
Abstract
Purpose:
Retinopathy of prematurity (ROP) is the leading cause of childhood blindness. The aim of our study is to validate the new screening criteria elaborated by the Postnatal Growth and Retinopathy of Prematurity (G-ROP) study group in a monocentric cohort of Italian preterm infants.
Methods:
We retrospectively applied the G-ROP screening criteria to a cohort of preterm infants born between May 2015 and July 2020 with known birth weight, gestational age, serial weight measurement, and known ROP outcome. Primary outcomes were sensitivity and specificity of ROP detection, especially of treatment requiring ROP. Secondary outcomes were reduction of ophthalmologic examinations and of infants requiring screening.
Results:
We retrospectively evaluated 595 children and 475 were included in our study. Of them, 119 developed any type ROP, 39 developed type 1 ROP, and 28 underwent treatment. G-ROP criteria predicted 39 of 39 cases of type 1 ROP (100% sensitivity and specificity). Sensitivity and specificity for detection of treated ROP were 100%. Considering any type ROP detection, sensitivity was 87.4% and specificity was 100%. Our analysis showed that screening could be avoided in 50% of patients, resulting in a 29% reduction of the number of examinations.
Conclusions:
Our study validates the new G-ROP screening protocol in a monocentric cohort of premature infants. We demonstrate that all Type 1 ROP and requiring treatment ROP could be found even with a reduction of eye examinations.
Introduction
Retinopathy of prematurity (ROP) is a disease that afflicts low birth weight preterm newborns and is a major cause of childhood blindness. ROP is caused by a disorder of the retinal blood vessels development that usually proceeds from the optic nerve head to the periphery during gestation. In preterm newborns the lower is the gestational age, the greater is the risk of incomplete development of retinal vascularization. 1
ROP screening in Italian clinical practice follow the AAP (American academy of pediatrics) indications, 1 including all preterm newborns with a gestational age (GA) less than 30 weeks and/or a birthweight (BW) <1501 g, as well as infants with GA more than 30 weeks and/or a birthweight between 1500 and 2000 g with a complicated clinical course and a ventilatory support necessity. 2
The specificity of those criteria is low for type 1 ROP, with only half of examined newborn develop any ROP and approximately 7% receive treatment. 3
In 2018, new screening criteria for ROP were elaborated by the Postnatal Growth and Retinopathy of Prematurity (G-ROP) study group, 4 and validated in a North American cohort of preterm newborns. 3 The new prediction model achieved more than 30% reduction in ophthalmologic examination for ROP, with a sensitivity of 100% for Type-1 ROP and 98.6% for Type-2 ROP, 3 and a great reduction of cost. 5
In literature there are other three validation studies,6 –8 which confirm the efficacy and safety of the G-ROP screening criteria. However, to extend its use worldwide, more validation studies on different cohort are needed. This study aims to compare all parameters including sensitivity and specificity between current ROP screening criteria,1,2 and new G-ROP screening model, 3 in a preterm newborns population as well as the ability to identify infants needing treatment.
