
Abstract
Ischaemic optic neuropathy (ION) is a major cause of blindness. The clinical approach and management is a matter of debate for the treating neurologist and the ophthalmologist. Of the two broad varieties namely the posterior (PION) and anterior ischaemic optic neuropathy (AION), the arteritic variety of the AION (AAION) is usually due to giant cell arteritis. Giant cell arteritis may only present with visual loss in up to 25% of cases. AAION is a neuro-ophthalmic emergency. Early recognition and differentiation from AAION is imperative in order to prevent further devastating visual loss. A literature search was conducted on pubmed using key words as AAION, arteritic anterior ischaemic optic neuropathy, giant cell arteritis (GCA) and articles from the year 2000 till date were included. In any case very few reviews are available on AAION. The literature search on pubmed provided holistic overview about this clinical significant entity and the same is compiled in this review. Moreover the histopathologic features of a temporal artery biopsy have been described with its microscopic images. In any case reviews are mostly available on the Non arteritic variety of AION. This review recapitulates the diagnostic and management protocol of a patient presenting with AAION.
Keywords
Introduction
Anterior ischaemic optic neuropathy (AION) is one of the important causes of a permanent visual morbidity in the elderly. Though arteritic AION (AAION) is less commonly observed than the non arteritic subtype, it is among the few ocular emergencies that prompts an early establishment of diagnosis to initiate treatment in order to prevent blindness. 1 Arteritic Anterior Ischaemic Optic Neuropathy (AAION) results from infarction of the optic disc, most commonly from short posterior ciliary artery involvement by giant cell arteritis (GCA) leading to its thrombosis and occlusion.1,2 It can rarely occur due to other forms of vasculitis as well, for example, polyarteritis nodosa, systemic lupus erythematosus and herpes zoster.1,2 The aim of this review was to recapitulate the diagnostic modalities currently available as well as those underway for the disease.
Literature search and review
An online review of the PubMed, Google Scholar and MEDLINE was performed, searching for the key words: arteritic anterior ischaemic neuropathy, diagnosis, giant cell arteritis, imaging, optical coherence tomography in the main text. Some literature was obtained from the reference lists of identified publications. The articles published since the year 2000 to date were included for the review of existing literature.
Epidemiology
It occurs predominantly in elderly patients over age 50 years.1,2 It is more commonly unilateral and rarely bilateral.1,2 Although simultaneous bilateral AAION has been reported, more often than not it was due to sequential involvement with one disc showing older changes than the other on fundoscopy.1,3,4 Giant cell arteritis (GCA) is considered the most common cause of AAION and remains the most common systemic vasculitis that is seen in patients aged over 50 years. Giant cell arteritis is more common in women and Caucasians; the prevalence of AAION also reflects the same.1,2,5 The prevalence of GCA is seen to be lower in Asian and Arab (2.3%) than Caucasian populations (10%) indicating prevalence is based on race as well.1,2 The aetiology of GCA is more strongly associated with the genetic background than environmental influences as observed in the United States. 6 GCA is also found in patients of myelodysplastic syndromes. 7
Symptoms
Patients classically present with acute onset profound visual loss (~50% in biopsy positive GCA). 1 It is usually preceded by amaurosis fugax in almost 44% patients.1,2,8 Less commonly reported symptoms include ocular pain (8%), diplopia (6%) and visual hallucinations (<1%).1,9–11 Individuals suffering from GCA may present with additional clinical features in the form of headache (usually a new onset in 67% of the patients and mostly localised to temples in 60%–90% of the patients), weight loss, scalp tenderness, jaw claudication (50%), neck pain, myalgia and malaise.1,2,5,12–15
In contrast, the occurrence of headache, jaw claudication and anterior ischaemic optic neuropathy were notably lesser in patients with GCA in myelodysplastic syndromes (14.3%, 0% and 0% respectively). 7
Forty to sixty percent of patients of GCA are associated with polymyalgia rheumatica (PMR) and they present with proximal myalgia and stiffness of neck. 13
The diagnostic criteria for GCA are based primarily on systemic clinical features and blood investigations. The clinical criteria included in calculating the score for diagnosing GCA in a patient include age at onset if that is more than or equal to 50 years (Score-1), a new type of headache (Score-2), temporal artery abnormality such as tenderness to palpation or decreased pulsation (Score-3), Erythrocyte sedimentation rate of more than or equal to 50 mm in first hour (Score-4) or an abnormal artery biopsy showing vasculitis with mononuclear cell or granulomatous inflammation, usually with giant cell infiltrates (Score-5) (Table 1). 16 However, failure to fulfil these criteria does not preclude a diagnosis of GCA. 16 It has been found that around 21% patients of AAION present with no systemic symptoms, known as ‘occult GCA’.1,2
Revised ACR criteria (rACR) for diagnosis of GCA. a

In the presence of 3 or more points out of a total of 11 with at least 1 point belonging to domain I along-with all entry criteria. If these criteria are met, the diagnosis of Giant cell arteritis can be established.
