retinopathy (p = 0.039 and p = 0.005, respectively). However, the leakage time and area were not significantly different between patients with no retinopathy and nPDR (p > 0.05).
Conclusion:
IFA examination can only assist in estimating the fundus severity of PDR patients, whereas the fundus changes of patients with no retinopathy and nPDR were not related to DI changes.
Trial registration No.: ChiCTR1800018003.
The date of registration: Aug 26th, 2018.
Keywords
Introduction
Diabetic retinopathy (DR) is a common microvascular abnormality in the retina of patients with diabetes. Almost all patients with type I diabetes and 60% of patients with type 2 diabetes would develop retinopathy after suffering from diabetes 20 years later. 1 In patients with diabetes, the whole vasculature of the eye can be affected by microangiopathy. Diabetic iridopathy (DI) and DR are the two most severe complications. The high risk of neovascular glaucoma after vitrectomy 2 and cataract extraction 3 in patients with diabetes is well-known. This means that the abnormalities in the iris and retina must be carefully examined before surgery to avoid severe complications. However, DR is not easily found due to the opacity of dioptric media, such as in vitreous or preretinal hemorrhage and metabolic cataract.
In order to assess the foggy fundus condition in patients with DR, the relationship between DI and DR needs to be confirmed. So far, this relationship has not been clearly reported. Previous studies have shown that iris fluorescein angiography (IFA) is the most effective way to assess iris diabetic microangiopathy, and hence, to make an indirect evaluation of DR. 4 Other studies have shown that the absence of DI did not exclude the presence of DR. 5 Therefore, how DI indicates the presence of DR remains unclear. Moreover, iris leakage occurs with the increase in the age of normal people; it is also known as physiologic leakage. It is also essential to distinguish new blood vessel leakage from physiological leakage to determine the relationship between DI and DR. With the advancement in technology, ultra wide field fundus fluorescein angiography (uwFFA) has been widely applied in the diagnosis and treatment of DR, which provides a clearer wide-angle fundus image. Therefore, this study aimed to assess how DI indicates the presence of DR and determine how to distinguish new blood vessel leakage from physiological leakage using IFA and uwFFA.
Methods
This is a prospective cross-sectional study. Patients with diabetic mellitus (DM) were recruited from our out-patient department between January 2017 and January 2019. The exclusion criteria were the following: topical myotic therapy; previous laser or anti-VEGF therapy; previous ocular surgery; and other ocular disorders or systemic diseases, such as retinal detachment, glaucoma, hypertension, and immune. This study was approved by the institutional review board of Tianjin Medical University, and the protocols adhered to the tenets of the Declaration of Helsinki.
A total of 210 subjects were recruited in this study. Sixty subjects were normal people and divided equally into three groups: <39 years old, 40–59 years old, and 60–79 years old. Depending on the DR severity scale classification, 6 150 subjects with DM were divided equally into five groups: no retinopathy group, mild non proliferative diabetic retinopathy (mild nPDR) group, moderate nPDR group, severe nPDR group, and PDR group. The clinical characteristics of all subjects are summarized in Table 1. All patients were provided with informed consent for being involved in this study.
Demographic characteristics in normal subjects and diabetes patients.
The subjects underwent complete ocular examinations, including slit-lamp, uwFFA, ultra wide field color fundus photographs (Optos Panoramic 200), and IFA (FA; Spectralis HRA, Helderberg engineering, German). To compare the iris and fundus angiogram, we arranged a new approach to perform uwFFA and IFA at the same time. At the start of the examination, fluorescein was injected intravenously. A 5-mL dose of 20% fluorescein solution was used; the patient’s pupils did not dilate. IFA was performed in the early phase for 1 min using Spectralis HRA angiography. Then, uwFFA was performed using Optos Panoramic 200 for the next 1–3 min. After that, IFA was recorded continuously in the late phase for 15 min using the Spectralis HRA angiography. Fundus photographs were graded by a retina specialist (ZL) using the standard PDR classification. 7 Retina and iris angiogram evaluations were carried out separately by two different retina specialists (KY and ZL). The degree of leakage areas in the pupillary margin were calculated using a specially designed ruler (Figure 1). Retinal angiograms were double-checked to confirm the grading assessed from fundus photographs.
