
Abstract
Purpose:
To assess the association between carbohydrates (CH) intake and glaucoma incidence.
Methods:
18,247 volunteer participants (183,067 person-years at risk) with 10-year of median follow-up were included in this prospective dynamic cohort. Baseline total CH intake (g/d) was categorised in quartiles and classified in nine different CH food sources. Self-reported diagnosis of glaucoma was collected at baseline and on biennial follow-up questionnaires. CH intake and glaucoma diagnosis were validated in a subsample of participants. We studied potential confounders and effect modificators, including diabetes. The relationship between CH intake and glaucoma incidence was analysed using multivariable Cox proportional hazards ratio (HR) models to adjust for potential confounding factors.
Results:
During 10 years of median follow-up, a total of 242 new cases of glaucoma were identified. Participants in the highest quartile of baseline CH intake had a significantly higher risk of glaucoma as compared to participants in the lowest quartile [HR 1.50 (95% Confidence interval (CI): 1.01–2.25), p for trend = 0.042]. None of the nine CH food groups was individually related to glaucoma. In stratified analyses, after excluding all cases of diabetes, the HR comparing extreme quartiles of CH intake was 1.77 (95% CI: 1.15–2.74).
Conclusions:
Our results suggest that a higher intake of total carbohydrates is associated with a higher risk of incident glaucoma. The total amount of CH, rather than the specific food sources of CH, seems to play a major role, and this association does not seem to be confounded or modified by diabetic status.
Introduction
Glaucoma is one of the most common eye diseases and the second leading cause of blindness worldwide. 1 In 2010, 60.5 million people were diagnosed with glaucoma, and this optic neuropathy is expected to affect 79.6 millions by 2020, and 111.8 millions by 2040.1,2 The most efficient approach to reduce new cases of glaucoma is to identify and control risk factors associated with this disease. Previous cohort studies have shown a higher risk of glaucoma in persons with advanced age,3,4 African American and Latinos ancestry3,5 or axial myopia.4,6,7 However, the association between modifiable factors, such as dietary factors, 2 and glaucoma incidence or progression deserves further investigations. 8
The “
High carbohydrate intake has been previously associated with diabetes mellitus incidence, and diabetes mellitus has been associated with glaucoma incidence.14,15 The objective of this study was to determine the association between high carbohydrate intake and glaucoma incidence, and to investigate whether carbohydrate (CH) intake could act as a risk factor for glaucoma, independently of diabetic status. As far as we know, there are no previous published studies analysing the relationship between CH intake and risk of glaucoma. In order to assess modifiable glaucoma-related dietary risk factors, we analysed the association between total CH intake and nine different sources of dietary CH and the incidence of glaucoma in the SUN cohort.
Material and methods
Study participants
Twenty thousand two hundred and seventy-nine participants were initially eligible for inclusion [SUN participants who had responded the baseline questionnaire (Q0) before March 2014]. We also used the information collected after 2-year follow-up (Q2), and after every two subsequent years (Q4, Q6, Q8. . .) until the last follow-up questionnaire available at the time of these analyses, (Q16) that collected information after 16 years of follow-up. Data analysis excluded 1850 participants who were lost to follow-up and did not respond to follow-up questionnaires (retention rate 91.1%). Two thousand one hundred and fourteen participants with extremely low or high total energy intake defined according to Willet, 16 and 68 participants with prevalent glaucoma at baseline were also excluded as shown in the flow-chart (Figure 1). Finally, 18,247 participants were available for analysis, 10,965 women and 7282 men with a mean age of 37.8 (SD 12.2).