Exclusion criteria: Ear Nose Throat and eye inflammation, involvement of the renal, cutaneous and peripheral nervous system, infiltration of the lung, lymphadenopathies, stiffness in the neck and digital gangrene or ulceration.
No other possible aetiology is able to explain any one of the above enlisted criteria.
Enlarged and/or pulseless temporal artery: 1.p./tender temporal artery: 1.p.
The parameter must be ignored in the presence of Polymyalgia Rheumatica.
Vascular and/or perivascular fibrinoid necrosis along-with infiltration of the leucocytes: 1.p./and granuloma: 1.p.
Clinical signs –
Visual acuity loss is devastating, being <20/200 in more than 50% of cases. 1 There is a presence of a relative afferent pupillary defect (RAPD) in unilateral cases with an otherwise normal anterior segment. 1 Signs of anterior segment ischaemia with ocular hypotony may be seen along-with marked exudation in anterior segment and this may be confused with clinical presentation of anterior uveitis. 1 In GCA, Visual field (VF) defects may reveal involvement of the central and peripheral fields, but the fellow eye, subjectively asymptomatic, may show altitudinal defect on automatic perimetry that is performed for VF charting. Broadly, visual fields, if feasible, reveal altitudinal defects in AAION. 17
Fundus examination of affected eye typically reveals ‘chalky white’ swollen disc (Figure 1(a)) with cotton wool spots, choroidal infarcts, central retinal artery occlusion(14% patients) and cilioretinal artery occlusion (~22% patients). 1 CRAO in the setting of GCA is found to coexist with occlusion of the posterior ciliary artery (PCA), which is often detected only on fluorescein angiography. 1 Cilioretinal artery occlusion is to be expected since it stems directly or indirectly from PCA for which GCA has a predilection. 1 However, it is often misdiagnosed as ‘branch retinal artery occlusion’, a mistake that may cost the patient their eyesight. Occasionally, there may be hyperaemic swelling too which may mimic non-arteritic AION (NA-AION). 18 When disc oedema resolves, most discs show pallor with significant cupping similar to a glaucomatous optic nerve head (Figure 1(e)) while the fellow eye shows physiological cupping.1,19 These enlisted changes in the eyes are usually not seen in eyes that experience an episode of NA-AION in which the disc has a diffuse/segmental pallor with no/small cup-to-disc ratio.1,19,20 Danesh-Meyer et al. in using confocal laser ophthalmoscopy to compare optic disc morphologies further found that while the cup area and cup/disc ratio were comparable in AAION and open angle glaucoma, glaucomatous discs exhibited significant deepening of the cup in contrast to AAION eyes. 20