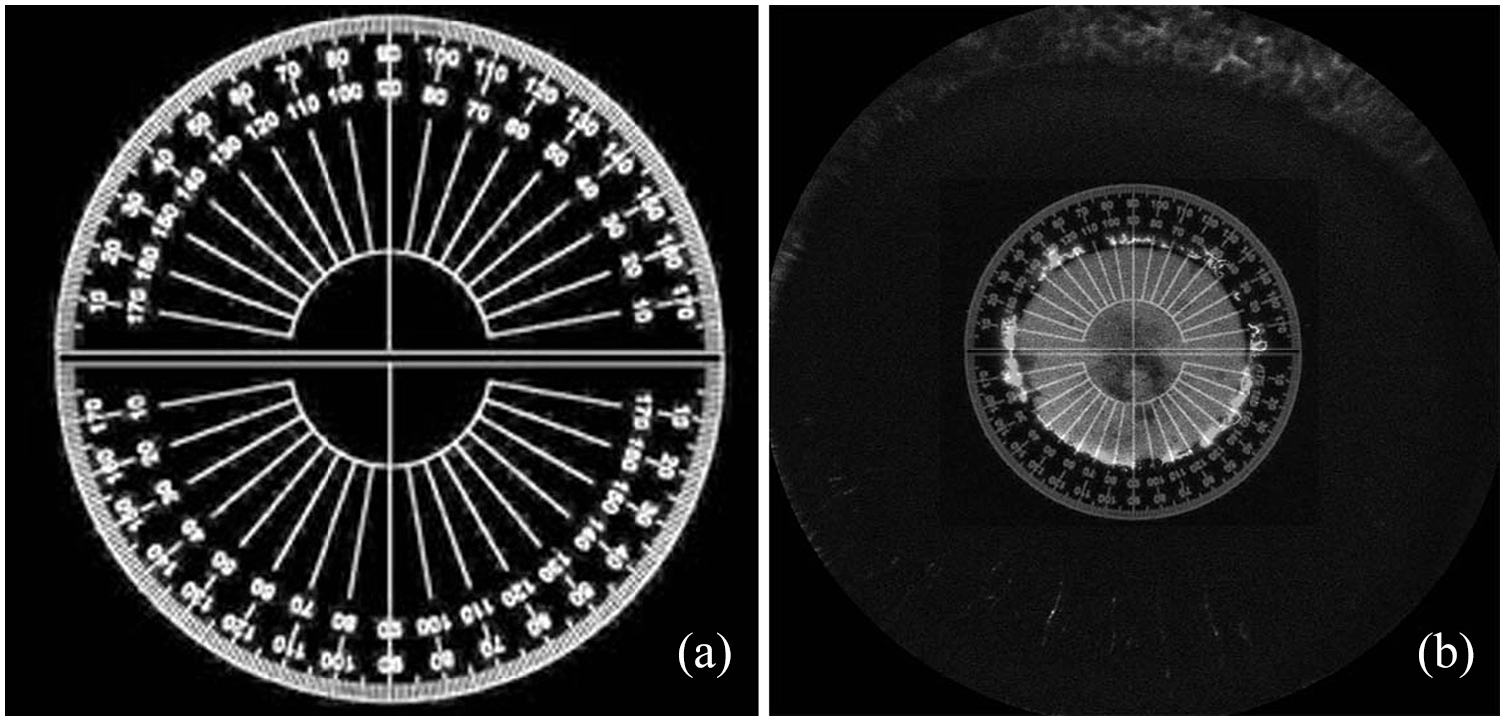
(a) The 360° ruler, (b) the leakage area degree on the papillary margin was calculated with 360° ruler.
DI was classified according to previous studies. 4 Briefly, the absence of DI (no DI): fluorescein leakage is absent in late phases; non proliferative DI (NPDI): the hyperfluorescence tends to diminish and disappear rapidly after the fluorescein passed through; proliferative DI (PDI): neovascularization exists in the pupillary margin, filling rapidly, and leaking promptly and diffusely; and neovascular iris (NVI): with newly formed blood vessels on the iris surface and at the anterior chamber angle.
Statistical analysis
All data were expressed as the means and standard deviations and were analyzed using the SPSS software (version 17.0; SPSS Inc, Chicago, IL, USA). One-way ANOVA was used to compare the leakage time and area among the different groups. A p value < 0.05 was considered significant.
Results
Demographic characteristics
In 60 normal subjects, the average age was 49.37 ± 8.54 years old, 25 (42%) subjects were male, and 35 (58%) subjects were female. The right eye was the only one examined. In 150 patients with DM, the average age was 58.07 ± 8.67 years old, 84 (56%) subjects were male, and 66 (44%) subjects were female. The right eye was involved in 80 (53%) patients, whereas the left eye was involved in 70 (47%) patients. All demographic characteristics are shown in Table 1.
