
Abstract
Purpose:
To evaluate the safety and efficacy of double compared to single intraluminal suture stenting in reducing early postoperative hypertensive spikes (HS) and hypotony after Baerveldt glaucoma implant surgery.
Methods:
For this retrospective study, we reviewed the medical charts of 60 patients (60 eyes) who underwent Baerveldt drainage device surgery between 2017 and 2019. Two groups were formed according to whether a single suture stent was placed within the tube (5-0 polypropylene, 30 eyes, group 1) or a double suture (5-0 and 6-0 polypropylene, 30 eyes, group 2). Intraocular pressure (IOP) was measured at baseline, at 6 h, and on postoperative days 1, 2, 5, 7, 14, 21, 30, 60, 90, 180. The occurrence of HS (IOP ⩾ 30 mmHg), anterior chamber reformation, decompressive paracentesis, anti-glaucoma medication, and adverse events were recorded.
Results:
There was a greater decrease in IOP from baseline at days 1, 2, and 21 (p < 0.05) and number of HS at 6 h (p = 0.006) and postoperative day 1 (p < 0.001) in group 2. The mean number of decompressive paracentesis, anterior chamber reformation procedures, and topical anti-glaucoma medications was the same in both groups; the need for oral acetazolamide was significantly lower in group 2 at days 1, 21, and 30 (p < 0.05).
Conclusions:
While both stenting methods provide a gradual, controlled decrease in IOP, the double stenting technique was associated with a sooner and greater postoperative reduction in IOP and a good safety profile thanks to fewer HS in the early postoperative period and less need for oral acetazolamide.
Keywords
Introduction
Glaucoma drainage devices (GDDs) have been shown to lower intraocular pressure (IOP); they are mainly indicated after unsuccessful filtrating surgery or in patients with high risk of failure after conventional surgery. 1 Postoperative complications after uneventful GDD implantation include corneal endothelial damage, hypotony, conjunctival erosion, strabismus, and infection. 2 A major difference in design between tube shunts is the presence or absence of a flow restrictor that acts as a valve. The Baerveldt implant is a non-valved GDD composed of a silicone tube connected to a silicone plate different in surface area. The tube shunts the aqueous humor from the intraocular space (anterior/posterior chamber or vitreous chamber) to an encapsulated space surrounding the plate outside the scleral surface, where it can diffuse into the fibrous walls of the bleb. 3 In non-valved GDDs, long-term pressure control is provided by fibrovascular encapsulation of the episcleral plate, which resists aqueous flow and prevents hypotony. Because encapsulation may take several weeks to develop, temporary restriction of aqueous flow is necessary at the time of surgery to prevent serious early hypotony-related complications such as choroidal detachment and suprachoroidal hemorrhage. 4 This can be achieved with either intraluminal tube suture stenting 5 or external constriction. Internal sutures can be removed later if hypertension develops, whereas external tube ligation either undergoes spontaneous release or requires suture lysis.
A consequence of these non-valved GDD modifications is that hypertension can develop, for which topical anti-glaucoma drug therapy or oral acetazolamide therapy and decompression via a pre-existing corneal paracentesis are usually performed. Hypertensive spikes in patients with a compromised optic disc can have a deleterious effect on the remaining nerve fibers and result in further visual field loss.6,7 Strategies to obtain a desirable postoperative IOP include two-stage implantation, 8 not-occlusive ligature and fenestration9,10 with and without antimetabolites, 11 and suture stenting of tube fenestration. 12 These modifications have certain disadvantages: the two-stage technique is associated with an interval of uncontrolled pressure, and fenestration carries the risk of fibrotic tissue overgrowth, ensuing in blockage and increased IOP. 11 Here we describe a novel approach that employs internal non-absorbable suture stenting and an external absorbable ligature, in partial modification to our standard Baerveldt implant surgery technique. 13 Our hypothesis was that the different sized internal sutures would create an internal space between the two ripcords and the external constriction, thus allowing for greater aqueous outflow compared to a single suture and reduce the occurrence of hypertension spikes, without inducing hypotony during the early postoperative period.
Methods
Study design and patients
This retrospective, observational study was performed following the ethical standards of the Declaration of Helsinki. Ethical Committee Board approval was not needed. Written consent was obtained from each patient before surgery.
We retrospectively reviewed the charts of 60 consecutive patients: 30 underwent unilateral Baerveldt 350-mm2 implantation with a single 5-0 polypropylene intraluminal suture (group 1) and 30 underwent unilateral Baerveldt 350-mm2 implantation via a modified technique with double 5-0 + 6-0 polypropylene intraluminal sutures (group 2). All surgeries were performed by glaucoma specialists (GM and RT). The Baerveldt GDD (Johnson & Johnson Surgical Vision inc., Santa Ana, CA, USA) is a non-valved 32-mm silicone tube (external diameter 0.63 mm, bore 0.30 mm) attached to a medical-grade silicone 350 mm2 plate with four fenestrations.