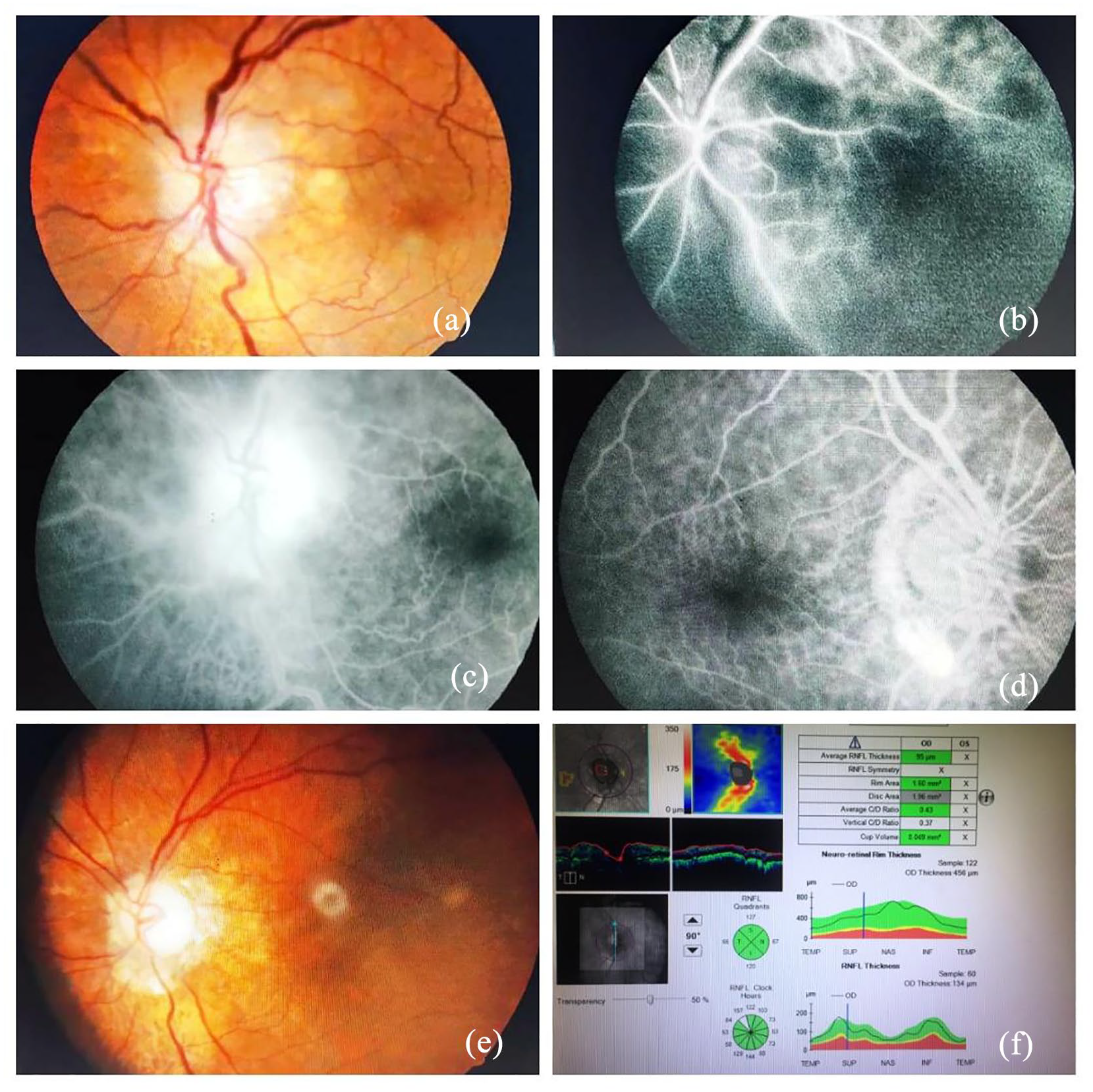
Sequential fundus, fluorescein angiography (FFA) and optical coherence tomography (OCT) images: (a) at presentation, fundus showed pale optic disc oedema with dilated venules, (b) early phase of the FFA showing delayed arteriovenous transit with choroidal infarcts and impaired posterior ciliary circulation, (c) late phase of the angiogram showing persistent laminar flow in the veins and leakage at the optic disc, (d) normal contralateral eye in a patient with AAION on FFA, (e) optic atrophy seen in terminal stage of the disease and (f) optical coherence tomography of the contralateral unaffected eye.
Physical exam may reveal ptosis, nodularity and tenderness of temporal arteries and purpuric lesions on the scalp.1,2 Established cardiovascular risk factors have an association with the onset of PMR and GCA. Raised diastolic blood pressure of over 90 mmHg is seen to increase the risk of onset of PMR, and smoking increases the risk of onset of GCA and peripheral arterial disease. 21 Smoking does not increase the risk of cardiovascular disease in individuals who are diagnosed with GCA.22,23 Pujades-Rodriguez et al. analysed 12 cardiovascular disease (CVD) presentations in 1164 patients with GCA and 9776 patients with PMR. 24 There was no association observed in the 12 presentations of vascular disease in patients suffering from PMR or GCA. Li et al. analysed the data procured by Pujades-Rodriguez et al. and demonstrated an increased risk for vascular disease and further found an increased incidence of CVD events prior to the onset of GCA.24, 25 Patients with PMR or GCA were more likely to have been prescribed an antihypertensive and antiplatelet medication in both the evaluations by the Li et al. 25
Diagnosis
Presentation with acute visual loss in old age patient makes it imperative to differentiate between NAION and AAION (Table 2). This differentiation is important to prevent prolonged periods of unnecessary corticosteroid therapy in patients where the same is not indicated. However, neuro cognitive comorbidities in geriatric population can make it difficult to diagnose promptly, possibly due to vague history or uncooperative patients
Clinical differentiation of NAION from AAION.