More specifically, in the no-retinopathy group, 21 patients had no DI, nine had NPDI, and none had PDI or NVI. In the mild nPDR group, 18 subjects had nPDI, 12 had PDI, and none had NVI. In the moderate nPDR group, 16 patients had nPDI, 14 had PDI, and none had NVI. In the severe nPDR group, nine patients had nPDI, and 21 had PDI. In the PDR group, 22 patients had PDI and eight had NVI (Table 2).
Relation between diabetic iridopathy (DI) groups and diabetic retinopathy (DR) groups (%).
No DR = absence of DR; nPDR = none proliferative DR; PDR = proliferative DR.
No DI = absence of DI; NPDI = non-proliferative DI; PDI = proliferative DI; NVI = neovascular iris.
IFA results among the normal subjects
In the 60–79 years old group, fluorescein leakage occurred in 11 subjects. The fluorescein leakage was found on the pupillary margin 40.13 ± 2.23 s after fluorescein injection, and the leakage area was 13.5° ± 9.75°. Whereas in the 40–59 years old group, seven subjects had fluorescein leakage 39.22 ± 2.49 s after fluorescein injection, and the leakage area was 18.18° ± 18.43°. This iris leakage had features that became larger and brighter in the early phase and disappeared quickly during the late phase after fluorescein injection (Figure 2). No patient in the 20–39 years old group had iris leakage; therefore, we did not compare the 20–39 years old group to the other groups. The leakage time and area of the three groups are shown in Table 3.
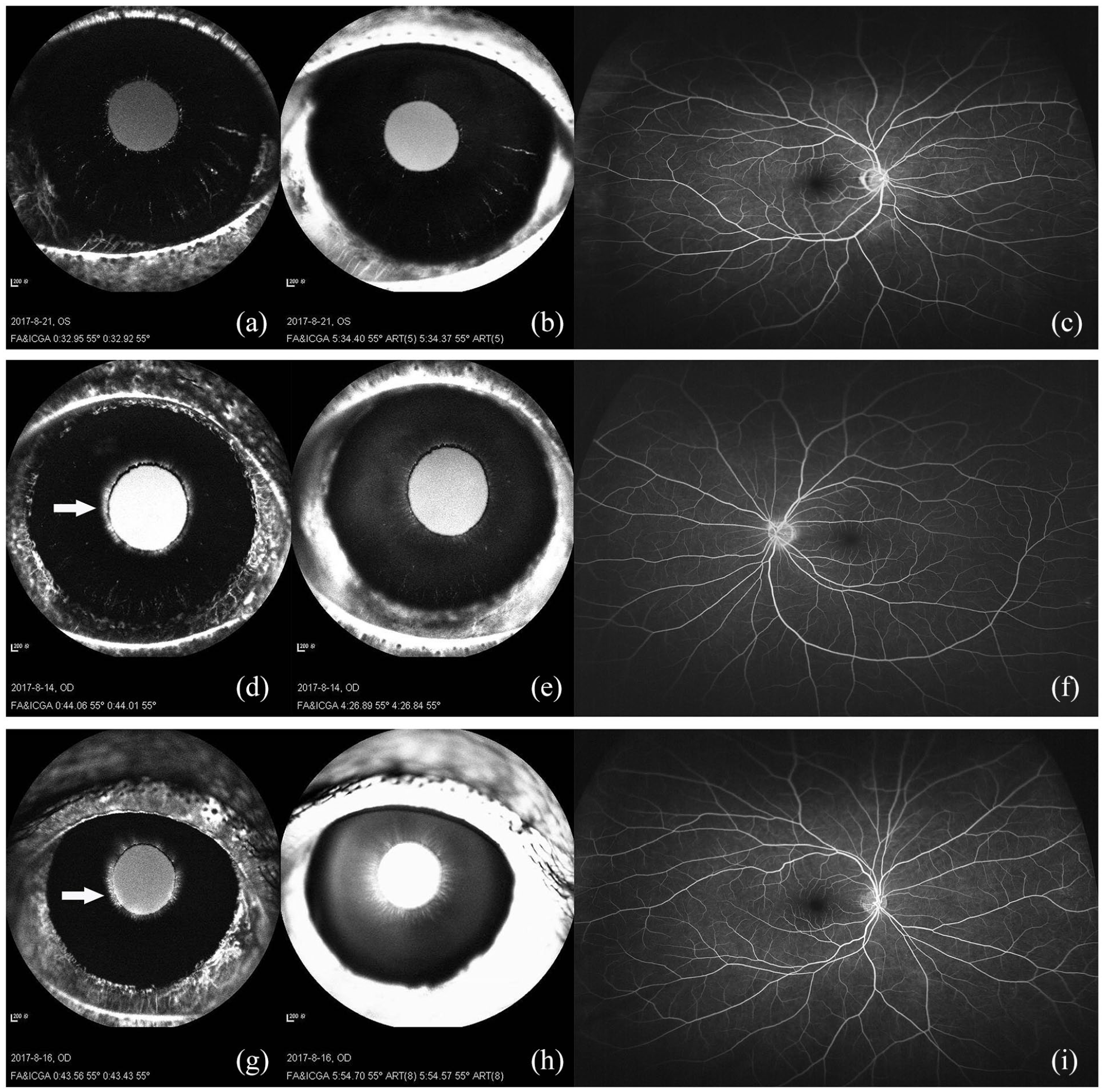
IFA and UWFFA imaging in normal people: (a–c) 30–49 years old group. no fluorescein leakage in iris, (d–f) 40–59 years old group, slight fluorescein leakage started in iris around 40 s (arrow) and leakage disappeared quickly around 5 min, (g–i) 60–79 years old group. Slight fluorescein leakage started in iris around 40 s (arrow) and leakage slightly retained around 5 min.
Fluorescein leakage time and area of normal subject groups and DR groups.

DR: diabetic retinopathy; NA: not applicable; nPDR: non-proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy.*: Eight PDR patients with NVI did not include in the calculation of leakage time and area.
IFA results among the patients with DM
The intraocular pressure in all patients with DM as normal. Approximately 26 (90%) patients with no retinopathy, 80 (88%) patients with nPDR, and 30 (100%) patients with PDR showed iris fluorescein leakage. Totally eight patients with PDR had NVI on the surface of the iris stroma. Owing to the different leakage location, eight patients with PDR with NVI were not involved in our leakage area statistical analysis. The leakage times in the no retinopathy, nPDR, and PDR groups were 29.89 ± 4.14, 30.38 ± 6.40, and 25.87 ± 5.42 s, respectively. The leakage areas in these three groups were 36.67° ± 48.15°, 49.09° ± 59.27°, and 137.71° ± 95.53°, respectively (Table 3).