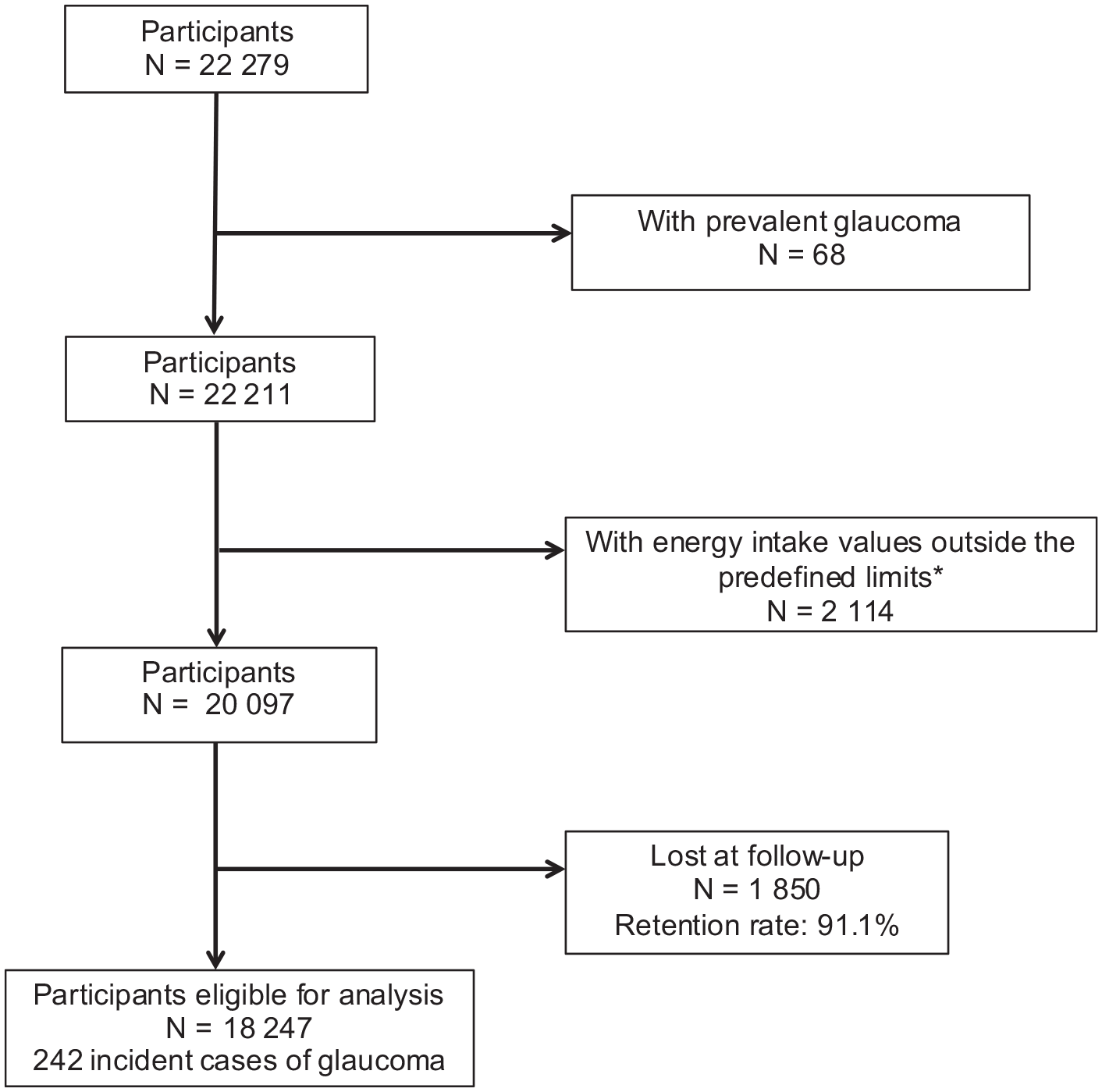
Flow chart of subjects in the Seguimiento Universidad de Navarra (SUN) Project, 10 years of follow-up.
Exposure assessment: Carbohydrate consumption
Dietary exposures at baseline were gathered using a semi-quantitative food frequency questionnaire (FFQ) with 136 items repeatedly validated in Spain.17,18 The FFQ validation study showed a moderately good validity for assessing carbohydrate intake. Total CH intake (g/d) was calculated including CH from all food sources. Additionally, we classified CH sources in nine groups: refined CH, fruits, vegetables, dairy products, sugary drinks, legumes, whole grains, alcoholic beverages and meats and fish (Table 1). The validated FFQ collects the frequencies of food consumption in nine categories (from never or almost never up to more than six times per day). Energy and nutrient intake were calculated from tables according to food composition and performed by trained dieticians.19,20 We also used the residual method proposed by Willett et al., 21 in order to better calculate our main exposure variable (CH intake). The residuals (observed intake minus intake predicted from energy) had a correlation equal to 0 with total energy intake and, thus, they represent the excess or shortfall of CH intake under conditions of equal total energy intake.
Food groups and the foods included in each one.