Methods
We conducted a retrospective study on a preterm newborns’ cohort from a single Neonatal Intensive Unit in Italy, from May 2015 to July 2020. The study complies with the principles of the Declaration of Helsinki (1964). Inclusion criteria were GA <34 weeks with a BW <2500 g, but also newborns considered to be at high risk of developing ROP by a neonatologist (e.g. infants with risk factors like sepsis, necrotizing enterocolitis, blood transfusions or ventilatory support necessity).9,10
Exclusion criteria were newborns with unknown ROP outcome, deceased newborns, patients transferred from another center after the start of the follow-up and infants without daily sequential weight determination. All newborns in the study were examined by an ophthalmologist with binocular indirect ophthalmoscope after 28 days from birth or between 29 and 31 weeks of GA. Eye exams were performed as indicated by AAP until discharge. 1 ROP diagnosis and treatment indications were deduced from the International Classification of ROP Revisited, 11 and the Early Treatment for ROP Study. 12
We searched demographic and ophthalmologic data from medical records: for each patient we collected birth and discharge date, length of stay, sex, BW, GA, all available weight measurements, every information about presence of hydrocephalus, number and dates of eye examinations, ROP zone, stage, development and any treatments performed. Afterwards, we examined the data obtained considering the new criteria suggested by the G-ROP study: GA <28 weeks, BW <1051 g, weight gain <120 g between age 10 and 19 days, weight gain <180 g between age 20 and 29 days, weight gain <170 g between age 30 and 39 days and hydrocephalus. 3
We applied G-ROP model criteria to patients who already undergone eye screening during the previous hospitalization following the guidelines in use. Infants who met at least one of the six criteria were considered as undergone ophthalmological examination. Those who did not meet even one were considered as ineligible for screening and therefore as not evaluated.