Laboratory investigations
Patients with AAION demonstrate raised levels of erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). However, there are many reports where ESR has also been found to be normal or indeed even low in cases of biopsy confirmed active GCA.1,2,5 Evaluation of CRP levels is considered to be more sensitive than estimating ESR in diagnosing GCA.1,2,26,27 Moreover, a combination of ESR and CRP is a highly specific (97%) marker for detection of GCA.1,26 Other less sensitive markers for diagnosing GCA include thrombocytosis, normocytic anaemia and leucocytosis but have a sensitivity below 60%.27,28 Inanc et al. in their recent study suggested neutrophil lymphocyte ratio (NLR) as a reliable index to differentiate between NAAION and AAION. 29 Neutrophil lymphocyte ratio was found to be significantly higher in AAION patients in their study. However, this novel biomarker needs further investigation before being adapted in mainstream clinical practice, because of the relatively small sample size in their study.
Fundus fluorescein angiography and optical coherence tomography (OCT)
Fundus fluorescein angiography (FFA) demonstrates occlusion of posterior ciliary artery. The occlusion is clearly demonstrated by FFA if this investigation is performed soon after onset of visual loss (Figure 1(b)–(d)). 1 However, in later stages the findings are not apparent since there is establishment of collateral circulation. 2 Peripapillary choroid delay, leakage from the disc (focal or generalised) and/or disc filling defects are the three different patterns seen on FFA, of which the delay in peripapillary choroidal filling is more typical in AAION (Figure 1(b) and (c)), but it has also been described in NA-AION. 30 But, FFA being an invasive dye based procedure may result in a few side effects like nausea, vomiting and allergy. It is imperative to screen the other eye of the patient on FFA and OCT (Figure 1(d) and (f)).
With the advent of newer non-invasive OCT angiography (OCT-A), it is possible to recognise micro-vascular perfusion defects in ischaemic optic neuropathies. In a study directly comparing the findings of OCT-A with FFA-ICG in acute ischaemic neuropathies, OCT-A was found to be able to visualise the boundary and the extensions of the optic nerve head non-perfusion areas. These findings were perfectly comparable with FA. 31 In cases where no clear perfusion defects were visible on FA, OCT A was still able to demonstrate a peripapillary capillary network reduction in NAAION while the AAION case showed peripapillary choroidal defect. 31 However due to the small sample size, one cannot presume the sensitivity and specificity of these signs. OCT angiography in AAION has also demonstrated worse vessel density and vessel tortuosity values than NA-AION. 32 Rougier et al. highlighted the importance of segmentation of retinal nerve fibre layer (RNFL) in allowing better imaging of the peripapillary choroidal capillary network, proposing that it reduces the optic disc oedema related artefacts. 33
Temporal artery biopsy
Although, most ophthalmologists do not wait for a histopathological confirmation of GCA to start treatment, temporal artery biopsy (TAB) is the gold standard for diagnosis of GCA (Figures 2(a) and (b) and 3(a) and (b)).1,2,5 Microscopic examination of the sections from temporal artery show inflammatory infiltrate in the tunica adventitia and tunica media layers of the arterial wall (Figure 3(a) and (b)) with fragmentation of the internal elastic lamina with or without the presence of giant cells.5,8 The sensitivity of TAB ranges from around 70% to over 90%. Thus, a negative biopsy does not exclude the diagnosis of GCA. 5 Skip lesions are cited as the reason for false negative results of a TAB.1,5 Complications of the TAB procedure are rare (~0.5%), however incidences of injury to the facial nerve, drooping of the eyebrow, skin necrosis, infection and stroke are known. 5 In addition, some patients may refuse to undergo this invasive procedure.