Outcome assessment: Glaucoma
Glaucoma diagnoses were assessed at baseline and through the SUN follow-up questionnaires repeated every 2 years. Participants responded to the following question: “Have you ever been diagnosed of glaucoma by a health professional?” The question also specified the date of diagnosis. The diagnosis of glaucoma was validated in a subsample of 150 participants. Self-reported information was compared to clinical evaluation, made by an experienced ophthalmologist, blinded to the information referred by participants. Glaucoma was defined, according to the European Glaucoma Society as optic nerve rim damage and retinal nerve fibre loss with related visual field defects. This validation study found an adequate glaucoma diagnosis based on the self-reported diagnosis of glaucoma. The Kappa value was 0.85 (95% coefficient interval [CI], 0.834–0.872). The sensitivity was 0.83 and the specificity 0.99. Prevalent cases of glaucoma at baseline were excluded from the analysis.
Assessment of other variables
The SUN questionnaires also collected information useful for multivariable adjustments, such as: sociodemographic variables (i.e. age, sex, educational level), lifestyle and health-related characteristics, (i.e. smoking, physical activity, adherence to the Mediterranean diet, total energy intake, special diets consumption, caffeine intake, Omega 3/6 ratio), anthropometric measures, (i.e. weight and height) and medical history (prevalent disease as hypertension, cardiovascular disease, cancer, or diabetes and medication use).
Statistical analyses
We conducted a first analysis, investigating differences in the baseline characteristics of the 18,247 participants included for analysis and the 1850 not included in the final sample. Participants were divided into quartiles based on their total energy intake (Kcal/d) and CH intake (g/d). To analyse the contribution of the nine food groups to the total CH intake, we calculated sources of variability (R2) and quantities of CH for each group. We calculated person-years follow-up from the date of completion of the baseline questionnaire to the date of glaucoma, death, or return of the last follow-up questionnaire, whichever occurred first. We estimated hazard ratios (HR) and 95% confidence intervals (CI) of glaucoma, for every of the three upper quartiles of carbohydrates intake versus the lowest quartile, using Cox proportional hazard regression models with age as underlying time variable. We adjusted for multiple potential confounding factors: adherence to the Mediterranean diet (0 to 9 Trichopoulou’s score, 22 anthropometric data (body mass index [BMI]), prevalence of cancer at baseline, cigarettes smoked per year (pack-year) leisure-time physical activity (METS-h/wk), caffeine intake (continuous), alcohol intake (continuous), omega-3/omega-6 ratio, (continuous), prevalence of arterial hypertension at baseline, prevalence of type 2 diabetes at baseline, educational level and year of completion of the baseline questionnaire. We used categories of age (roughly deciles) and year of entering the cohort as stratification variables. P for linear trend was added by assigning to each quartile of CH intake the median of that category (g/d) and treating the variable as continuous.
We additionally used Cox proportional hazard regression models to estimate the risk of glaucoma associated with CH intake from each source (food groups). We also used the residual method and defined the first quartile as the reference category, adjusting for the same multiple confounding factors mentioned above.
Sensitivity analyses were performed to test the robustness of the results in different scenarios. We repeated two Cox regression analyses, evaluating CH intake without applying the residual method and using only the percentage of energy intake as CH with respect to the other energy-providing macronutrients (fats and proteins). We conducted analysis stratifying by age (>55) and sex, including Willett’s et al. 21 energy limits, and excluding prevalent and incident Diabetes Mellitus and former and no-smokers. We used Cox regression models to estimate the risk of glaucoma associated with type 2 diabetes, after adjusting for multiple confounding factors. Finally we used Cox regression models to estimate the risk of glaucoma associated with total energy intake (quartiles), after adjusting for multiple confounding factors. All p values presented are two-tailed; p < 0.05 was considered statistically significant. Analyses were performed using STATA/SE 12.0.
The voluntary completion of the baseline questionnaire, once participants understood the specific information needed, was considered to imply informed consent. We informed the potential candidates of their right to refuse to participate in the SUN study or to withdraw their consent to participate at any time without reprisal, according to the principles of the Declaration of Helsinki. The Institutional Review Board of the University of Navarra approved this survey and methods.
Results
After a median of 10 years of follow-up and 183,067 person-years at risk, 242 new cases of glaucoma were reported (128 in men and 114 in women). The main baseline and demographic characteristics of participants (n:18,247) compared with participants not included in the final sample are shown in the online supplementary table. Participants characteristics at baseline according to quartiles of CH intake are summarized in Table 2. It should be noted that subjects in the highest quartile, practiced more physical activity and had a higher total energy intake, they smoked less and presented lower prevalences of diabetes and hypertension.