Multiple comparisons of leakage time and area between the groups
According to multiple comparisons in different age groups, the average leakage time and area in the 60–79 years old group were not significantly different (p = 0.712 and p = 0.795, respectively) from the 40–59 years old group; no iris leakage was found in the 20–39 years old group. This indicated that physiologiciris leakage will increase with age. According to multiple comparisons in patients with DM, the leakage time was significantly earlier and the leakage area was significantly larger in the PDR group compared to the no-retinopathy group (p = 0.039 and p < 0.001, respectively) and nPDR group (p = 0.005 and p < 0.001, respectively). However, the leakage time and area were not significantly different between the no retinopathy and nPDR groups (p = 0.817 and p = 0.591, respectively) (Table 4).
Multiple comparisons of leakage time between the participant groups.

DR: diabetic retinopathy; No.: number; nPDR: non-proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy.
In multiple comparisons between the normal people and patients with DM, the average leakage time in the 60–79 and 40–59 years old groups was significantly different from the three DM groups (all p < 0.001). This indicated that neovascular iris changes in normal people and patients with DM can be distinguished by iris fluorescein leakage time. However, the average leakage area in the 40–59 and 60–79 years old groups was not significantly different from the no retinopathy group (p = 0.324 and p = 0.062, respectively) and nPDR group (p = 0.424 and p = 0.081, respectively). Only the average leakage area in patients with PDR was significantly different from the normal people (p < 0.001 and p < 0.001, respectively). This indicated that the iris leakage area can only be used to distinguish patients with PDR from the other groups (Table 4).
IFA results among three diabetic retinopathy groups
Patients with nPDR were divided into mild, moderate, and severe nPDR groups according to fundus photograph and uwFFA (Figure 3). The leakage time in the mild, moderate, and severe nPDR groups were 33.00 ± 8.96, 34.66 ± 8.38, and 35.38 ± 9.58 s. The leakage areas in the three groups were 51.25° ± 68.96°, 58.33°+64.00°, and 62.50° ± 61.12°, respectively. The leakage time and area in the PDR group were 26.50 ± 5.41 s and 137.71° ± 95.53°, respectively (Figure 4; Table 5).