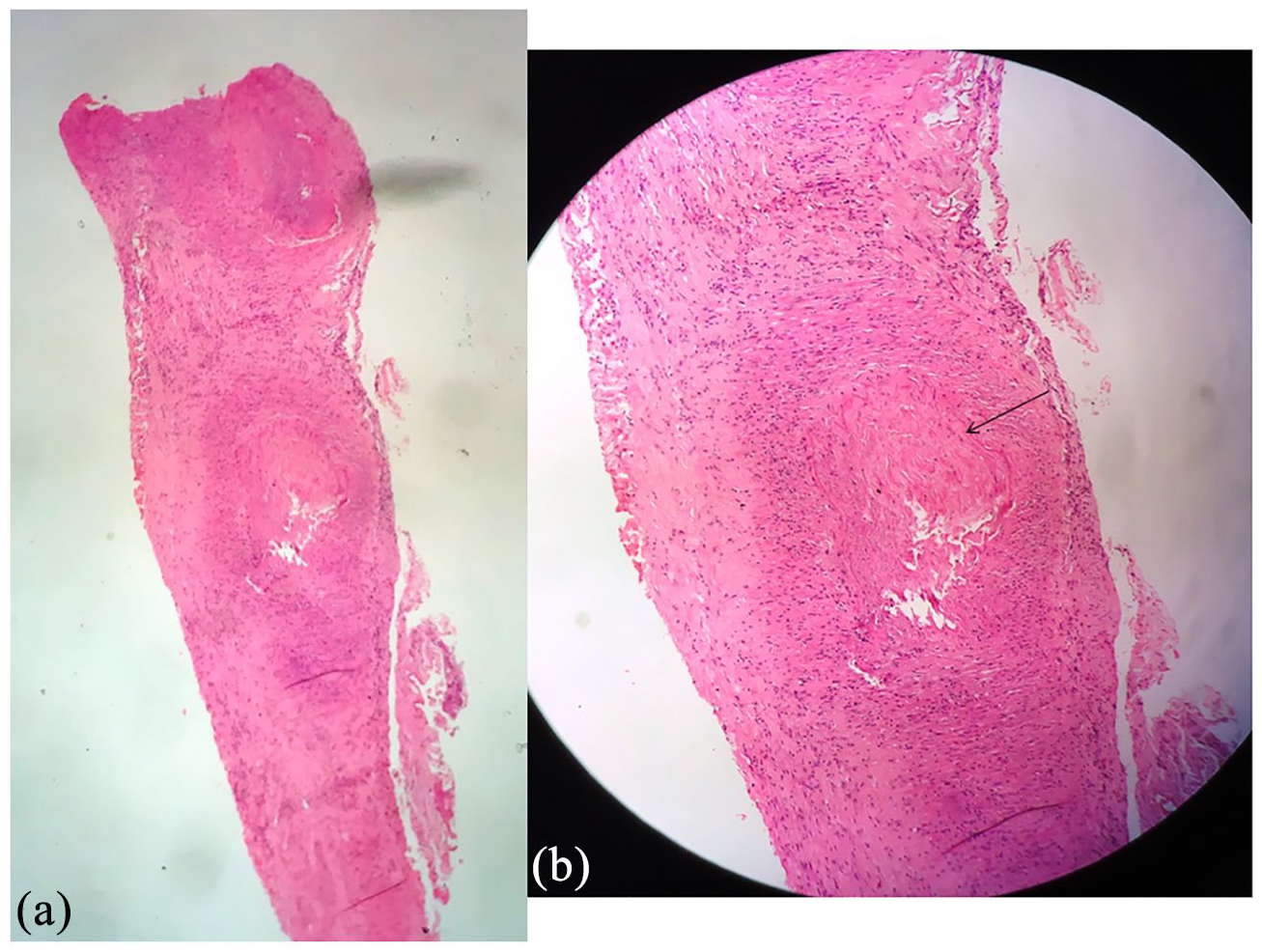
Temporal artery biopsy (TAB): (a) haematoxylin and eosin stained sections of the TAB as observed under a scanner view in the microscope and (b) thrombus in the lumen of temporal artery as seen under magnification of 10× (H & E, 10×; b).