Baseline characteristics of participants by quartiles of energy-adjusted CH intake by residual method.

Values are expressed as means (SD), unless otherwise noted. (SUN project).
Participants in the highest quartile of CH intake showed a significantly higher risk of glaucoma compared to those in the lowest quartile, after controlling for potential confounding factors. [HR 1.50 (95% CI: 1.01–2.25); p for trend = 0.042] (Table 3).
Risk of glaucoma (HR and 95% confidence intervals) according to baseline consumption of energy-adjusted quartiles of carbohydrates intake by residuals method The SUN Project.

Q1–Q4: quartiles carbohydrate intake by residuals method.
Adjusted by adherence to Mediterranean diet, BMI, prevalence of cancer at baseline, cigarettes smoked per year, leisure-time physical activity, caffeine intake, alcohol intake, omega-3/omega-6 ratio, prevalence of systemic hypertension at baseline, prevalence of diabetes mellitus type 2 at baseline, educational level and year of completion of the baseline questionnaire.
Figure 2 shows the multivariable-adjusted HR of glaucoma across food sources of carbohydrates for each of the nine food groups. The vegetable group was inversely associated with the risk of glaucoma (HR 0.68; 95% CI: 0.47–1.00). No other CH group was significantly associated with glaucoma incidence. Sensitivity analyses (Table 4) showed how the risk of glaucoma was significantly increased in the highest quartile of CH intake, when analysed without using the residual method [HR 2.42 (95% CI: 1.27–4.62)]. The association was not significant when we used the percentage of CH intake as the main independent variable [HR highest vs lowest quartile of % of CH: 1.46 (95% CI: 0.97–2.19)]. The association of CH intake with the risk of glaucoma was statistically significant within the subgroups of women, younger participants (less than 55 years) and participants without type 2 diabetes. The prevalence of diabetes at baseline was associated with a higher incidence of glaucoma [HR, 2.12; 95% (IC, 1.26–3.57)]. Participants in the highest quartile of energy intake showed no significant association with the risk of developing glaucoma (HR 0.67; 95% CI: 0.36–1.24) when compared to participants in the lowest quartile, after controlling for multiple potential confounding factors.
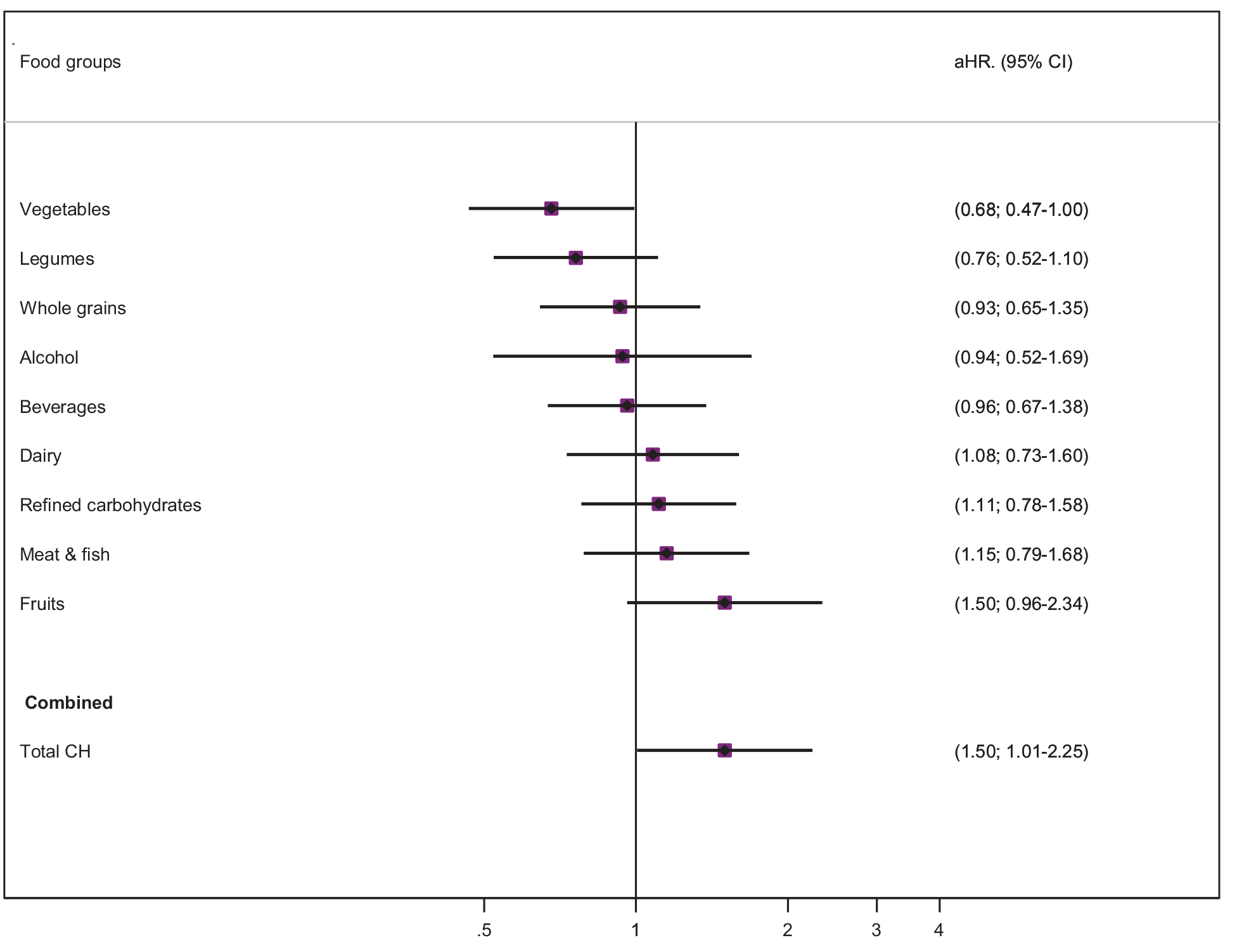
Hazard ratios* (95% Confidence Interval) for glaucoma incidence linked to the consumption of carbohydrates groups and the total intake in quartiles by residuals method. The SUN Project.
Sensitivity analyses exploring the association between highest intake of carbohydrates and risk of glaucoma.

HR (95% CI): Fourth quartile vs referent quartile.
Adjusted by energy intake but not use Residual method.
DM: Type 1, type 2, incident (before event of glaucoma) and prevalent diabetes mellitus.
Adjusted by: adherence to Mediterranean diet, BMI, prevalence of cancer at baseline, cigarettes smoked per year, leisure-time physical activity, caffeine intake, alcohol intake, omega-3/omega-6 ratio, prevalence of systemic hypertension at baseline, prevalence of diabetes mellitus type 2 at baseline, educational level and year of completion of the baseline questionnaire.
Discussion