The final number of visits considered the number of examinations conducted in patients who would screen plus the amount of the examination following the growth slowdown finding. Primary outcomes were sensitivity and specificity measures of the model for detecting type 1 ROP, any stage ROP and treated ROP among our cohort. Secondary outcome was the reduction in number of examination and infants requiring ophthalmologic exam. Descriptive statistics were generated for the whole cohort and data were expressed as mean and standard deviation (SD) for continuous variables. Moreover, median value and range were calculated and reported, as were absolute or relative frequencies for categorical variables. Sensitivity and specificity with 95% confidence intervals (CI) were calculated. Statistical analysis was performed using SPSS for Windows (SPSS Inc., Chicago, IL, USA).
Results
Of 595 infants which met the inclusion criteria, 475 were eligible in this study. We excluded from the study patients transferred from another center after the start of the follow-up (n = 2), patients without eye evaluation before transfer to another center (n = 18) or before discharge (n = 62), infant without weight records (n = 13), infant with other eye disease (n = 1), and death (n = 24) (Figure 1).
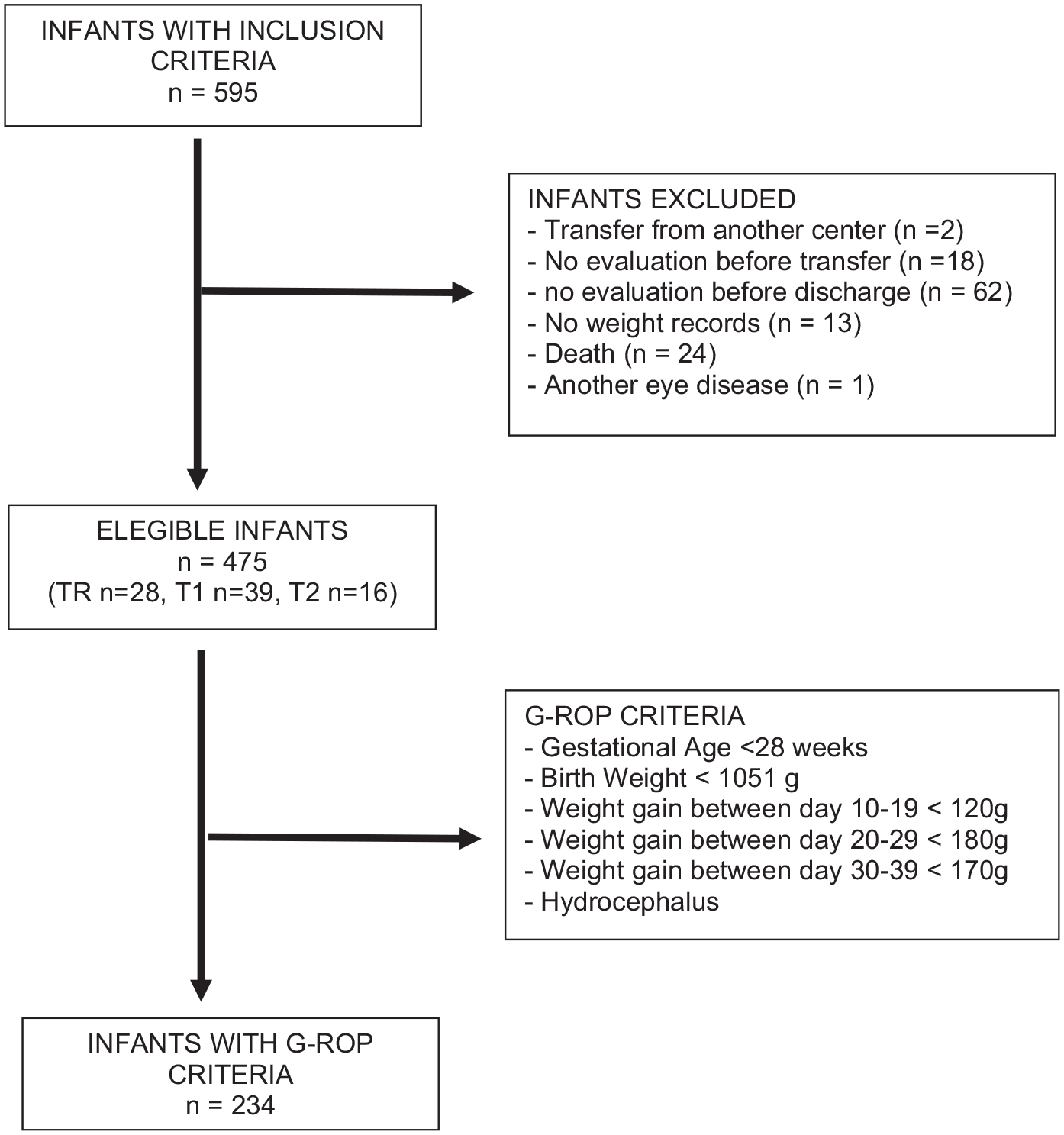
Flow-Chart. The chart shows the process of inclusion and the exclusion criteria of the patients in the study.
The median GA was 30.4 ranged (22.1 weeks to 33.8 weeks) with median BW was 1300 g (range 410–2840 g). The number of total females was 236 (49.7%). Of the 475 newborns, 119 (25.1%) developed any type ROP, of whom 39 (32.8%) developed type 1 ROP, 16 (13.4%) developed type 2 ROP and 64 (53.8%) either not Type 1 or Type 2 ROP. The treated newborns were 28 (23.5%): of them 26 had type 1 ROP, 2 had Type 2 ROP.
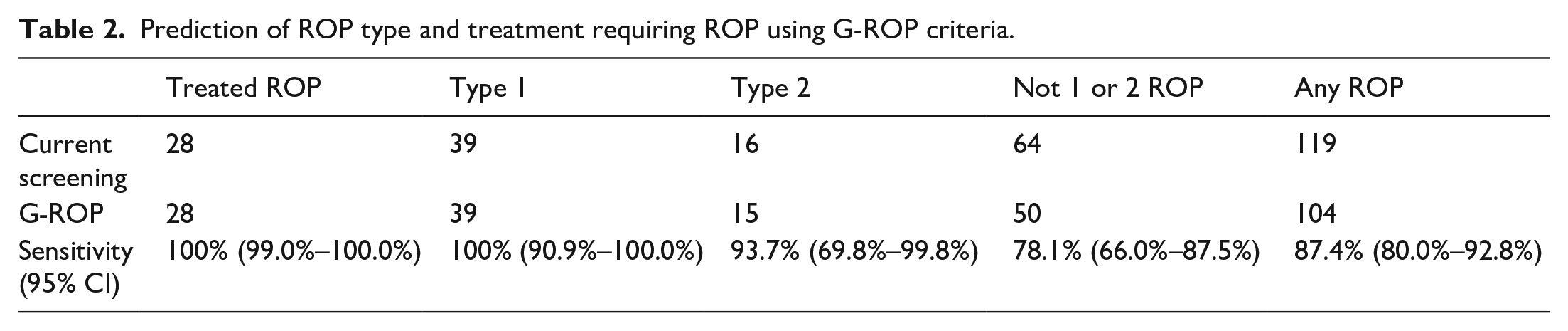
Applying G-ROP screening model, we predicted all the 28 infants who underwent ROP treatment (Sensitivity 100%; 95% CI 88%–100%; and Specificity 100%; 95% CI 99%–100%). The Infants who would be undergoing treatment using G-ROP criteria at birth, would be 26 and the other two infants would be found out with WG criteria. The G-ROP screening model predicted 104 newborns of the 119 who developed any Type of ROP (Sensitivity 87.4%; 95% CI 80.0%–92.8%. Specificity 100%; 95% CI 98.9%–100%) (Table 1).