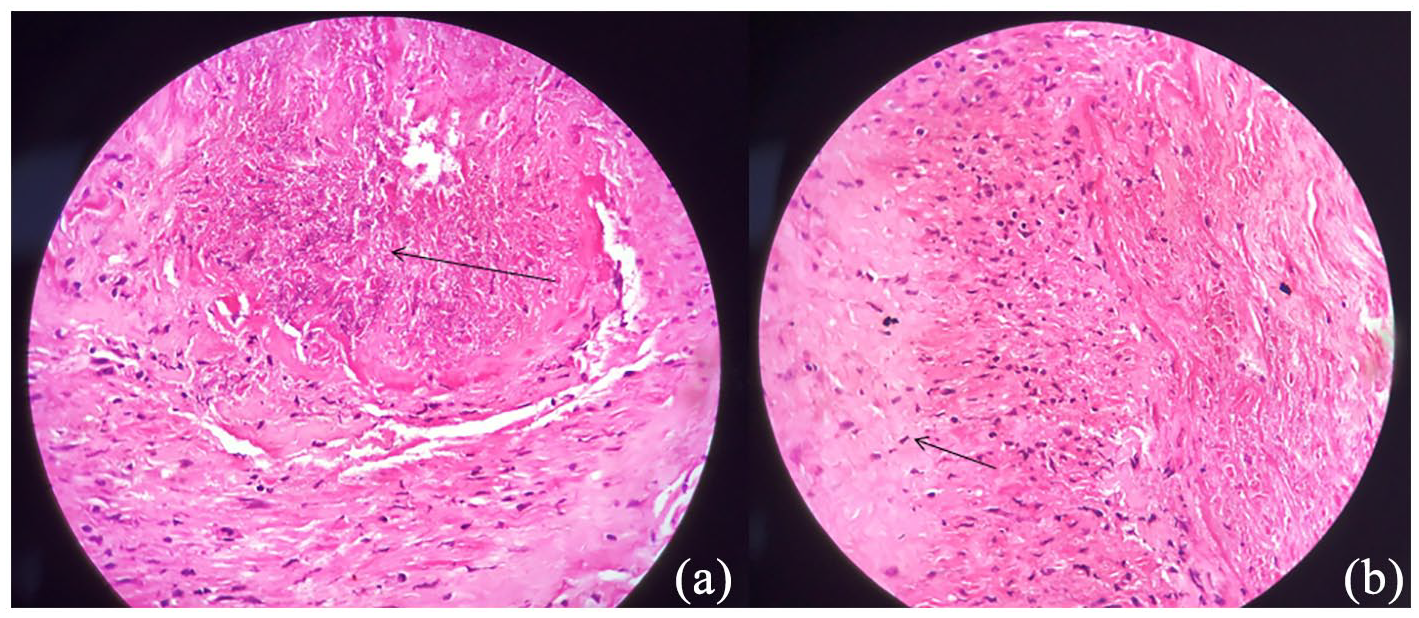
Magnified view of the temporal artery biopsy: Necrotic material seen in the lumen of the temporal artery along-with blood clot and inflammatory cell infiltrate (Black arrow, 40×, H and E; a). There is reduplication of the internal elastic lamina of tunica intima, the innermost layer of the temporal artery (a). Spindle shaped smooth muscle cells of the tunica media layer, as seen (Black arrow; b).
Radiological investigations
Performing colour Doppler and duplex ultrasonography of temporal arteries in one sitting in patients with GCA is gaining popularity. A reduction in blood flow with the stenosis of the artery is observed. A circumferential thickening of the arterial wall around the lumen of the artery appears as a dark hypoechoic area giving a typical appearance of a ‘halo sign’ which has specificity of 89%–91% and a sensitivity of 69%–75% in experienced hands. 5 This finding disappears after 2–3 weeks of initiation of therapy. 5 However, the operator dependency of ultrasonography proved to be a major limitation by affecting reproducibility of the sign. Aschwanden et al. in a bid to find a simpler and relatively operator independent ultrasound marker for temporal arteritis put forward the ‘compression sign’. 34 If on compression sonography, the wall of temporal artery remains visible in contrast to surrounding structures, the sign is considered ‘positive’ for arteritis. In their study, they found this novel sign to be equally sensitive and specific to halo sign in identifying temporal arteritis as well as having ‘excellent interobserver agreement’.34,35 High-resolution vessel wall magnetic resonance imaging (HR-VW MRI) is emerging as a highly accurate modality for distinguishing AAION from NAAION. A prospective study of 27 patients with AION showed inflammatory changes in wall of ophthalmic artery were seen in all cases of AAION and none of the cases of NAAION, putting the sensitivity and specificity of the HR-VW MRI at 100%. 36 Involvement of the posterior ciliary artery in patients with AAION has been detected using a three-dimensional high-resolution T1-weighted black-blood MRI (T1-BB-MRI). It was shown to have specificity of 92.3% and sensitivity of 92.9% for detection of patients with AAION. 37 It was also able to detect posterior ciliary involvement in GCA patients with unremarkable fundoscopy thus helping in detection of ‘at risk’ eyes and possibly, prevention of visual loss in these eyes. 37 However, MRIs are expensive investigations and may not be available easily, especially in the setting of developing country such as India.
GCA may also demonstrate optic nerve sheath enhancement that is possibly due to inflammation along with ischaemia of the optic nerve. 38 Differential diagnosis of a patient presenting with acute onset visual loss, optic disc oedema and such an MRI usually includes optic neuritis and optic perineuritis. Very few cases of OPN have been reported in GCA, with most being bilateral.39,40 The aetiology of OPN is usually idiopathic though infection or inflammatory disorders such as vasculitis may also present with OPN.39–42 OPN due to GCA may be difficult to recognise, especially since the corticosteroid treatment initiated early in the disease process masks typical features of GCA. 39 Steroid administration demonstrates a visible visual recovery in cases of OPN but the cases of GCA with enhancement of the optic nerve sheath have a poor response to steroid therapy.41,42
Treatment
While administering treatment to patients with AAION the main aim is to ensure preservation of vision in the fellow eye. 2 If left untreated, 54%–95% of patients progress to complete blindness in affected eye. 43 The rate of vision loss can be reduced to 13% with glucocorticoid treatment. 36 Moreover, 50% of patients with unilateral AAION may lose sight in the unaffected eye within days if no treatment is administered. 43 Thus, treatment should be promptly instituted upon suspected diagnosis.