This prospective follow-up study of young-middle-aged university graduates showed that a higher CH intake was associated with higher risk of glaucoma. This finding could be consistent with the biologically plausible hypothesis that increased CH intake increases the risk of diabetes, 23 and diabetes is likely to increase the risk of glaucoma. Although perhaps, and based in our findings, there may also be other alternative pathways linking CH intake with a higher glaucoma risk. The association between type 2 diabetes and glaucoma incidence remains controversial.15,24–26 In a recent meta-analysis including 2,981,342 individuals, Zhao et al. 15 found that both, diabetes and diabetes duration, were associated with a significantly higher risk of glaucoma [relative risk 1.48 (95% confidence interval, 1.29–1.71)]. However, the Rotterdam study that included 3837 participants without glaucoma, did not find any relationship between glaucoma and diabetes [odds ratio (OR) 0.82 (95% CI: 0.33–2.05)]. 27 Another study with a population of 6631 diabetic subjects and 166,144 non-diabetic subjects without glaucoma also failed to confirm an association between type 2 diabetes and primary open angle glaucoma. 25 In the current study we obtained a HR, 2.12 (95% IC: 1.26–3.57), indicating a strong relationship between diabetes and glaucoma. The inconsistency in results may be related to differences in age, selection criteria, race/ethnicity, follow-up time and definitions of risk factors and end points. 28
There are also some studies in which levels of fasting blood glucose has been directly associated with the glaucoma incidence.15,26,29 Higher long-term hyperglycaemia was related to higher intraocular pressure (IOP) in individuals without diabetes. 29 All these data suggest that blood glucose levels are associated with an elevated IOP and higher glaucoma incidence. The mechanisms relating hyperglycaemia and glaucoma are not clear. High glucose blood levels can interrupt the outflow of the trabecular meshwork. 29 Also the hyperglycaemia itself can induce an osmotic gradient, attracting excess aqueous humour toward the anterior chamber. 30 In a study with 943 subjects, Oh et al, suggested that insulin resistance might contribute to this potential explanation for the association between diabetes and high IOP. 31 These authors used the homeostasis model assessment for insulin resistance (HOMA-IR), and they found that the IOP was significantly associated with the degree of insulin resistance in non-diabetic individuals. 31 Fasting blood glucose and anterior chamber glucose levels may be related to CH intake. Insulin resistance may be one potential mechanism that may account for the association of CH intake with higher glaucoma risk in our study. Previous studies showed that total dietary CH also increased the risk of diabetes. 31 Therefore, Oba et al., 32 in a population based cohort study involving 27,769 men and 36,864 women, found that the dietary glycaemic load was positively associated with diabetes risk among women. In addition, dietary CH intake was also directly associated with the risk of type 2 diabetes among men with high total fat intake. Probably the insulin resistance is a potential mechanism that might produce glaucoma or diabetes in patients with sustained high CH intake. In our analysis the association