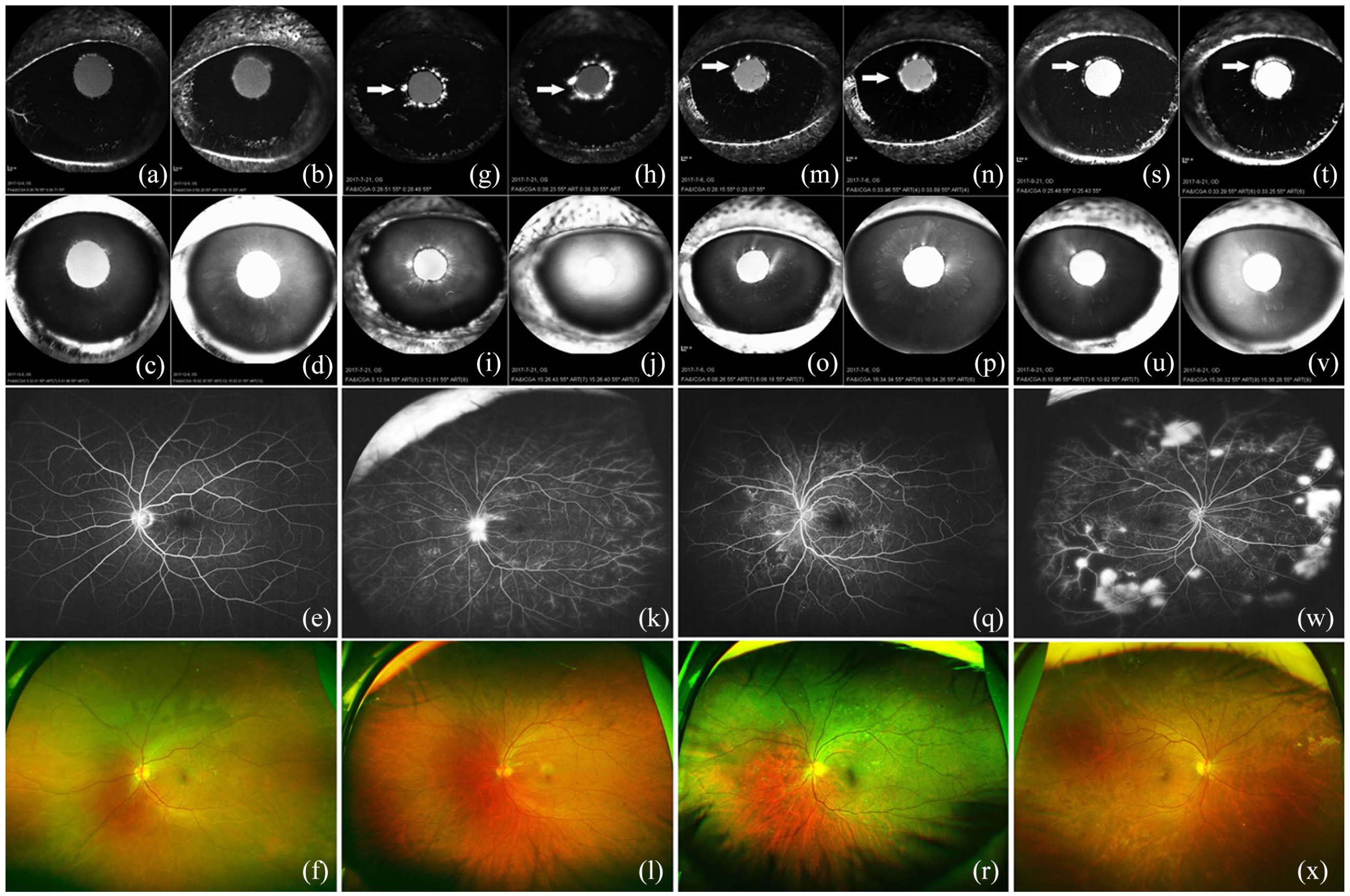
IFA and UWFFA imaging in nPDR patients: (a–f) no retinopathy group, (g–l) mild nPDR group, IFA showed fluorescein leakage started in iris around 30 s (arrow) and fluorescein still retained after 5 min. FFA showed numerous microaneurysms. (m–r) moderate nPDR group, IFA showed fluorescein leakage started in iris around 30 s (arrow) and fluorescein still retained after 5 min. FFA showed numerous microaneurysms and non-perfusion area. (s–x) severe nPDR group, IFA showed fluorescein leakage started in iris around 30 s (arrow) and fluorescein still retained after 5 min. FFA showed non-perfusion area and peripheral blood vessel leakage.