High dose systemic corticosteroids are the mainstay of treatment.1,2 A high dose of intravenous (IV) methylprednisolone (1 g/kg/day) is administered initially for 3 days followed by oral prednisolone in a dose of 1 mg/kg/day as a maintenance therapy for at least 4–6 weeks. 2 This regimen is advocated by most neuro ophthalmologists in the setting of acute profound visual loss in GCA patients and/or when there is development of visual field defects or amaurosis fugax in these patients suggesting that vision is at risk. Various studies have been conducted that tested the benefit of IV steroids in GCA patients (Table 3).44–46
Summary of studies conducted testing the benefit of IV steroids in GCA patients.

Tapering of steroids should be guided only by estimation of a reduction in the levels of ESR and CRP and this varies from individual to individual. 2 Since there might be a relapse during tapering period, it needs to be a slow process and typically a steroid course of at least 1–2 years is needed. Tapering can be begun by reducing the dose by 10 mg per month till 20 mg/day is reached, then by 5 mg every month and further as little as 1 mg every month once a dose of 10 mg/day is reached. Alternate day corticosteroid regimens are not recommended, because rebound arteritis has been associated with this regimen. 47 Compared to idiopathic variant, GCA in MDS patients showed more steroid dependence and decreased relapse-free periods. 7
A life-time of steroid therapy is needed in most of the patients to prevent visual loss. 2 Since AAION affects the elderly population who already have multiple co existing co-morbidities, a careful lookout needs to be kept for the various systemic side effects of corticosteroids. Indeed, it is advisable to start calcium supplementation and vitamin D in a dose of 1200 mg per day and 800 IU per day respectively as a prophylactic measure.
Methotrexate (7–15 mg/week) is one of the most widely studied ‘steroid sparing’ agents. A metaanalysis has concluded the benefit of adjunctive methotrexate in preventing relapses and reducing the total dose of steroids by 48 weeks. 48
Case reports of addition of intravenous prostaglandin E1 (PGE1) after initial dose of intravenous steroids have shown that this regimen appears to be effective in early reduction of ESR and CRP levels with no drastic improvement in the visual acuity of patients. However, we note that the dose of intravenous steroid used was less than the norm (owing to co morbid conditions of the patients) which may have affected the results. 49 This premise needs to be explored with larger trials especially since IV PGE1 have been shown to be beneficial in patients of peripheral vascular diseases. 50
Recently, Tocilizumab (Anti IL-6 receptor monoclonal antibody) received FDA approval for treatment of GCA in 2017 and was also shown to be effective against corticosteroid resistant AAION. 51 Calderón-Goercke et al. found it to be excellent steroid sparing option with their real world data showing rapid decrease in CRP and ESR levels as well as persistent disease remission in 69.2% patients. 52 Serious infections emerged to be the most significant side effect, found in 11.9% of patients. 52 Most recently Unizony et al. in their retrospective analysis, concluded that there was a decreased incidence of fresh GCA-associated visual symptoms when patients were given tocilizumab and no new cases of AAION or permanent blindness were reported. 53 Whereas tocilizumab have actually been demonstrated to be effective in idiopathic GCA, biological-targeted therapies seem to be less effective in MDS/MPN associated diseases with increased risks of cytopenias, in particular neutropenia. 7
No strong scientific evidence exists that supports the usefulness of other cytotoxic agents/immunomodulatory therapy such as cyclosporine, hydroxychloroquine, azathioprine, etc. in treatment of GCA over steroids. Figure 4 shows the stepwise management approach in a patient presenting with clinical features suggestive of AAION.