Surgical technique
All patients received Baerveldt surgical implantation under general anesthesia. A limbus-based conjunctival incision was made at 11–12 mm from the limbus: 12
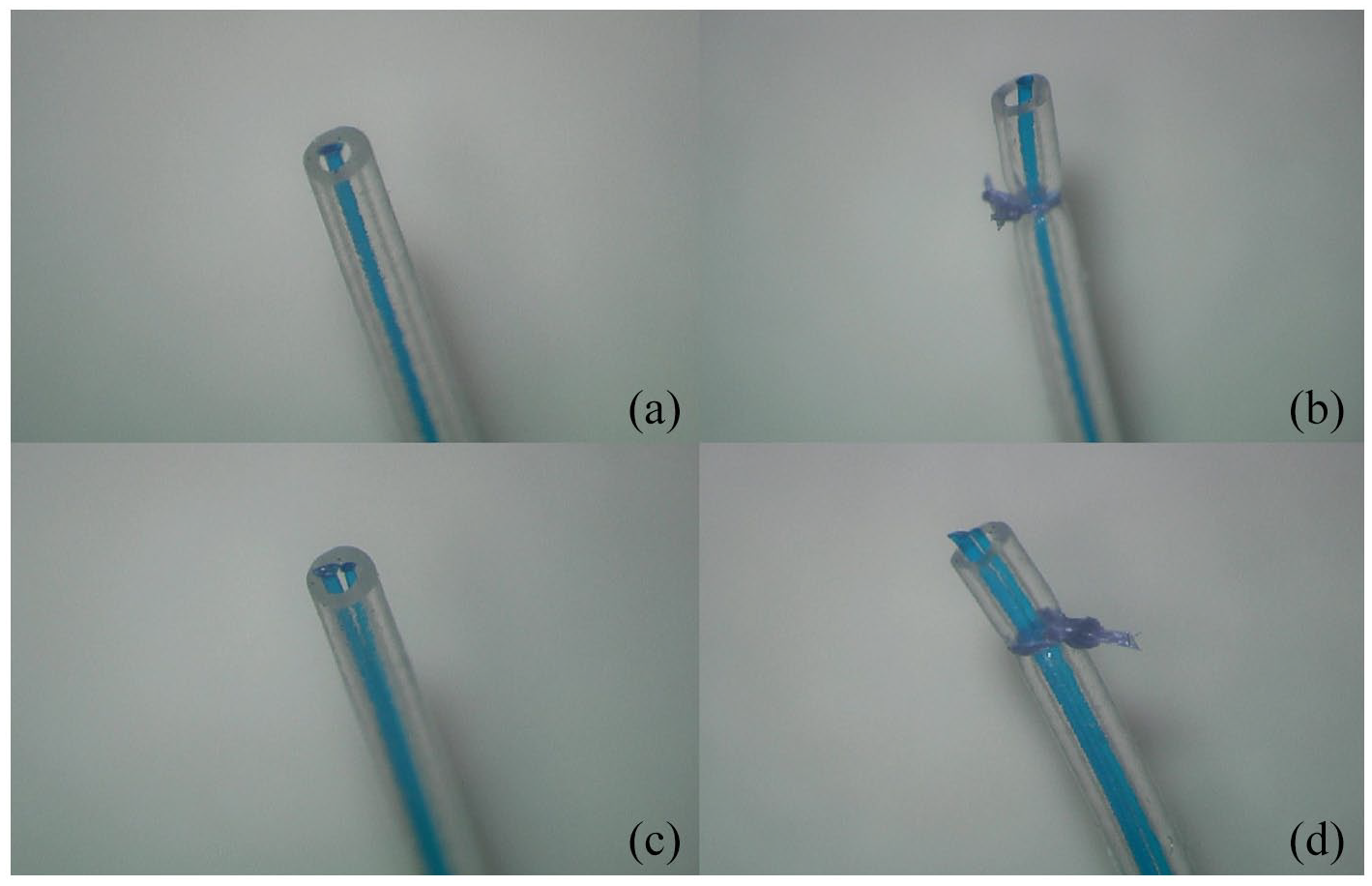
The bore of the non-valved GDD tube is routinely occluded during surgery to prevent excess aqueous flow during the early postoperative period. This was obtained with a single intraluminal, not absorbable suture (a) and an external absorbable suture (b) in group 1; a double intraluminal suture (c) and the same occluding external suture (d) in group 2.