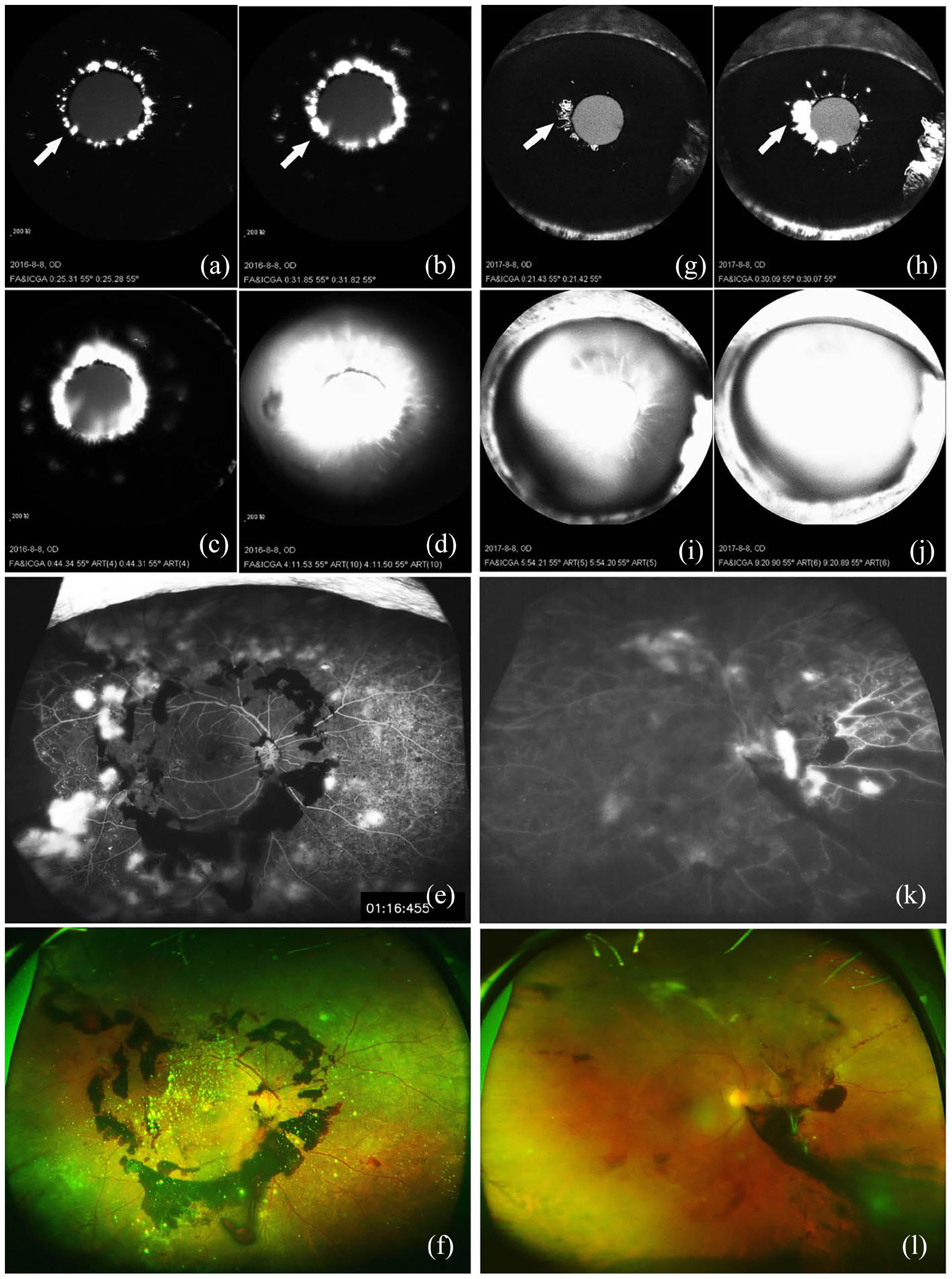
IFA and UWFFA imaging in PDR patients: (a–f) PDR patient with pupil margin leakage only. IFA showed fluorescein leakage started in iris around 25 s (arrow) and hyperfluorescein retained after 5 min. FFA and fundus photograph showed preretinal hemorrhage. (g–l) PDR patient with NVI. IFA showed fluorescein leakage started in iris around 20 s (arrow) and hyperfluorescein retained after 5 min. FFA and fundus photograph showed vitreous hemorrhage.