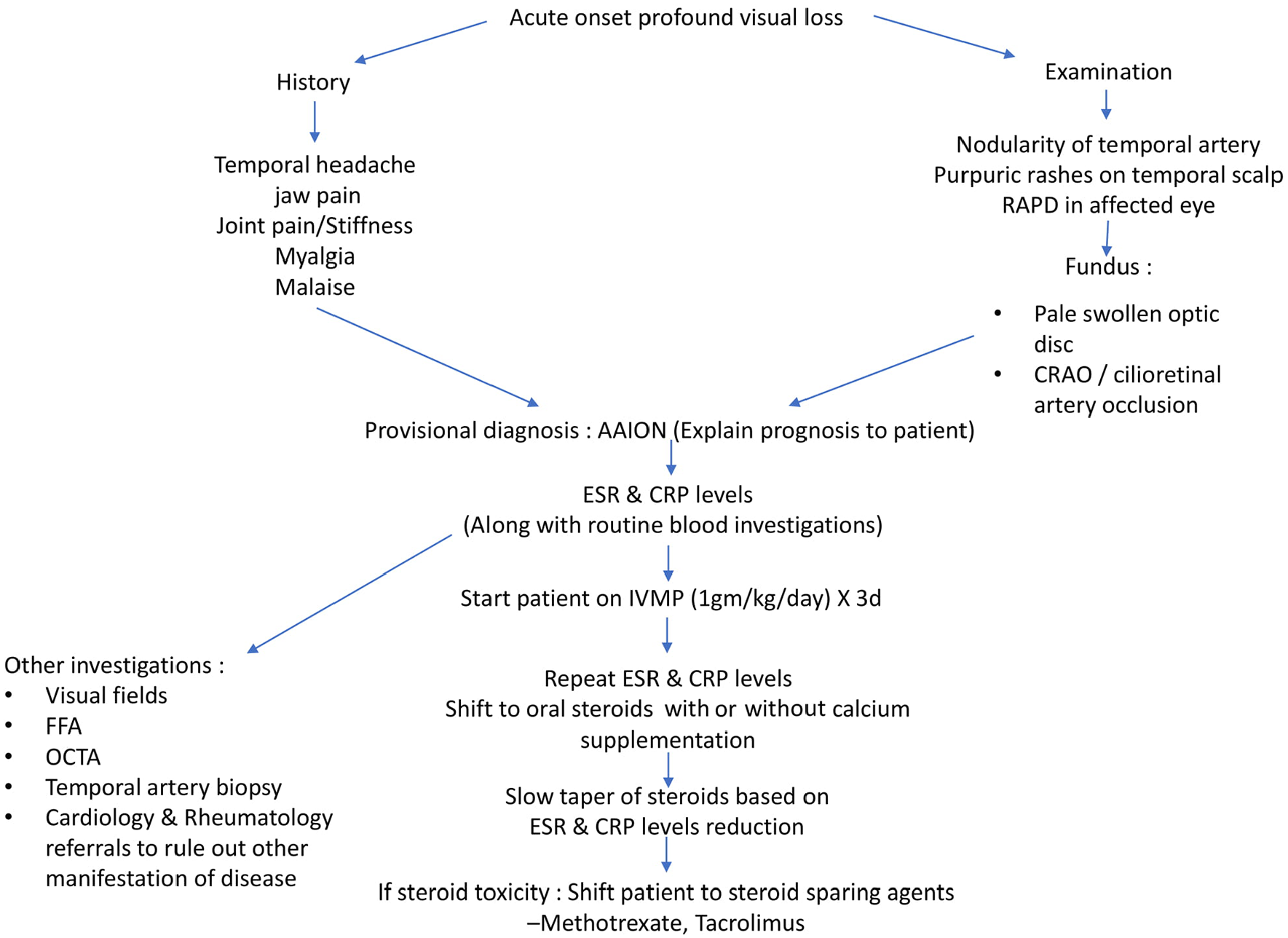
Flow chart depicting management approach to a patient presenting with AAION.
Prevention
There are no randomised controlled trials that have evaluated the use of aspirin as an adjuvant treatment in GCA. 54
Two retrospective studies have demonstrated protective effects of low-dose aspirin in averting ischaemic intracranial episodes in patients with GCA.55,56 But other studies have not corroborated these results which makes the use of aspirin in GCA controversial.57,58
Conclusion
The almost fulminant nature of visual loss in setting of AAION makes it an ocular emergency. Establishment of a definitive diagnosis is important. Not all cases present with textbook features and in clinical practice differentiation between NAAION and AAION is often difficult. Being a disease of elderly population who are often fraught with multiple comorbidities, giving steroids indiscriminately can lead to increased morbidity. In addition, the recent trend in diagnostic workup of AAION seems to be shifting towards finding non-invasive markers of the disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
There are no ethical issues related to this case report.
Informed consent
Informed consent was taken from the patient for inclusion of clinical photgraphs in the case report.