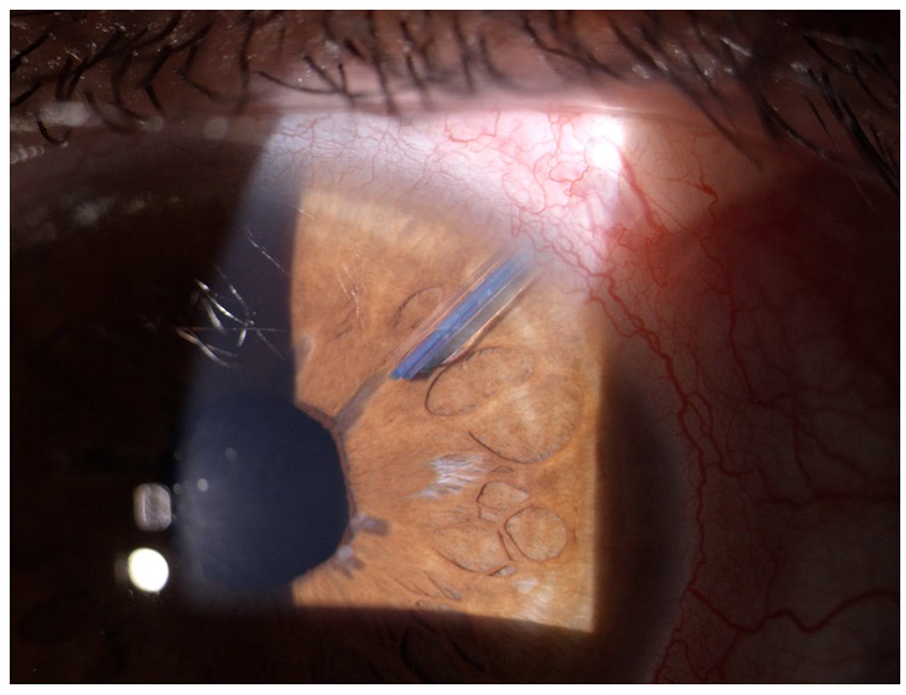
Double stented tube within the anterior chamber 30 days after surgery.
Outcome measurements
Preoperative data included: age, sex, eye laterality, glaucoma diagnosis, number of anti-glaucoma drugs, and baseline IOP. Postoperative IOP, number of hypertensive spikes, number of anti-glaucoma medications and anterior chamber reformation/decompressive procedures, number of acetazolamide tablets, and complications rate were recorded at 6 h and then at 1, 2, 5 ± 1, 7 ± 1, 14 ± 3, 21 ± 3, 30 ± 6, 60 ± 8, 90 ± 7, 180 ± 10 days after surgery. Anti-glaucoma medications were adjusted according to the patient’s glaucoma status, with the addition of beta-blockers (BBs), topical carbonic anhydrase inhibitors (CAIs), and oral acetazolamide.
Pressure peak was defined as an IOP ⩾30 mmHg. The number of patients needing ripcord suture removal and the mean time to removal were recorded. Single and double ripcord removal was performed if IOP was ⩾18 mmHg despite medical therapy (BBs + CAIs + 500 mg oral acetazolamide) at two consecutive follow-up visits.
Statistical analysis
Statistical analysis was performed with PSPP software for Windows (version 1.2.0, GNU, Free Software Foundation). Descriptive statistics, independent sample t-test, and chi-square test were employed. Parametric results are reported as mean ± standard deviation. Statistical significance was set at p < 0.05.
Results
We reviewed the medical charts of 60 consecutive patients who underwent glaucoma surgery at our clinic between March 2017 and August 2019 and were clinically followed for at least 6 months. Demographics were equally distributed between the two groups (Table 1). Table 1 presents the types of glaucoma in the study sample.
Demographics, descriptive analysis of the study sample, and types of glaucoma.

OAG: open-angle glaucoma; ACG: angle-closure glaucoma; ICE: iridocorneal endothelial syndrome; PEX: pseudoexfoliation; PKP: penetrating keratoplasty.
Baerveldt implant was the first glaucoma surgery in 15 (50%) group 1 (single suture) patients; previous trabeculectomy in 11 (37%), and deep sclerectomy in 4 (13%). Primary tube shunt was recorded for 18 (60%) group 2 (double stent) patients; previous trabeculectomy in 7 (23%), and deep sclerectomy in 5 (17%). The IOP was significantly lower in group 2 at day 1 (p = 0.04), day 2 (p = 0.04), and day 21 (p = 0.003) but higher at day 90 (p = 0.003) (Figure 3). The number of topical medications was the same in both groups (Figure 4); fewer acetazolamide tablets were needed to control IOP in group 2 at day 1 (p = 0.001), day 21 (p = 0.04), and day 30 (p = 0.04) (Figure 5).