Comparison between current ROP screening criteria and G-ROP screening criteria.

Applying G-ROP screening model we found 39 newborns with type 1 ROP, 15 newborns with type 2 ROP and 50 newborns with either not Type 1 and 2 ROP (see Table 2 for comparison). In G-ROP screening model, 15 newborns who had developed ROP (1 type 2 ROP and 14 not 1 or type 2 ROP) would remain unscreened but these did not need to be treated. Among preterm infants included in the study, 24 (5%) developed hydrocephalus following intraventricular hemorrhage: 11 would have been selected for altered parameters at birth (BW or GA), 3 would be included in the screening program due to a slowdown in weight gain while in 10 patients the only altered parameter was hydrocephalus. Among the 24 patients suffering from hydrocephalus, 8 developed ROP (4 infants Type 1 ROP, 2 infants type 2 ROP and 2 not Type 1 or 2 ROP). Two of them underwent treatment. All the treated infants had an altered parameter in addition to hydrocephalus. At last, of the 475 infants from our cohort, G-ROP model excluded from eye screening 241 infants (50.7%), with a reduction of examination of 772 (29.2%).
Prediction of ROP type and treatment requiring ROP using G-ROP criteria.
Discussion
Our study validated G-ROP criteria for ROP screening in an Italian monocentric cohort of preterm infants. G-ROP is a prediction model based on BW and GA, the two most significant risk factor for ROP development,9,10,13 plus low weight gain as a surrogate of IGF-1 levels and hydrocephalus as source of non-physiologic weight gain. 3 The G-ROP protocol is the latest of several screening methods proposed during the last 20 years,13 –16 based on gestational age, birth weight, and weight gain. Compared to the other methods, G-ROP screening protocol could either be simpler to use and avoid errors because it does not involve algorithm or equation. The primary aim of our study was to find a strong and effective screening model for ROP detection the lower subjective as possible. The secondary aim was to reduce the great number of eye examination and associated ophthalmologist effort. After we applied G-ROP criteria in our cohort, we detected 104 of 119 infants who developed any Type of ROP, reaching a sensitivity of 87%. Nevertheless, we detected all the 39 infants who developed Type 1 ROP as well as all the 28 newborns who underwent treatment for ROP. We showed that despite a reduction in ROP detection sensitivity, with 15 of 119 ROP misses (13%), no infants who requiring treatment would be miss, reaching a 100% sensitivity and specificity for treatment requiring ROP and for Type 1 ROP. We also registered a reduction in number of eye examination (772 examination, 29.1%) and in infants who required ophthalmologic follow up (241 patients, 50.7%).