between CH intake and glaucoma was calculated after adjusting for diabetes occurrence. In our sensitivity analyses we studied the relationship between CH intake and glaucoma eliminating all prevalent and incident cases of diabetes, to avoid possible cases of undiagnosed diabetes that followed the diagnosis of glaucoma. In this analysis we also observed an increased risk of glaucoma in subjects, with higher CH intake, who were free of diabetes [HR 1.77 (95% CI: 1.15–2.74)]. We also calculated the interaction between CH intake and diabetes and we did not find any suggestion of effect modification. Therefore, we cannot assure that the occurrence of diabetes may modify the effect of CH intake on the risk of glaucoma in our sample. On a similar way, diabetes is a well-known risk factor for cataract development, but a large prospective epidemiologic study described how this relationship did not seem to be mediated by CH intake or by a high dietary glycaemic load. 32 Other interesting studies analyse the advantages of caloric restriction and glaucoma. Caloric restriction has been reported to increase longevity and to have some benefits in different chronic diseases.33,34 Fasting is a form of caloric restriction and it has been shown in animals’ models to have neuroprotective effects. A recent study has shown that 7 weeks of alternate-day fasting suppresses retinal degeneration in a mouse model with normal-tension glaucoma. 35 According to Russo et al., 36 these neuroprotective effects of fasting might suggest that short-term dietary restriction could represent an aid in the treatment of glaucoma, where current topical treatments do not always halt the development of the disease.
When we individually analysed the effect of each CH grouped with the risk of glaucoma none of the nine CH-groups studied was significantly associated with glaucoma incidence. We did find that a higher vegetable intake was inversely associated with glaucoma (HR 0.68; 95% CI: 0.47–1.00), but not statistically significant differences were found.
These results support the findings previously published by Coleman et al., 37 where they also reported how consumption of green leafy vegetables, rich in nitrate, was associated with an approximately 20% lower risk of developing POAG, particularly POAG with early paracentral visual field loss, but they did not find any significant association between the other groups of nutrients analysed. But when we performed a risk calculation by progressively adding each group of foods, as CH intake increases (regardless of whether CH came from a food group that tended to be protective or not) the risk of glaucoma increases. This finding might indicate that the relationship that we found between CH intake and glaucoma is not based on the quality of the CHs but on the total amount of CH intake. The association seen between energy intake and glaucoma incidence was inverse, but not significant (HR: 0.67; 95% CI: 0.36–1.24). This suggests that the effect of CH consumption on glaucoma incidence was not mediated by a higher energetic value derived of a higher CH consumption, ant that the effect seen is probably mediated by a different pathway. Further studies are needed to better understand the physio-pathological pathways beneath this association.