Comparison of leakage time or area between NPDR and PDR groups divided according to FFA foundings.
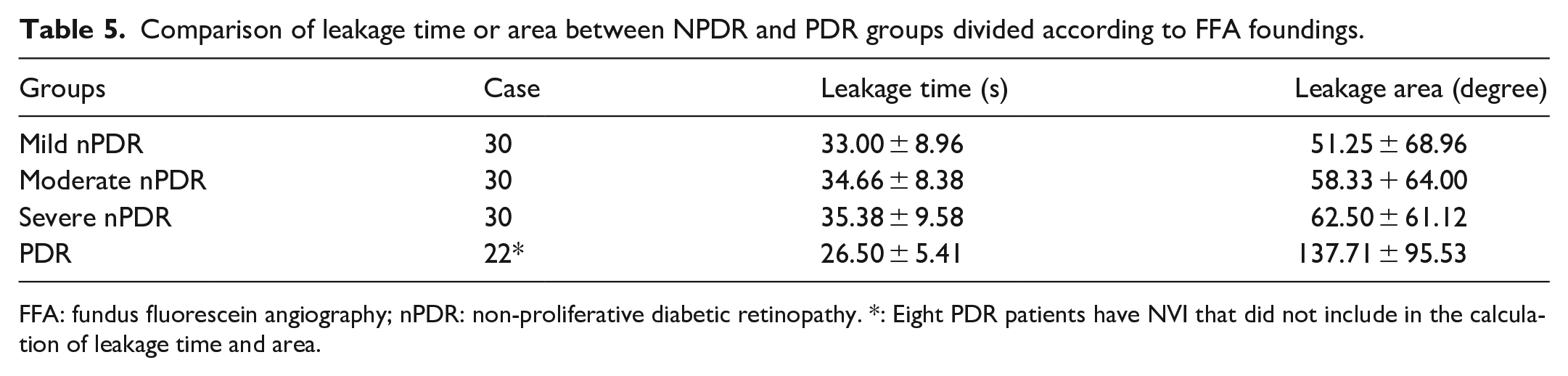
FFA: fundus fluorescein angiography; nPDR: non-proliferative diabetic retinopathy. *: Eight PDR patients have NVI that did not include in the calculation of leakage time and area.
Multiple comparisons of leakage time and area between the three diabetic retinopathy groups
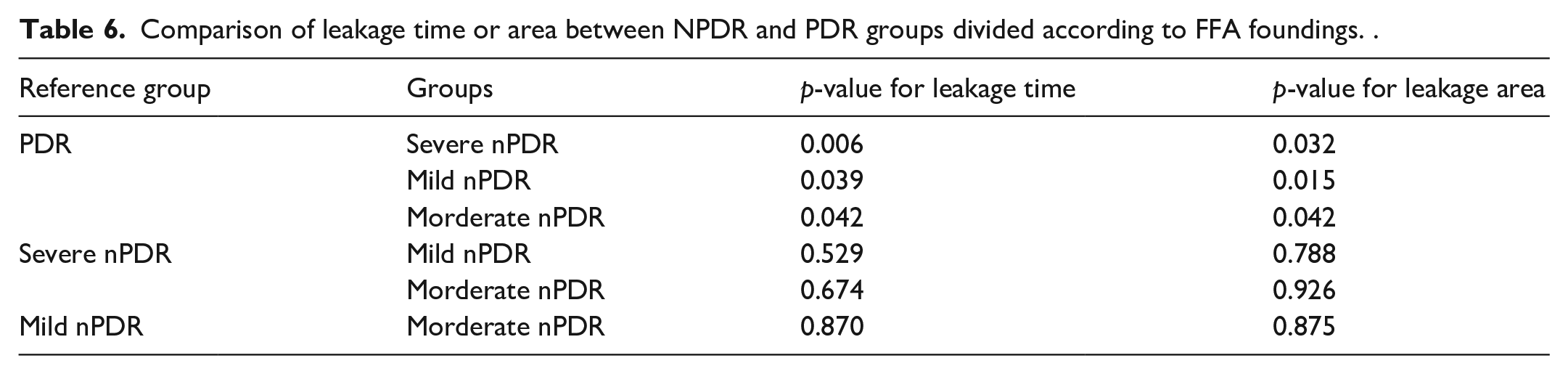
Based on the multiple comparisons, the leakage time and area of the three nPDR groups were not significantly different (p > 0.05). The leakage time and leakage area in patients with PDR were significantly different from mild (p = 0.039 and p = 0.015, respectively), moderate (p = 0.042 and p = 0.042, respectively), and severe nPDR (p = 0.006 and p = 0.032, respectively; Table 6). This result revealed that IFA can only hint new blood vessel changes in the retina of the PDR group.