This model showed very high sensitivity value, even if applied to a cohort of patients with different characteristics from the ones observed in North America or Japan. This data confirms the utility of G-ROP screening protocol. At time of writing there are only three validation study for G-ROP protocol.6 –8 The data we collected are similar to those showed by Shiraki et al., 6 in a retrospective analysis of a Japanese preterm cohort. As illustrated by Shiraki, retrospective collection of data is not a limitation: in neonatal intensive care unit, accurate record of daily weights is a common practice, as the close ultrasound brain monitoring, and data we have collected are therefore reliable and complete. Compared to their results, we found a much higher proportion of reduction of patients examined (50.7% vs 24.5%) and in eye examination (29.1% vs 12.9%). Therefore, G-ROP criteria would lead to a significant drop of efforts and costs in our group, as described by Wadley et al., 8 and according with CO-ROP model, 17 fewer dilated eye examinations could further reduce distress for premature infants.
Differently from the previous Japanese study, we also included the detection of hydrocephalus in our retrospective analysis and we were able to add other 10 infants who otherwise would have been excluded from screening protocol. Fortunately, no one of them developed any ROP and all the newborns with hydrocephalus who underwent treatment had a second altered parameter. Especially considering that the mean BW value in our cohort was higher than the ones proposed by the Japan validation study (986 gr), 7 and G-ROP validation study (1070 gr), 4 the BW and the 3 WG thresholds criteria could have inferior safety margins than in the other studies. Therefore, despite we observed no ROP development in preterm newborns with isolated hydrocephalus, this parameter could be very useful in different settings to find out infants without low BW or GA or poor weight gain who would require eye examination for ROP development risk.
It should be emphasized that through the application of G-ROP criteria, we did not detect some infants who developed ROP: one developed Type 2 ROP and 14 developed not classifiable either Type 1 or 2 ROP. Despite this no one of them required treatment and all of them regressed spontaneously. We want to highlight the case of the missed infant with type 2 ROP, who developed a stage 3, zone 2, nonplus ROP, which spontaneously regressed without treatment. From an analysis of the available data, the patient reported no major risk factors for the development of ROP. 9 He did not develop sepsis or necrotizing enterocolitis and he did not need blood transfusions. He required ventilatory support for 36 hours with synchronized intermittent positive pressure ventilation (SIPPV) and 4 days with CPAP (Continuous Positive Airway Pressure), with oxygen saturations never excessively high. Brain and heart ultrasound examinations were normal. Genetic factors and polymorphisms might also affect risk for retinopathy of prematurity 9 ; therefore, it is possible that the disease development is linked to them. Unfortunately, we do not have genetic analysis available for this patient.
Of the 14 patients with either not Type 1 or 2 ROP misses at screening, 3 newborns developed stage 2 zone 3 ROP, 4 newborns developed stage 2 zone 2 ROP and 7 newborns developed stage 1 zone 2 ROP. Mean spontaneous regression occurred in 34.5 days, with a minimum of 10 days and a maximum of 84 days. Total number of eye evaluation for these patients was 62.
The great accuracy in detection of ROP needing treatment and the reduction of eye examination could justify the exclusion of those newborns, especially because of the spontaneous regression without any medical intervention. Otherwise, the application of the screening model does not avoid the possibility that neonatologist applies a subjective judgment to also include newborns who not strictly comply with the G-ROP criteria, but who show other risk factors for ROP.9,10
There are two major limitations to our study: first, no data about risk factors (surgeries, sepsis) for ROP development were available. As we previously suggested, the importance of these factors is important for the development of retinopathy and therefore it could be the aim of a future prospective study. Second limitation is the impossibility to quantify the resources savings related to the reduction in eye examinations. It could be interesting to elaborate a further analysis about the economic aspect of the introduction of the new screening model.
In conclusion, our study demonstrates that the new G-ROP screening protocol can find the same patients affected by ROP needing eye treatment on a cohort of Italian premature newborns, compared to the criteria currently in use. We also demonstrate that about a third of eye examinations could be avoided, allowing a better allocation of resources and ensuring not only the same results, but also greater care for the patient. This validation study showed that those criteria could be extended in Italy and this is the first step to introduce them in the whole European countries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.