Among the identified risk factors, intraocular pressure (IOP) is a major and modifiable ocular risk factor for glaucoma incidence.26,38 However the decrease the IOP requires topical or laser treatment or surgery. Other ocular risk factors, such as low corneal thickness, 39 or pseudoexfoliation, 40 or irregular corneal hysteresis 41 among others, are not modifiable. Systemic risk factors, such as diabetes, 15 age, 42 family history, 42 race/ethnicity, 2 are also not modifiable factors. Identifying potential modifiable risk factors, is therefore of great interest in order to reduce the burden of disease, and to promote primary prevention strategies. Smoking was also a modifiable risk factor in a previous report of the SUN cohort, specially in relationship with a high number of cumulative pack-years of smoking. 12 Similarly, several studies found a positive association between IOP and high systolic and diastolic blood pressure.43,44 On the other hand, low blood pressure, specially nocturnal hypotension, may also be a risk factor for developing glaucoma due to compromised perfusion pressure to the optic nerve.3,43,44 In this study, a new modifiable risk factor such as CH intake is suggested.
This study has important strengths. First it has a prospective design with a wide variety of potential confounders considered, avoiding the possibility of inverse causation bias, which is a frequent phenomenon in cross-sectional or case-control studies. Second, the diagnosis of glaucoma was validated in a subsample with high sensitivity and specificity. However, there are some limitations. First, some new-onset cases may have been missed, leading to a reduced sensitivity, which, in any case, will not affect the results. Second, the data were obtained from self-reported general questionnaires, not specifically intended to evaluate the systematic ophthalmological examination, and not able to differentiate the type of glaucoma. However, in the validated subsample of participants all glaucomatous cases were open-angle glaucoma. The basal prevalence of glaucoma in our sample was not high, as the SUN Cohort is mainly formed by middle-age, healthy university graduates, but the long follow-up period allowed to perform the analysis and to detect significant differences. Another possible limitation is that CH was assessed only at baseline and not subsequently updated. However, in our experience, dietary styles are generally not modified, except in cases of diet-related illnesses and potential changes in dietary habits during follow-up will only contribute to attenuate a true association. In addition, other risk factors for glaucoma such as obstructive sleep apnea or nocturnal hypotension were not assessed in these questionnaires. Despite these limitations, our cohort had a long follow-up period (mean 10 years) and a high retention rate (91.1%) and demonstrates the effect of CH intake on glaucoma incidence. Additional research is necessary before advising patients to change their dietary habits in order to prevent glaucoma, but physicians should consider promoting healthy lifestyles, quitting smoking, preventing hypertension and eating a moderated and balanced healthy diet, not limiting any specific food, but giving the recommendation of avoiding high CH intakes.
In conclusion, this study found a direct association between total CH intake and glaucoma incidence. This relationship seems not to be mediated or modified by diabetes, and has been analysed adjusting for multiple potential confounding factors. None of the nine groups of CH was a risk factor for glaucoma incidence when analysed individually. According to these findings, physicians should consider promoting a healthy diet, with special focus on avoiding high CH intake in patients with glaucoma risk factors. Further studies are needed to replicate our results in other cohorts and to better understand the mechanism by which CH intake might cause glaucoma.
Supplemental Material
sj-pdf-1-ejo-10.1177_11206721211012862 – Supplemental material for Carbohydrate intake and risk of glaucoma in the sun cohort
Supplemental material, sj-pdf-1-ejo-10.1177_11206721211012862 for Carbohydrate intake and risk of glaucoma in the sun cohort by Javier Moreno-Montañés, Itziar Gutierrez-Ruiz, Elsa Gándara, Laura Moreno-Galarraga, Susana Santiago, Miguel Ruiz-Canela, Julio Martínez-González, Miguel Ángel Martínez-González and Alejandro Fernandez-Montero in European Journal of Ophthalmology
Footnotes
Authors’ note
This submission has not been published anywhere previously and it is not simultaneously being considered for any other publication. This article was previously rejected in Clinical Nutrition and Public Health Nutrition. One of the editors suggested that we submit this article to a journal of Ophthalmology.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by Instituto de Salud Carlos III, “Red temática de Investigación Cooperativa, Proyecto RD07/0063. OftaRed: Patología ocular del envejecimiento, calidad visual y calidad de vida.” MAMG and MRC were supported by and Advanced Research Grant of the European Research Council (Agreement 340918). The SUN Project has received funding from the Spanish Government-Instituto de Salud Carlos III, the European Regional Development Fund (FEDER) (RD 06/0045, CIBER-OBN, Grants PI13/00615, PI10/02658, PI10/02293, PI13/00615, PI14/01668, PI14/01798, PI14/01764, PI17/01795 and G03/140), the Navarra Regional Government (27/2011, 45/2011, 122/2014), and the University of Navarra. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.