Comparison of leakage time or area between NPDR and PDR groups divided according to FFA foundings. .
Discussion
It is difficult to distinguish normal iris leakage from new blood vessel leakage in IFA examination. According to this study, slight fluorescein leakage occurred at the pupillary edge of older subjects, but fluorescein leakage did not appear in young subjects. This indicated that aging could influence the physiological leakage in the iris of normal people. Moreover, fluorescein leakage at the pupillary edge of normal elderly people was dim; it slowly enlarged in the early phase and disappeared quickly after the fluorescein passed through the retinal blood vessel. New blood vessel leakage rapidly and persistently diffused into the anterior chamber, resulting in hyperfluorescence at the late phase. This demonstrated that normal iris leakage can be distinguished from new blood vessel leakage according to different leakage characteristics. The iris physiological leakage was speculated to be weak tight junctions in iris vascular endothelial cells. 8 Along with aging, the iris vessels aged and the tight connection slightly slacked. The fluorescein in iris vessels slowly leaked and disappeared quickly. This result is consistent with previous studies on the light-colored iris of caucasians. 9
This study also found that leakage times in normal elderly people groups were significantly different from the DM groups, which was about 10 s delayed than patients with DM. This indicated that iris neovascularization leakage was more rapid than physiological leakage. This characteristic of IFA could be used to distinguish iris neovascularization leakage from aging blood vessel leakage.
To determine whether DI is correlated with DR, previous studies showed that the presence of DI was significantly correlated with the presence of DR in varying degrees of severity. 4 However, during this study, no difference was observed in the IFA leakage area between all nPDR groups and the no-retinopathy group, whereas only the IFA leakage area inpatients with PDR was significantly different from the other DM groups. It is well-known that the retinal impairment in patients with mild, moderate, and severe nPDR gradually progress, but the iris leakage area in our study did not increase with progressing DR. Therefore, neovascular changes in the iris were not correlated with the fundus of patients with nPDR through the IFA. Alternatively, the IFA leakage areas in patients with PDR developed quicker and larger than in the nPDR groups. This result demonstrated that new blood vessel changes in the iris were consistent with the severely damaged retina in patients with PDR. Hence, IFA can only reveal retinal neovascular changes in patients with PDR, but not in other patients with DR. In addition, no patients with nPDR had NVI, whereas 27% of patients with PDR had NVI. This indicated that patients with nPDR will not have NVI until DR progress to PDR. All patients with DM had normal IOP and no neovascular glaucoma (NVG). This may be due to the varying distribution of iris neovascularization. Characteristically, iris neovascularization was usually found around the pupillary margin in patients with DM and it was usually observed in the anterior chamber angle and iris root of patients with the ocular ischemic syndrome. 10 This may be the key reason what we did not find NVG in our patients with PDR.
There is no obvious explanation for the alteration in NVI and why only PDR was associated with NVI. Speculations include that basement membrane thickening, tight junction disruption, and pericyte loss are the determining factors in the leakage of retinal capillaries in mild and moderate nPDR. Vasoconstriction and capillary occlusion worsen the ischemic retina in severenPDR. 11 All these changes in nPDR have released various intravascular contents into the interstitial space, such as proteins, lipids, and inflammatory mediators. However, the concentration of these angiogenic factors is not high enough to cause iris blood vessel changes until the retinal neovascular changes in PDR. Moreover, the gradient-driven diffusion of angiogenic factors from the posterior to the anterior segment of the eye has been observed in ischemic retinal disease. VEGF diffuses following its concentration gradient from the vitreous to the anterior chamber, and it is finally cleared through the trabecular meshwork. 12 In nPDR, the VEGF diffusing into the anterior chamber is sparse and clears rapidly. This gradient and rapid clearance may decrease the potential risk of anterior segment neovascularization.
Conclusion
Due to the association between DI and DR, we can speculate that the characteristic findings of IFA can assist in estimating the fundus severity of patients with PDR; however, these findings can not assess the fundus of patients with nPDR and normal patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Yifeng Ke was supported by grants from the Natural Science Foundation of Tianjin (Grant number: 16JCQNJC12700) and the National Natural Science Foundation of China (Grant number: 81500745). Longli Zhang was supported by Tianjin Clinical Key Discipline Project (Grant number: TJLCZDXKM009).