Intraocular pressure (IOP) variations in the two groups during the first 6 months of follow-up.

Number of topical antiglaucoma medications during the first 6 months of follow-up.

Number of acetazolamide oral tablets (1 tablet = 250 mg) during the first 6 months of follow-up.
Hypertensive spikes were recorded in 12 (40%) group 1 patients and 7 (23%) group 2 patients (p = 0.006) at 6 h after surgery and then in 8 (27%) group 1 patients and 0 (0%) group 2 patients at 1 day (p < 0.001) (Figure 6). At least one episode of hypertensive spikes (IOP ⩾ 30 mmHg) occurred in 14 group 1 patients and in 7 group 2 patients during the follow-up period (p = 0.05).

Number of patients with hypertensive spikes recorded at each follow-up visit. No hypertension spikes were recorded for the double suture stenting group on days 1, 7, 21, and 60 days after surgery.
Anterior chamber reformation with the viscoelastic solution was needed in 13 (43%) in group 1 patients and in 9 (30%) group 2 patients (p = 0.59): 0.96 ± 1.43 in group 1 and 0.70 ± 1.23 in group 2, respectively (p = 0.48). Decompressive actions were performed in 11 (37%) group 1 patients and in 7 group 2 patients (23%) (p = 0.56): mean paracenteses 0.73 ± 1.28 in group 1 and 0.37 ± 0.69 in group 2 (p = 0.21).
Removal of the 5-0 and the 6-0 polypropylene suture was necessary in 11 (33%) group 2 patients; removal of the single 5-0 polypropylene suture was necessary in 7 (30%) group 1 patients (p = 0.26). The mean time to suture removal was 70.2 ± 39.6 days for group 2 and 71.7 ± 65.1 days for group 1 (p = 0.95). One patient in group 1 and 2 patients in group 2 required ripcord removal during the first postoperative month. Mild, self-limiting choroidal detachment (n = 7, 23%) was noted in each group (p > 0.05), cystic macular edema (n = 2, 7%) in both groups (p > 0.05), corneal edema (n = 3, 10%) in group 1 and (n = 1, 3%) in group 2 (p = 0.03). One case (3%) of mild vitreous hemorrhage in group 1 (p > 0.05) resolved spontaneously.
Discussion
Treatment of early postoperative ocular hypotony and hypertension after Baerveldt implantation remains challenging. Hypotony can lead to choroidal detachment and visual loss
14
and hypertensive peaks in glaucoma patients can cause apoptosis of retinal neural cells.
6
Efforts to limit this risk include the development of multiple surgical techniques for non-valved tube shunts. Ideally, the goal of modification is to restrict flow and prevent early hypotony but still allow some egress of aqueous to ensure reduction in early intraocular pressure.
A major advantage of using a stent technique in addition to external obstruction is the predictability of removing tube resistance to flow. However,
While there was no statistically significant difference in the number of anterior chamber reformation and decompressive procedures between the two groups, fewer interventions were necessary in the double suture stenting group. A larger study sample might be able to reveal clinically relevant differences between the groups. The number of hypertensive spikes in the double suture stenting group (Figure 6) was significantly lower in the immediate postoperative period (6 h and 1 day after surgery) when the IOP peaks in both groups were more frequent. Starting from day 2 the occurrence of hypertensive spikes diminished and was the same in the two groups. Optimal postoperative pressure control was achieved in the double suture stenting group, which is desirable in glaucoma patients since fluctuating IOP leads to neuronal cell loss. 1 Furthermore, significantly fewer group 2 patients experienced hypertension peaks, with fewer requiring treatment adjustment. Short-term control of hypertension spikes can be achieved with oral acetazolamide therapy. While there were no differences in the number of medications between the groups during the follow-up period, the number of acetazolamide tablets at days 1, 21, and 30 after surgery was lower in group 2.
Suture removal was performed in 33% of group 2 and in 30% of group 1 patients at around 3 months after surgery. There was no statistically significant difference between the groups. This percentage correlates with bleb encapsulation in the late hypertensive phase after Baerveldt implantation; 15 our data show that use of a double internal suture does not influence this phenomenon. The modified technique is safe, as demonstrated by the similar complication rates for the two groups during the follow-up period. Hypotony-related complications were infrequent and resolved with an in-office intervention (e.g. reformation of the anterior chamber with a viscoelastic solution). Finally, our data show that the double suture technique is effective in lowering IOP spikes during the early postoperative period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.